-
44
-안와저 결손을 동반한 술후성 협부 낭종의 내시경적 조대술
인제대학교 의과대학 이비인후-두경부외과학교실,1 백인제기념 임상의학 연구소,2 영상의학교실,3 안과학교실4
허경욱1·박성국1,2·정 현1·정해웅3·이슬기4
Endoscopic Marsupialization of Postoperative Cheek Cyst with Orbital Floor Defect
Kyung Wook Heo, MD1, Seong Kook Park, MD, PhD1,2, Hyun Jung, MD1, Hae Woong Jeong, MD3 and Sul Gee Lee, MD, PhD4
1
Department of Otorhinolaryngology-Head and Neck Surgery,
2Paik Institute for Clinical Research,
3Diagnostic Imaging and
4Ophthalmology, Inje University, College of Medicine, Busan Paik Hospital, Busan, Korea
ABSTRACT
Background and Objectives:The postoperative cheek cyst with orbital involvement is a rare condition and the treatment of eroded orbital floor is controversial. This study evaluated the efficacy of endoscopic marsupialization for treating postop- erative cheek cyst with orbital floor defect and assessed the requirements of a direct orbital approach for orbital reconstruction.
Materials and Methods:The study involved a retrospective review of twelve patients with postoperative cheek cyst and orbital floor defect. Medical records were reviewed for details of previous surgery, presenting symptoms, surgical approach and the results of the operation. The maximum diameter of the involved orbital floor was calculated using the coronal imaging of paranasal sinus computed tomography (PNS CT). Results:All patients had previously undergone Caldwell-Luc procedures.
The most common symptom was pressure on the cheek. According to PNS CT, the maximum diameter of the involved orbital floor ranged from 0.7 to 3.1 cm (mean 1.46 cm) and the involved orbital area ranged from 0.35 to 4.23 cm
2(mean 1.87 cm
2). All patients underwent only endoscopic marsupialization without orbital reconstruction. Postoperatively, all patients showed no recurrence of symptoms or required revision surgery. Conclusion:Endoscopic marsupialization without recon- struction of the orbital floor could be considered as a first treatment option for postoperative cheek cyst combined with orbital floor defect.
KEY WORDS
:Mucocele·Maxillary sinus·Orbit·Endoscopy·Operations.
서 론
점액낭종은 부비동을 침범하는 비교적 흔한 낭성 질환으 로, 크기가 커지면서 안와를 침범하는 병변의 4~8.5%를 차 지하며 전두동과 사골동에서 가장 많이 발생한다.1) 부비동 점액낭종의 발생과 성장에는 선천적 인자, 점액 저류, 감염, 염증, 그리고 외상 등의 많은 요소들이 관여하며 부비동 자연공의 폐쇄와 분비물의 축적이 흔히 일어난다.2) 상악동 에 생긴 점액낭종은 대부분 Caldwell-Luc 수술 후에 2차
적으로 발생하는 술후성 협부 낭종으로 국내에서는 부비동 점액낭종의 반 이상을 차지하며,3) 드물게 안와 하벽을 손 상시키는 경우 낭종이 안와 내로 돌출하게 된다.4-7)
술후성 협부 낭종의 전통적인 치료는 Caldwell-Luc 접근 으로 낭종을 완전히 제거하고 하비도 비강상악동 개창술로 상악동의 환기를 유지하는 방법이 사용되어 왔으나, 최근에 는 술후성 협부 낭종을 포함한 상악동 점액낭종의 치료에 내 시경적 접근법이 시도되고 있다.1)2)8-11) 술후성 협부 낭종이 안와저 결손을 일으킨 경우 안와로의 직접 접근이 시행되고 있지만 적응증에 대해서는 정확히 알려져 있지 않다.12-14) 이에 저자들은 안와저 결손이 동반된 술후성 협부낭종에서 내시경적 조대술과 내시경 부비동 수술 만을 시행하여 증 상의 호전 정도와 안구돌출의 변화를 관찰하여 직접적인 안 와 접근법이나 안와벽 결손 재건술의 필요성 여부를 알아보 고자 하였다.
본 논문은 2005년도 인제대학교 학술연구조성비 보조에 의한 것임.
논문접수일:2008년 9월 10일 / 심사완료일:2008년 10월 22일 교신저자:박성국, 614-735 부산광역시 부산진구 개금2동 633- 165 인제대학교 의과대학 이비인후-두경부외과학교실
전화:(051) 890-6375·전송:(051) 892-3831 E-mail:[email protected]
대상 및 방법
1998년 3월부터 2005년 2월까지 안와저 결손을 동반한 술 후성 협부 낭종으로 진단되어 3차 의료기관에서 치료받은 환자 12명을 후향적으로 분석했다. 술후성 협부 낭종의 진 단은 과거 병력, 이학적 검사, 비내시경 검사, 부비동 컴퓨 터 단층촬영(Paranasal sinus computed tomography, PNS CT), 그리고 수술 소견에 따라 내렸으며 의무기록을 검토 하여 환자의 현재 증상, 코수술 과거력, 이전 코수술과 증 상 발생까지의 기간, 수술 방법, 술후 증상 및 병변의 회복 정도, 그리고 재수술여부 등을 조사했다. 안구돌출을 호소 한 두 명의 환자에서는 안과적인 검사를 시행했으며, 술전 PNS CT는 환자에 대한 정보 없이 한 명의 영상의학과 전 문의가 판독하고 계측했다. 술전 PNS CT에서 협부 낭종이 안와를 명백하게 침범한 경우만 포함시켜 골 결손 없이 골 미란만 존재할 가능성이 있는 경우는 대상에서 제외하였으 며, 다발성 낭종(multiple cyst)의 경우도 모두 Caldwell- Luc 접근을 시행하여 대상에서 제외하였다. PNS CT의 관 상면에서 결손된 안와저의 장경을 측정한 다음, 측정된 장 경, 결손이 관찰되는 PNS CT 단면 갯수, 그리고 PNS CT 단면의 두께를 이용해 안와저 결손의 면적을 계산했다.
수술은 동일한 술자에 의해 시행되었다. 국소 또는 전신마 취하에 비강내 내시경적 접근법을 시행하여 점액류 내측벽 일부를 개방하고 굴곡된 흡인기로 어두운 색깔의 수양성 내 용물을 확인하여 술후성 협부 낭종으로 확진한 다음, 중비도 및 하비도 비강상악동 개창술을 시행했다. 점액류 내벽의 완 전 제거, 안와벽 재건, 그리고 외부 안와 접근술은 시행하지 않았으며 비강 패킹후 수술을 종료했다. 술후 1~2일에 패킹 을 제거하고 다음 날 퇴원하여 외래추적 관찰을 시행했다.
결 과
12명의 환자중 남자 10명, 여자 2명이었고 연령은 36~66 세로 평균 52.3세 였다. 모든 환자는 이전에 상악동의 만 성 부비동염에 대해 Caldwell-Luc수술을 시행받은 과거력 이 있었고 이전 수술과 현재 증상의 발생까지 경과 시간은 3~50년으로 평균 20.5년 이었다. 환자들이 호소한 증상은 협부 압박감(9명), 비폐색(5명), 안구 돌출(2명), 그리고 복 시(1명) 등 이었다(Table 1). 안구 돌출을 호소하던 환자 두 명은 Hertel 안구돌출계 검사상 각각 3 mm의 안구 돌출이 있었고, 한 명은 상방, 내측, 및 외측 주시시 복시를 호소했 으나 Hess chart 검사상 정상 소견이었다.
모든 환자는 술전 PNS CT상 낭성 병변이 상악동을 완전 히 채우고 있었으며, 안와 하벽의 골결손을 통해 안와 내로 침범하고 있었다(Figs. 1A and 2A). 안와저에서 골결손부의 장경은 0.7~3.1 cm의 범위로 평균 1.46 cm이었고, 면적은 0.35~4.23 cm2의 범위로 평균 1.87 cm2이었다(Table 2).
수술 중이나 수술 후 특별한 합병증은 없었으며 술후 추 적관찰은 14~70개월간(평균 35.8개월) 시행했다. 수술 전 환자의 증상 중 협부 압박감은 수술 후 모든 환자에서 완 전히 사라졌고, 술전에 비폐색을 호소한 5명의 환자 중 1 명에서 경도의 비폐색이 남아 있었다. 술전 복시를 호소한 1명의 환자는 수술 후에도 경도의 복시를 호소했지만 Hess chart 검사상 정상 소견이었다. 안구 돌출은 술후 1주 경 부터 호전되기 시작하였고, 술후 3주째 시행한 Hertel 안구 돌출계 검사상 두 명의 환자 모두 정상소견 이었다. 그리 고, 술후 각각 8개월과 13개월에 시행한 PNS CT상 이전의 낭성 병변은 소실되었으며 중비도 비강상악동 개창부위는 잘 유지되었고, 안와 하벽의 결손 장경과 면적은 변화가 없
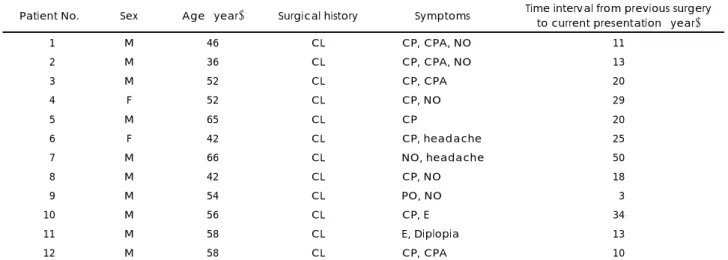
Table 1. Characteristics of patients with postoperative cheek cyst with orbital floor defect
Patient No. Sex Age (year) Surgical history Symptoms Time interval from previous surgery to current presentation (year)
01 M 46 CL CP, CPA, NO 11
02 M 36 CL CP, CPA, NO 13
03 M 52 CL CP, CPA 20
04 F 52 CL CP, NO 29
05 M 65 CL CP 20
06 F 42 CL CP, headache 25
07 M 66 CL NO, headache 50
08 M 42 CL CP, NO 18
09 M 54 CL PO, NO 03
10 M 56 CL CP, E 34
11 M 58 CL E, Diplopia 13
12 M 58 CL CP, CPA 10
CL:Caldwell-Luc operation, CP:cheek pressure, CPA:cheek pain, NO:nasal obstruction, PO:periorbital pain, E:exophthalmos
었지만, 골 재형성(bone remodeling)이 일어나 함몰되지 않 았다(Figs. 1B and 2B). 재수술이 필요한 경우는 없었으며 현재 외래 추적관찰 중이다.
고 찰
상악동 점액류의 가장 흔한 원인은 외상으로, 사고에 의하 거나 Caldwell-Luc 수술 후에 의인성으로 발생할 수 있
다.15) 특히 수술 후 발생한 상악동 점액류는 점액류내의 분 비액이 저류되어 서서히 진행하는 경우가 많고, 감염으로 인 해 점액류가 급격히 커질 경우 빠른 진행을 보이며 주위 구 조물을 압박하거나 폐쇄시켜 증상을 일으킨다.1) 협부의 무 통성 종물과 비폐색을 호소하는 경우가 가장 많아 술후성 협부 낭종으로 불리며, 안구 증상으로는 안구 돌출, 시력저 하, 복시, 사시가 발생할 수 있다.6) 본 연구에서는 환자들 은 협부의 압박감을 가장 많이 호소했고 2명에서 안구 돌
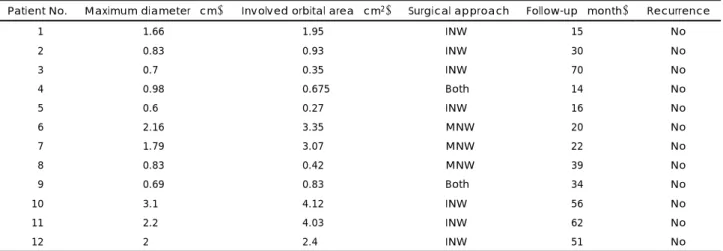
Table 2. Coronal paranasal sinus computed tomography measurements, surgical approaches and outcomes for postoperative cheek cysts combined with orbital floor defect
Patient No. Maximum diameter (cm) Involved orbital area (cm2) Surgical approach Follow-up (month) Recurrence
01 1.66 1.950 INW 15 No
02 0.83 0.930 INW 30 No
03 0.70 0.350 INW 70 No
04 0.98 0.675 Both 14 No
05 0.60 0.270 INW 16 No
06 2.16 3.350 MNW 20 No
07 1.79 3.070 MNW 22 No
08 0.83 0.420 MNW 39 No
09 0.69 0.830 Both 34 No
10 3.10 4.120 INW 56 No
11 2.20 4.030 INW 62 No
12 200. 2.400 INW 51 No
INW:Inferior nasoantral window, MNW:Middle nasoantral window, Both:INW+MNW
Fig. 1. Paranasal sinus computed tomo- graph scans in case number 10. Pre- operative coronal image (soft tissue setting) showing a cystic mass filling the right maxillary sinus, and bone ero- sion in the right orbital floor and ex- tending into the right orbit (white ar- row)(A). Postoperative coronal image (bone setting) showing no evidence of the earlier cystic lesion, patency of the middle nasoantral window, and bone remodeling in the inferior wall of the right orbit (white arrow)(B).
B A
Fig. 2. Paranasal sinus computed to- mograph scans in case number 11.
Coronal image (bone setting) show- ing a cystic mass filling the left maxi- llary sinus with pressure erosion in the lateral, medial, and superior wall of the left maxillary sinus and extending into the left orbit through the orbital wall defect (white arrow)(A). Postop- erative coronal image showing no evidence of depression in the left or- bital floor (white arrow)(B).
B A
출이 동반되었다. 술후성 협부 낭종의 진단은 수술 받은 병력, 증상, 이학적 검사, 그리고 방사선학적 검사 등으로 내릴 수 있다. 특히 PNS CT는 비용면에서 효과적이며 골 미란 등의 골변화를 민감하게 진단할 수 있는 장점이 있어 일반적으로 널리 사용된다.16)
술후성 협부 낭종의 치료는 점액류 상피를 완전히 제거 하고 환기가 잘되는 부비동 또는 비강과의 교통을 확보하 는 것을 원칙으로 하여5)7) 과거에는 Caldwell-Luc 수술 또 는 Weber-Ferguson 접근법을 이용한 근치적 접근방법이 사용되었다.13)17) 최근에는 근치적 수술보다 기능적이고, 정 상 점막으로의 재생이 훨씬 용이하며, 수술시간이 짧고, 출 혈이 거의 없으며, 회복기간이 짧은 비강내 비내시경적 접 근으로 시행하는 경우가 늘어나고 있다.1)2)8-10) 그러나, 외측 에 위치한 전두동 점액류, 전두동개구부위가 비후된 골에 의해 막혀있는 경우, 악성질환에 의해 발생한 점액류, 그 리고 다발성 낭종(multiple cyst)의 경우는 아직 외부 접근 을 통한 수술이 권장되고 있다.18)
전두동 점액류에 대한 조대술후 6개월이 경과하여 시행한 조직학적 검사에서 정상적인 위중층 섬모 원주상피가 보고 된 바 있으며,19) 조대술후 비내시경 검사상 점액류 내피가 정상 점막으로 덮여있는 것으로 관찰되었다.20) 이러한 보 고에 비추어 볼 때, 저자들은 술후성 협부 낭종류의 치료 에 있어 점액류 내용물을 제거하고 배농한 후 충분한 크기 의 비강상악동 개창술로도 치료가 가능할 것으로 착안하여 본 연구를 시행했다.
안와 외향골절의 경우 안와저 결손의 면적이 2 cm2 이상 일 때 수술적 처치의 적응증이 되지만,21) 술후성 협부 낭종 에 의한 안와저 결손에 대해서는 수술적 처치의 적응증에 대한 검토가 거의 이루어지지 않았다. 일부 저자들은 안와 저 결손이 있는 상악동 점액류의 수술시 비강내 내시경적 접근과 동시에 외안부 접근으로 안와저를 재건하여 좋은 결과를 보고하고 있지만, 외안부 접근의 구체적인 적응증 에 대해서는 언급이 거의 없다.8)13) 사골동 또는 접형동 점 액류에 의한 안구 병변을 수술할 때 외안부 접근을 시행하 면 수술부위의 노출과 안정성을 확보할 수 있고 재발성 염 증에 의한 점액류 상피가 안와 연조직에 유착이 있는 경우 에도 정확한 박리를 할 수 있는 장점이 있고 비내시경적 조 대술 시행시에는 내직근이나 시신경의 손상이 드물게 보고 되고 있어,22)23) 안과영역에서는 많은 술자들이 사골동 또는 접형동 점액류에 의한 안구돌출시 외안부 접근법을 선택하 고 있다.1)24-26) 그러나, 상악동 점액류시 비내시경적 조대 술을 시행한 최근의 연구들에서 수술에 의한 안구 등의 합 병증은 거의 없이 낮은 재발률을 보이고 있으며, 이는 비
내접근시 손상이 쉬운 내직근이나 시신경과는 사골동이나 접형동 보다 해부학적 거리가 멀기 때문인 것으로 사료된 다.1)2)8)11)20)
점액류에 의해 안와저 골의 결손이 있더라도 periorbita가 손상되지 않은 경우 골 재형성 없이도 안와 내용물에 대한 적절한 지지를 할 수 있는 것으로 알려져 있으며18) 본 연구 에서도 안와저 결손의 면적이 0.35~4.23 cm2의 크기였지 만 안와내 농양이나 시력감퇴의 합병증은 없었으므로, 비 내시경적 조대술만으로도 합병증 없이 병변이 완치되었고 외안부에 대한 접근은 필요하지 않았다.
본 연구에서와 같이 술후성 협부 낭종 환자에서 안구돌 출이 동반되어 있더라도 안와저에 단순 결손만 있다면, 비 강내 비내시경적 조대술을 먼저 시행하고, 증상의 잔존이 나 재발 여부에 따라 낭종 내벽의 완전절제와 안와저의 재 건은 이차적으로 시행할 수 있을 것으로 사료된다.
결 론
저자들은 12명의 안와저 결손을 동반한 술후성 협부 낭 종 환자를 비강내 내시경적 조대술로 완치했다. 술후성 협 부 낭종으로 인해 안와저에 단순 결손만 있을 경우 안구돌 출이 동반되더라도 일차적으로 내시경적 조대술을 시행할 수 있으며, 안와벽의 재건은 조대술 시행 후에도 안구 증 상이 남아 있을 경우 고려할 수 있을 것으로 사료된다.
중심 단어:점액낭종·상악동·안와·내시경·수술.
REFERENCES
1) Khong JJ, Malhotra R, Wormald PJ, Selva D. Endoscopic sinus surgery for paranasal sinus mucocele with orbital involvement.
Eye 2004;18:877-81.
2) Busaba NY, Kieff D. Endoscopic sinus surgery for inflammatory maxillary sinus disease. Laryngoscope 2002;112:1378-83.
3) Song HM, Park HW, Chung YS, Jang YJ, Lee BJ. Primary muco- celes of the maxillary sinus. Korean J Otorhinolaryngol-Head Neck Surg 2006;49:47-51.
4) Som PM, Shugar JM. Antral mucoceles: a new look. J Comput Assist Tomogr 1980;4:484-8.
5) Hasegawa M, Kuroishikawa Y. Protrusion of postoperative maxillary sinus mucocele into the orbit: case reports. Ear Nose Throat J 1993;
72:752-4.
6) Kaltreider SA, Dortzbach RK. Destructive cysts of the maxillary sinus affecting the orbit. Arch Ophthalmol 1988;106:1398-402.
7) Gardner DG, Gullane PJ. Mucoceles of the maxillary sinus. Oral Surg Oral Med Oral Pathol 1986;62:538-43.
8) Busaba NY, Salman SD. Maxillary sinus mucoceles: clinical pre- sentation and long-term results of endoscopic surgical treatment.
Laryngoscope 1999;109:1446-9.
9) Benninger MS, Marks S. The endoscopic management of sphenoid and ethmoid mucoceles with orbital and intranasal extension. Rhi-
nology 1995;33:157-61.
10) Marks SC, Latoni JD, Mathog RH. Mucoceles of the maxillary sinus. Otolaryngol Head Neck Surg 1997;117:18-21.
11) Kwon SH, Yang YS, Min YG. Surgical treatment and clinical study of postoperative maxillary cyst. Korean J Otorhinolaryngol-Head Neck Surg 1997;40:1115-21.
12) Billing KJ, Davis G, Selva D, Wilscek G, Mitchell R. Post-trau- matic maxillary sinus mucocele. Ophthalmic Surg Lasers Imaging 2004;35:152-5.
13) Garber PF, Abramson AL, Stallman PT, Wasserman PG. Globe ptosis secondary to maxillary sinus mucocele. Ophthal Plast Reconstr Surg 1995;11:254-60.
14) Choi IS, Kim JS, Jun BH. Two cases of postoperative cheek cyst with exophthalmos. Korean J Otorhinolaryngol-Head Neck Surg 2005;
48:267-70.
15) Atherino CC, Atherino TC. Maxillary sinus mucopyoceles. Arch Otolaryngol 1984;110:200-2.
16) Raman S. Mucocele of the maxillary sinus and the eye. Eye 2003;
17:101-4.
17) Schramm VL Jr, Effron MZ. Nasal polyps in children. Laryngoscope 1980;90:1488-95.
18) Shah A, Meyer DR, Parnes S. Management of frontoethmoidal mucoceles with orbital extension: is primary orbital reconstruction necessary? Ophthal Plast Reconstr Surg 2007;23:267-71.
19) Har-El G, DiMaio T. Histologic and physiologic studies of marsu- pialized sinus mucoceles: report of two cases. J Otolaryngol 2000;
29:195-8.
20) Har-El G, Balwally AN, Lucente FE. Sinus mucoceles: is marsupi- alization enough? Otolaryngol Head Neck Surg 1997;117:633-40.
21) Bai CH, Ye SB, Park KS, Song SY, Kim YD. Transnasal endoscopic reconstruction of medial orbital wall fracture. Korean J Otorhi- nolaryngol-Head Neck Surg 2005;48:1468-72.
22) May M, Levine HL, Mester SJ, Schaitkin B. Complications of en- doscopic sinus surgery: analysis of 2108 patients-incidence and pre- vention. Laryngoscope 1994;104:1080-3.
23) Kinsella JB, Calhoun KH, Bradfield JJ, Hokanson JA, Bailey BJ.
Complications of endoscopic sinus surgery in a residency training program. Laryngoscope 1995;105:1029-32.
24) Wang TJ, Liao SL, Jou JR, Lin LL. Clinical manifestations and management of orbital mucoceles: the role of ophthalmologists.
Jpn J Ophthalmol 2005;49:239-45.
25) Lai PC, Liao SL, Jou JR, Hou PK. Transcaruncular approach for the management of frontoethmoid mucoceles. Br J Ophthalmol 2003;
87:699-703.
26) Shorr N, Baylis HI, Goldberg RA, Perry JD. Transcaruncular ap- proach to the medial orbit and orbital apex. Ophthalmology 2000;
107:1459-63.