- 35 -
Endoscopic Diagnosis and Treatment of Isolated Sphenoid Sinus Lesions
Kyung-Chul Lee, M.D.
ABSTRACT
Isolated sphenoid sinus disease is a rare entity. Because of its close vicinity to important and vulnerable structures of the skull base, early diagnosis and treatments are needed. We aimed to characterize the clinical features of isolated sphenoid sinus lesions and to assess the outcome of endoscopic sphenoid sinus surgery. We reviewed the records of patients retrospectively from July 1994 to May 2004. 17 cases with disease of the isolated sphenoid sinus that has undergone endoscopic sinus surgery were studied. The pathology spectrum included 7 cases of isolated chronic sphenoid sinusitis, 4 fungal sinusitis, 2 mucoceles, 1 inverted papilloma, 3 malignant tumors. Except 3 cases of malignant tumors, 14 cases were cured by endoscopic sinus surgery without complication. Diagnostic nasal endoscopy procedures and imaging techniques are of great value for an early and precise diagnosis. Endoscopic sphenoid sinus surgery is safe and effective for treating isolated sphenoid sinus lesions.
KEY WORDS:Sphenoid sinus・Endoscopy.
INTRODUCTION
The sphenoid sinus is located in an isolated an- atomical location where approach is difficult. It is also easy to be clinically overlooked for sinusitis localized in the sphenoid sinus is rare and the symptoms are not so obvious.1) However, because of its close vicinity to important and vulnerable structures such as the middle cranial fossa, optic nerve, internal carotid artery, pi- tuitary gland and cavernous sinus, fatal complications may be induced. Therefore, early diagnosis and treat- ment is necessary.2)
The most common symptom is headache. But sym- ptoms such as cranial nerve palsy including visual dis- turbance, postnasal drip, nasal obstruction, rhinorrhea, etc. can be present. However, nasal symptoms are non-
specific and relatively rare. Therefore, diagnosis of isolated lesions of the sphenoid sinus is difficult.3)4) Nasal endoscopy and radiologic evaluation methods such as computed tomography are the most useful methods used for early and accurate diagnosis of such lesions.2)5) Also, it can be treated safely and effectively by approaching the sphenoid sinus with endoscopic sinus surgery.6-8)
This study reports the symptoms, evaluation and cause of 17 cases of patients who had enodoscopic di- agnosis and treatment out of 21 cases who were diag- nosed with isolated sphenoid sinus lesion, and also dictated about enodoscopic sinus surgery and its treat- ment outcomes considering other documents.
MATERIALS AND METHODS
This study is based on 17 patients among 21 patients diagnosed with isolated sphenoid sinus lesion from July 1994 through May 2004 at the department of Oto- rhinolaryngology Head and Neck surgery who have undergone nasal endoscopy. Four patients who have undergone conservative treatment such as antibiotics treatment have been excluded. Diagnosis was made by nasal endoscopy and computed tomography in all patients and was limited to only isolated lesions of the Department of Otolaryngology Head and Neck Surgery, Kang-
buk Samsung Hospital, School of Medicine, Sungkyunkwan Uni- versity, Seoul, Korea
Address correspondences and reprint requests to Kyung-Chul Lee, M.D., Department of Otolaryngology Head and Neck Sur- gery, College of Medicine, Sungkyunkwan University, Kangbuk Samsung Hospital, 108 Pyong-dong, Jongno-gu, Seoul 110-746, Korea
Tel:82-2-2001-2268, Fax:82-2-2001-2273 E-mail:[email protected]
Accepted for publication on July 30, 2004
sphenoid sinus. Lesions of other sinuses have been ex- cluded. Tumors of adjacent structures have also been excluded. A brain magnetic resonance imaging was also carried out in 14 cases.
A retrospective analysis of symptoms, radiologic findings, treatment such as endoscopic sinus surgery, cause and postoperative follow up was carried out through study of charts.
RESULTS
Among the patients that have been diagnosed with isolated sphenoid sinus lesion, 17 patients that have undergone an endoscopic sinus surgery have been analyzed (Table 1). There were 10 male and 7 female patients between the ages 16 and 73 years old. The mean age was 43.9 years old.
The causes of isolated sphenoid sinus lesion were inflammatory disease in 13 cases, chronic sphenoid si- nusitis in 7 cases, fungal sphenoid sinusitis in 4 cases and mucocele in 2 cases. All 4 cases of fungal sphe- noid sinusitis were aspergillosis. There were 3 cases of malignant tumors and the other 1 case was inverted papilloma that underwent endoscopic sinus surgery. A specific analysis of the cause of inflammatory diseases revealed that a nasal polyp of the sphenoid sinus caused
sphenoid sinusitis in 4 cases and in 2 cases an endo- scopic sinus surgery carried out under the suspicion of chronic sphenoid sinusitis exposed a fungal ball of the sphenoid sinus ostium that induced sinusitis that was diagnosed as sphenoid fungal sinusitis.
During the diagnosis process, 9 cases were trans- ferred to our department after visiting the neurology or neurosurgery department first with a headache, where they had taken Brain magnetic resonance imaging which identified sphenoid sinusitis. 1 case visited the ophthalmology department with exophthalmos, but was transferred to our department after a soft tissue density of the sphenoid sinus was revealed through a computed tomography that was carried out after admittance.
The chief complaints at the time of admittance were headache in 11 cases, cranial nerve palsy including visual disturbance in 3 cases, dizziness in 2 cases and postnasal drip in 1 case. Headache was the most co- mmon symptom complained by all 14 patients that diversely occurred in numerous regions such as the vertex, frontal region, temporal region, occipital region and so forth. However, there were no specific findings.
There were 5 cases with cranial nerve palsies. 3 cases had diplopia regarding to cranial nerve VI deficiencies.
1 case with cranial nerve III deficiencies. And 1 case with visual loss caused by cranial nerve II. 1 case
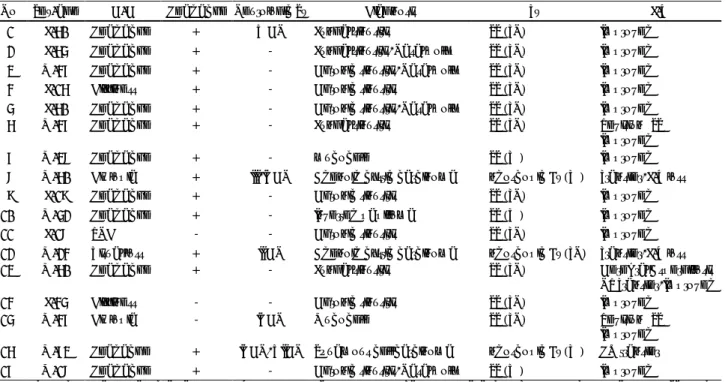
Table 1. Summary of 17 cases of lsolated sphenoid sinus lesions
No Sex/age C/C Headache Neurologic Sx Diagnosis Tx F/U
11 F/60 Headache + V CN Fungal sinusitis ESS (TN) Improved
12 F/65 Headache + - Fungal sinusitis, Nasal polyp ESS (TN) Improved
13 M/47 Headache + - Chronic sinusitis, Nasal polyp ESS (TN) Improved
14 F/16 Dizziness + - Chronic sinusitis ESS (TN) Improved
15 F/60 Headache + - Chronic sinusitis, Nasal polyp ESS (TN) Improved
16 M/47 Headache + - Fungal sinusitis ESS (TN) Revision ESS
Improved
17 M/38 Headache + - mucocele ESS (TE) Improved
18 M/60 Diplopia + III, IVCN Adenoid cystic carcinoma Endoscopic Bx (TE) Transfer, F/U loss
19 F/19 Headache + - Chronic sinusitis ESS (TN) Improved
10 M/52 Headache + - Inverted papilloma ESS (TE) Improved
11 F/18 PND - - Chronic sinusitis ESS (TN) Improved
12 M/24 Visual loss + II CN Adenoid cystic carcinoma Endoscopic Bx (TN) Transfer, F/U loss
13 M/60 Headache + - Fungal sinusitis ESS (TN) Cerebral Aspergillosis
NR Transfer, Improved
14 F/45 Dizziness - - Chronic sinusitis ESS (TN) Improved
15 M/47 Diplopia - IVCN Mucocele ESS (TN) Revision ESS
Improved 16 M/73 Headache + IVCN, VIICN Squamous cell carcinoma Endoscopic Bx (TE) HO transfer 17 M/18 Headache + - Chronic sinusitis, Nasal polyp ESS (TE) Improved
C/C:chief complaint, CN:cranial nerve, F/U:follow up, Sx.:symptoms, PND:postnasal drip, Tx:method of treatment, ESS:Endo- scopic sinus surgery, Bx:Biopsy, NR:Neurology, HO:Hemato-Oncology, TN:Transnasal approach, TE:Transethmoid approach
showed facial nerve palsy of cranial nerve VII and in 1 case patient apealed facial paresthesia consitent with cranial nerve V defeciencies. Other symptoms include dizziness, postnasal drip, nasal obstruction, throat dis- comfort and so forth. However, there were only 4 pa- tients that complained of nasal symptoms. An endo- scopic sinus surgery was carried out in all 17 patients for treatment. Surgery was carried out under general anesthesia in 3 patients and local anesthesia in 14 patients. Among all cases, 3 cases that were malignant tumors underwent endoscopic sinus surgery merely for biopsy where 1 was diagnosed as squamous cell car- cinoma and 2 as adenoid cystic carcinoma.
Excluding the 3 cases of malignant tumors, all 12 patients showed improvement of symptoms, however, two patients underwent a revision endoscopic sinus surgery due to stenosis of the sphenoid sinus ostium.
The mean follow up period was 10 months. A com- plication of cerebral aspergillosis occurred in 1 case that was diagnosed as sphenoid fungal sinusitis and 2 patients were transferred to a different hospital and were follow up loss.
DISCUSSION
Isolated sphenoid sinus lesion is a rare entity that takes up 2-3% of all sinus diseases.9) Wyllie et al., reported 45 patients that were diagnosed with isolated sphenoid sinus lesion within a 37 year period.10) Lew et al., stated that it takes up 2.7% of all sinus di- seases.11) Domestically, Dhong et al., reported a fre- quency of less than 1%.12) However, due to develop- ment of radiologic evaluations and use of nasal endo- scope, its frequency is gradually increasing.6)13)
In this study, the frequency was low with 0.7%, of which was 17 patients diagnosed with isolated sphenoid sinus lesion among 2427 patients that underwent endo- sopic sinus surgery due to sinus diseases within a 10 year study period.
The most common symptom in isolated sphenoid sinus disease was headache which took up about 60- 90% of all symptoms.12)14)15) The pathophysiology of headache is explained by the following;the sphenoid sinus mucosa receives nerve innvervation through the first segment of cranial nerve V and sensory nerve of the sphenopalatine ganglion.12) Headache can diversely occurr in numerous locations such as the vertex, frontal
region, temporal region, occipital region and so forth.
There was a difference in frequency according to lo- cation of the headache, depending on each reference, therefore there was no specific finding.1)14)15) In this study, 14 out of 17 patients complained of having a headache, which showed a 82% frequency that re- vealed similar result with other studies.
The second most common symptom was visual dis- turbance. 4 patients (24%) showed visual disturbance symptoms such as decreased visual acuity or diplopia, or blurred vision and so forth. Visual disturbance was noticed in 1 out of 13 patients with inflammatory di- seases and in all 3 malignant tumor patients. 20-45%
of all isolated sphenoid sinus lesion patients showed visual disturbance,2)4)15) and it has been stated that the cause of visual disturbance was cranial nerve palsy of nerves II, III, IV, and VI.5)9) Additionally, there were diverse symptoms such as facial paresthesia due to cranial nerve palsy, rhinorrhea, nasal obstruction, pos- tnasal drip, dizziness and so forth. However, they were all nonspecific symptoms.
In many cases early diagnosis of isolated sphenoid sinus lesion is difficult because the sphenoid sinus is located in the center of the nasal cavity and has non- specific symptoms with rare nasal symptoms.2)4) Nasal endoscopic examination and computed tomography are the most useful and necessary methods for diag- nosis.2)5)
Computed tomography must absolutely be carried out in patients who are under suspicion of isolated sphenoid sinus lesion for it shows the location of the lesion and degree of progress and also confirms dehi- scence of the sphenoid sinus wall.14) Bone erosion su- ggests variable pathologic findings including malignant neoplasm. Brain magnetic resonance imaging should be additionally carried out when bone erosion is found on CT, when a tumor or mucocele has spread outside of the sphenoid sinus, when intracranial involvement is suspected, when patients complain of visual disturbance or when patients have findings of cerebral palsy fin- dings.5)14)
Nasal endoscopy is important in evaluating patients with sphenoid sinus diseases and it generally reveals consistent results with radiologic findings. A nasal endoscopy can confirm rhinorrhea of the sphenoid sinus ostium or sphenoethmoidal recess and obtain microbi- ologic culture and it can also disclose whether or not
the lesion has spread to the sphenoid sinus anterior wall or ostium.2)5) It can also observe the sphenoeth- moidal recess and in case there is a protrusion of this area, inflammatory disease, tumorous lesion or malig- nant tumorous lesion findings can be confirmed for assistance in diagnosis.5) In case of CSF rhinorrhea, the location of the lesion can also be detected.5) How- ever, nasal endoscopic findings do not always consist with radiologic findings. In this study, among 9 pa- tients that were under suspicion of chronic sphenoid sinusitis followed by a radiologic evaluation that re- vealed soft tissue density of the sphenoid sinus, a nasal polyp was discovered in the sphenoid sinus ostium and sphenoethmoidal recess during endoscopic sinus sur- gery in 4 patients and a fungal ball was observed in 2 patients. Therefore, computed tomography and nasal endoscopy must always be performed at the same time.
For the treatment of sphenoid sinusitis, a broad spe- ctrum intravenous antibiotic treatment is effective for acute sphenoid sinusitis.4)15) However, surgery is ne- cessary when symptoms do not improve or worsen after 24-48 hours after antibiotic treatment, when chronic sphenoid sinusitis is suspected with symptoms lasting longer than one month, when fungal sphenoid sinusitis is suspected, when complications such as cranial nerve deficiencies develop or when malignant neoplasm is suspected6)7) Endoscopic sinus surgery is an effective and safe method to approach the sphenoid sinus and it also possesses the merits of causing less bleeding, shortening the admission days and operation time and decreasing morbidity.5-7)
Sphenoid sinus surgery using a nasal endoscope can be carried out by a transnasal approach between the middle turbinate and nasal septum and a transethmoid approach.7)8)16) The transnasal approach passes between the superior turbinate of the posterior of the middle turbinate and the nasal septum and passes through the sphenoethmoidal recess and approaches the sphenoid ostium.5)7)16) In case of middle turbinate hypertrophy or when the passage is too narrow, a portion of the anterior middle turbinate or the superior turbinate can be resected for convenient approach. Careful consider- ation must be inclined toward the important structures of the orbit and skull base in order to prevent com- plications and to carry out a safe and effective oper- ation.7)8) A transethmoidal approach is effective when an anatomical abnormality such as nasal septal devi-
ation is present and transnasal approach is difficult or when there is a lesion in the ethmoid sinus.5)7)16) In this study, a transnasal approach was carried out in 12 cases and a transethmoid approach in 5 cases.
When treatment is delayed for sphenoid sinus disease, serious complications may occur.11) In this study, cere- bral asperigillosis developed in 1 case and all 3 cases of malignant tumors were diagnosed when the disease has already invaded surrounding structures which made surgery impossible.
The postoperative follow up period was between 6 months and 64 months with an average follow up period of 10 months. Stenosis of the sphenoid sinus occurred in 2 cases causing recurrence of symptoms and underwent revision endoscopic sinus surgery and were cured. Good results can be obtained if diagnosed at an early stage and if appropriately treated with me- dical treatment and endoscopic sinus surgery.7) In this study, all cases including 13 cases of inflammatory diseases, 1 case of inverted papilloma and 2 cases that underwent revision endoscopic sinus surgery, showed improvement of symptoms.
CONCLUSION
Isolated sphenoid sinus lesion is a rare entity with nonspecific symptoms in most cases. Headache and visual disturbance are common symptoms but are non- specific and nasal symptoms rarely occur. Therefore, it is important to fully understand the symptoms and characteristics of isolated sphenoid sinus lesions and when suspected careful history taking, physical exami- nation along with radiologic evaluations such as com- puted tomography and confirmation of the sphenoeth- moidal recess and sphenoid ostium through a nasal endoscopy must be carried out. Early diagnosis and treatment is important and we believe that endoscopic sinus surgery is an effective treatment modality that can minimize complications and injury of the surroun- ding structures of the orbit and skull base.
REFERENCES
1) Cakmak O, Shohet MR, Kern EB. Isolated sphenoid sinus lesions.
Am J Rhinol 2000;14:13-9.
2) Martin TJ, Smith TL, Smith MM, Loehrl TA. Evaluation and sur- gical management of isolated sphenoid sinus disease. Arch Oto- laryngol Head Neck Surg 2002;128:1413-9.
3) Pearlman SJ, Lawson W, Biller HF, Friedman WH, Potter GD.
Isolated sphenoid sinus disease. Laryngoscope 1989;99:716-20.
4) Ruoppi P, Seppa J, Pukkila M, Nuutinen J. Isolated sphenoid sinus diseases: report of 39 cases. Arch Otolaryngol Head Neck Surg 2000;126:777-81.
5) Grillone GA, Kasznica P. Isolated sphenoid sinus disease. Oto- laryngol Clin North Am 2004;37:435-51.
6) Gilain L, Aidan D, Coste A, Peynegre R. Functional endoscopic sinus surgery for isolated sphenoid sinus disease. Head Neck 1994;
16:433-7.
7) Castelnuovo P, Pagella F, Semino L, De Bernardi F, Delu G. Endo- scopic treatment of the isolated sphenoid sinus lesions. Eur Arch Otorhinolaryngol 2004;2:1-10.
8) Kieff DA, Busaba N. Treatment of isolated sphenoid sinus inflam- matory disease by endoscopic sphenoidotomy without ethmoide - ctomy. Laryngoscope 2002;112:2186-8.
9) Goldman GE, Fontanarosa PB, Anderson JM. Isolated sphenoid
sinusitis. Am J Emerg 1993;11:235-8.
10) Wyllie JW, Kern EB, Djalilian M. Isolated sphenoid sinus lesions.
Laryngoscope 1973;83:1252-65.
11) Lew D, Southwick FS, Montgomery WW, Weger AL, Baker AS.
Sphenoid sinusitis: a review of 30 cases. New Eng J Med 1983;309:
1149-54.
12) Dhong HJ, Chung SK, Koh SJ. Isolated sphenoid sinus disease.
Korean J Otolaryngol 1998;41:467-70.
13) Rosen FS, Sinha UK, Rice DH. Endoscopic surgical management of sphenoid sinus disease. Laryngoscope 1999;109:1601-6.
14) Lawson W, Reino AJ. Isolated sphenoid sinus disease: an analysis of 132 cases. Laryngoscope 1997;107:1590-5.
15) Lee JR, Song SH, Kim HW, Kim JS. Isolated sphenoid sinus lesion: A clinical analysis of 17 cases. Korean J Otolaryngol 1998;
41:467-70.
16) Metson R, Gliklich RE. Endoscopic treatment of sphenoid sinusitis.
Otolaryngol Head Neck Surg 1996;114:736-44.