J Rhinol 20(1), 2013
- 37 -
A Clinical Analysis of Revision Endoscopic Sinus Surgery:
Single-Center 10-Year Experience
Boo-Young Kim, MD, Min Kim, MD, Jung Mee Park, MD, Hyun Bum Kim, MD, Sung Won Kim, MD, PhD, Byung-Guk Kim, MD, PhD, Jin Hee Cho, MD, PhD,
YongJin Park, MD, PhD and Soo Whan Kim, MD, PhD
Department of Otolaryngology-Head and Neck Surgery, The Catholic University of Korea, College of Medicine, Seoul, Korea
ABSTRACT
Background and Objectives : Endoscopic sinus surgery (ESS) has become a popular procedure for treating chronic sinusitis. Despite recent developments in medical and surgical techniques, primary ESS can still fail. Al- though revision ESS is one solution to the problem of recurrent sinusitis, revision surgery is stressful for patients and otolaryngologists. Therefore, we examined the causes of ESS failure and sought to find ways to prevent the failure of primary ESS. Materials and Methods : All patients who underwent revision ESS in our department between April 2003 and March 2012 were studied retrospectively. Results : During this period, revision ESS was performed 40 times to treat chronic sinusitis. We analyzed the preoperative computed tomographic (CT) findings of primary and revision ESS cases using the Lund-Mackay and Kennedy CT staging scores to compare disease severity. In our cases, the failure of ESS was not affected by the extent of disease, asthma, or allergy. Polyposis was the only useful predictor of revision ESS. Conclusion : Polyposis is an important predictor of revision ESS.
We recommend that patients be followed frequently and carefully, especially those with polyps.
KEY WORDS : Revision Endoscopic S inus Surgery · Nasal Polyps · Asthma.
INTRODUCTION
Recently, endoscopic sinus surgery (ESS) has become a popular procedure for treating chronic sinusitis.
1)Despite recent developments in medical and surgical techniques, the failure rate of primary ESS is still 2–24%.
2) 3)In cases of failed ESS, revision ESS is one solution to the problem of recurrent sinusitis. This study reports our experience with the causes and characteristics of revision ESS sta- tistically.
MATERIALS AND METHODS
We retrospectively reviewed 60 primary and 40 revision ESS cases seen in our department between April 2003
and March 2012. During the same period, 690 patients underwent primary ESS for chronic sinusitis in our de- partment. Of these, 60 patients were followed for a mean of 40 months with no recurrent chronic sinusitis. In the revision ESS cases, the mean interval between primary and revision surgery was 15 (range 3–49) years. In the control group, patients who underwent primary ESS had not experienced recurrent chronic sinusitis for a mean of 40 (range 9–105) months.
Exclusion criteria were: benign or malignant tumor; post- operative cheek cysts; sinus surgery for complications of sinusitis; the Caldwell-Luc operation; and immunodefi- ciency or depressed immune status.
Recurrent chronic sinusitis was diagnosed based on an of- fice endoscopic examination and radiologic findings. ESS was indicated for patients in whom optimal medical treat- ment had failed. In our cases, “failure of medical treat- ment” was defined as unsatisfactory results after repeated, appropriate antibiotic therapy with local treatment, such as saline irrigation or nasal spray, for at least 6 months.
We analyzed the preoperative computed tomographic (CT) findings of primary and revision ESS cases using the www.ksrhino.or.kr
Address correspondence and reprint requests to Soo Whan Kim, MD, PhD, Department of Otolaryngology-Head and Neck Surgery, Seoul St.
Mary’s Hospital, College of Medicine, The Catholic University of Korea, 505 Banpo-dong, Seocho-gu, Seoul, 137-701, Korea
Tel: +82-2-2258-6214 , Fax: +82-2 -535-1354 E-mail: [email protected]
Received for publication on February 5, 2013
Accepted for publicatoin on March 31, 2013
Lund-Mackay
4)and Kennedy
5)CT staging scores to com- pare disease severity.
We tested patients for allergies using the multiple aller- gen simultaneous test, eosinophil count, and total im- munoglobulin E concentration. During the operation, we biopsied the polyp and cultured the discharge from the paranasal sinus.
The data collected included demographics, presence of asthma or documented allergy, history of surgery, extent of surgery, pre- and postoperative management, recur- rence of chronic sinusitis, and presence of diabetes mel- litus (DM), high blood pressure (HBP), and/or underlying disease.
All patients with ESSs were treated with saline irriga- tion, inhaled steroids, antibiotics, and antihistamines for 2 weeks postoperatively. Patients with polyps were treated with inhaled steroids for a mean period of 1 month, antibi- otics for 2weeks postoperatively. All patients with asthma were given oral and inhaled steroids for asthma control and followed by a pulmonologist and rhinologist for at least 1 year.
We used Student’s t - test to compare normally distributed variables. Variables that were not distributed normally were analyzed using the Mann–Whitney U - test (PASW Statistics 18; SPSS Inc., Chicago, IL, USA). A p - value <
0.05 was considered to be statistically significant.
RESULTS
We performed revision ESS 40 times to treat chronic si- nusitis; these operations represented 5% of all ESSs we performed. The study sample included 27, 7, 4, and 2 pa- tients who had undergone ESS two to five times, respec- tively. Their mean age at the time of first revision ESS in our department was 52.5 (range 22– 82) years. Thirty patients were male and 10 were female.
Mean age of primary ESS patients was 40.6 (range 15–85) years (Table 1). Revision ESS was performed for chronic sinusitis without polyps in nine operations and with polyps in 31 (77.5%) operations. Primary ESS was performed for chronic sinusitis without polyps in 23 operations and with polyps in 37 (61.6%) operations. Medication use did not differ between the primary and revision ESS groups. Pa- tients with nasal polyposis had a significantly (p = 0.000) higher propensity for requiring revision ESS (Table 2).
Data from CT scans performed before revision and prima- ry ESS were available for analysis for all 100 operations.
The extents of disease existing before revision and pri- mary ESS were compared. The respective Lund-Mackay and Kennedy CT scores were 9.9 and 2.1 in the primary ESS group and 10.6 and 2.4 in the revision ESS group.
No statistical difference was observed between revision
and primary ESS (Mann–Whitney U - test: Lund-Mackay score, p = 0.498; Kennedy CT score, p = 0.053; Fig. 1).
The primary ESS group contained 15 (25%) patients with allergies and 1 (1.6%) with asthma, versus 7 (17.5%) and 3 (7.5%) patients, respectively, in the revision ESS group.
In the primary ESS group, four patients had renal disease, three patients had thyroid disease, four (6.6%) had DM, and eight (13.3%) had HBP. In the revision ESS group, three (7.5%) patients had DM and 9 (22.5%) had HBP.
Bacterial cultures were positive in one (1.6%) case in the primary ESS group and nine (22.5%) cases in the revi- 38 / J Rhinol 20(1), 2013
Fig. 1. (A) Coronal computed tomographic image showing bi- lateral polyposis in the osteomeatal unit before primary sinus surgery. (B) Before revision sinus surgery, recurrent polyposis was detected bilaterally, especially on the left side, at 3 years after primary sinus surgery.
A B
Primary ESS Revision ESS Total
No. of patients 60 40 100
Male:female 31:29 30:10 61:39
Mean age (years) 40.6 52.5 51.9
Mean follow-up (months) 40 48 43.2
Table 1. Summary of patients in the primary and revision endo- scopic sinus surgery groups.
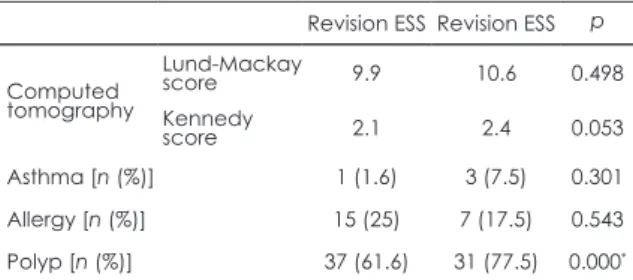
Table 2. Comparison of primary and revision endoscopic sinus surgery (ESS; Mann–Whitney U - test). The Lund-Mackay and Kennedy computed tomographic scores did not differ be- tween revision and primary ESS (Mann–Whitney U - test: Lund- Mackay score, p = 0.498; Kennedy score, p = 0.053). The revision ESS group contained seven (17.5%) patients with allergy and three (7.5%) with asthma. Patients with nasal polyposis had a high propensity for requiring revision ESS (p = 0.000).
Revision ESS Revision ESS p
Computed tomography
Lund-Mackay
score 9.9 10.6 0.498
Kennedy
score 2.1 2.4 0.053
Asthma [n (%)] 1 (1.6) 3 (7.5) 0.301
Allergy [n (%)] 15 (25) 7 (17.5) 0.543
Polyp [n (%)] 37 (61.6) 31 (77.5) 0.000*
*statistically significantigure.