- 31 -
KISEP Original Article J Rhinol 11(1,2), 2004
Navigation Assisted Transsphenoidal Approach for Pituitary Tumor
Seung-Hoon Lee, M.D.1, Eun-Jae Jung, M.D.1, Sang-Hag Lee, M.D.1, Heung-Man Lee, M.D.1, Soon-Young Kwon, M.D.1, Ji Ho Choi, M.D.2 and Cheol Min Ahn, M.D.2
ABSTRACT
The transsphenoidal approach is the choice of surgical approach for the treatment of pituitary tumors located on the upper portion of the sphenoid sinus. The proximity of vital anatomic structures (e.g. optic nerve, carotid artery, carvernous sinus, and anterior cranial fossa) surrounding the sphenoid sinus makes it difficult for surgeons to recognize the precise location during the transsphenoidal approach. We report 16 cases of transsphenoidal approach performed via the navigation system to identify vital anatomic structures and important surgical landmarks. We analyzed 16 patients to perform the transcrural transcolumellar approach under the guidance the navigation system for pituitary tumor resection. For the verification of important anatomic structures during operation, the navigation system demonstrates the position and direction of the probe on CT scans in real time.
The intrasphenoidal septum was in the midline in only four cases but not so in the other 12 cases. However, the posterior portion of the bony nasal septum attached to the anterior wall of the sphenoid sinus was located in the mid-portion of the sphenoid sinus in all cases. Without any serious damage to the important structures around the sella turcica, we successfully performed the pituitary tumor operation in all cases. Using the navigation system, we identified the relationship between the sella turcica and surrounding important structures on CT scan in real time, and successfully removed the pituitary tumors without complications.
In addition, we suggest that the posterior portion of the bony nasal septum attached to the anterior wall of the sphenoid sinus may be one of the available landmarks for the localization of the midline during a transsphenoidal approach.
KEY WORDS:Pituitary neoplasms・Neuronavigation.
INTRODUCTION
The transsphenoidal approach is the preferred route for the removal of the pituitary tumors that are con- fined to the sella turcica.1) The proximity of delicate anatomic structures (e.g. optic nerve, carotid artery, car- vernous sinus, floor of anterior cranial fossa) makes it mandatory for the surgeon to recognize precise lo- cations. Unfortunately, misdirected injuries for these structures lead to severe neurovascular complications,
which are known to sometimes be fatal.2-4) Therefore, to avoid the damage to these vital structures on the la- teral wall of the sphenoid sinus and to achieve safer and more accurate surgical interventions, it is important to identify the safe and constant midline landmarks and to be well aware of the surrounding anatomy during operation.
For this purposes, many intraoperative navigation systems for neurosurgical procedures and endoscopic sinus surgery have been introduced.5-7) The navigation system permits a direct comparison of intraoperative anatomy with preoperative CT or MRI imaging. The surgeon may point to a specific structure with a pointer instrument and then view the location of the instrument tip on CT or MRI images which are projected in all three orthogonal planes, in real time. Especially, this system is very useful in cases with distorted anato- mical structures.
We report 16 cases of transspehnoidal approaches performed under the guidance of a navigation system
1Department of Otorhinolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, 2Department of f Otolaryngology, Pundang Jesaeng General Hospital, Daejin Medical Center, Pundang, Korea
Address correspondences and reprint requests to Seung-Hoon Lee, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, Korea University College of Medicine, Ansan Hospital, 516 Kojan-dong, Ansan 425-707, Korea
Tel:82-31-412-5170, Fax:82-31-401-4365 E-mail:[email protected]
Accepted for publication on July 27, 2004
32 / J Rhinol 11(1,2), 2004
to reveal the safe landmark for the midline and to avoid damage of vital anatomic structures surrounding the sella turcica.
MATERALS AND METHODS
From December 1999 to February 2002, 16 patients at Pundang Jesaeng General Hospital underwent a tran- scrural transcollumellar approach under the navigation system for resection of pituitary tumors. There were nine male and seven female patients with a mean age of 44 years (from 22 to 75 years). Five patients pres- ented with IICP (increase intracranial pressure) symp- toms such as headache or vomiting. Six patients pres- ented with acromegaly, four patients with galactorrhea, amenorrhea and one patient had visual disturbance as a presenting symptom. Six patients had nasal septal de- viation. The sphenoid sinus was classified into the sellar, presellar and concha type depending on the degree of pneumatization of the sphenoid sinus. The sellar type is well pneumatized below the sellar floor, the presellar type shows pneumatization limited to the anterior aspect of the sella turcica and the concha type is occupied with the cancellous bone with pneumatization mostly absent. Before surgery, the patient was fitted and under- went ostiomeatal unit computed tomography (OMU CT) with the five reference markers in their face.
These scans were sent to the Vector Vision navigation system (Brain Lab, Heimstetten, Germany) using LAN (local area network). On the day of surgery, the pa- tient’s head was fixed tightly on the head supporter not to move the reference marker on the forehead during
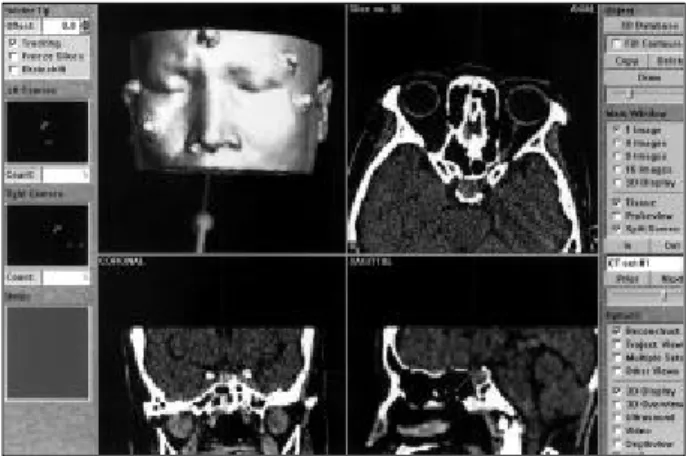
operation (Fig. 1). And then the pointer instrument was placed on the five reference markers and the in- frared ray from the camera of navigation system was reflected in order to register the pointer instrument’s location on the CT scan. The navigation system de- monstrated the position and the direction of the pointer instrument in three orthogonal planes (axial, coronal, and sagittal plane).
For access to the sella turcica, we used the tran- scrural transcolumellar approach to enter the sphenoid sinus. An inverted V incision was used to incise the full thickness of the columellar skin and was connec- ted posteriorly to a complete septal transfixion incision.
The submucoperichondrial and submucoperiosteal dis- section proceeded along the cartilagenous septum and nasal floor. The vomer and perpendicular plate of the ethmoid were removed. And then the self retaining transseptal pituitary speculum was placed between the sepal mucosal flap on the right and the cartilaginous septum to the left. After we inserted the pituitary spe- culum, we elevated the mucosa situated on the posterior portion of the nasal septum and confirmed whether it was reaching the appropriate position by using a pointer instrument. Once the anterior wall of the sphenoid sinus was resected, we could identify the intrasphenoidal septum inside the sphenoid sinus and define the sella turcica at the exact location using the navigation system (Fig. 2-4). The tumor was removed by a neurosurgeon with a microsurgical technique under the information provided by the navigation system. After removal of the tumor, the sphenoid sinus was obliterated by fat tissue from the abdomen and bony segments harvested from the septum. The medial crura was reapproximated
Fig. 1. Five reference markers on the forehead and both maxilla areas. The infrared ray from the camera of the navigation sys- tem is reflected in order to register the probe location on the
preoperative CT scan. Fig. 2. Probe on the sella turcica. The pituitary tumor is located on the postero-superior portion of the sphenoid sinus.
Fig. 3. Probe on the left lateral wall of the sphenoid sinus.
Lee et al:Navigation Assisted Transsphenoidal Approach / 33
with horizontal a mattress suture. Finally, the columellar skin incision and transfixion incision were approxi- mated. The intranasal packings with Merocel (Medt- ronic Xomed, Jacksonville, FL) and vaseline gauze were performed and maintained for two days. The mean postoperative follow-up time was 18 months (ranged from 12 months to 26 months).
RESULTS
Considering the pneumatization state of the sphe- noid sinus, 12 patients had the sellar type, three pa- tients had the presellar type and one patient had the concha type. According to brain MRI and histopatho- logic examinations, there were four microadenomas, 11 macroadenomas and one Rathke’s cleft cyst. The navigation system preparation time periods (data tran-
sfer, three-dimensional data reconstruction, positioning, sensor probe calibration and registration) from initiliza- tion to surgery ranged from 13 to 26 minutes (mean of 21 minutes). Anatomical landmarks such as the intras- phenoidal septa, bony protrusion for optic nerves, ca- rotid arteries, and the skull base were easily identified by the navigation system. Without any serious damage to vital structures surrounding the sella turcica, we successfully performed the pituitary tumor operation.
There were no serious delayed postoperative compli- cations such as CSF leak, septal perforation, nasal tip deformity and saddle nose, except for only in one case, where transient diabetes inspidus was noticed. An in- trasphenoidal septum in the sphenoid sinus was re- vealed in the midline in only four cases. However, the posterior portion of the bony nasal septum attached to the anterior wall of the sphenoid sinus was located in the midline of the sphenoid sinus in all cases.
DISCUSSION
In accessing the pituitary tumor, Caton first intro- duced the extracranial approach in the 19th century but it was limited because of the risks and complications of the procedure itself.8) Substituing this procedure, Cushing used the sublabial transseptal approach on 247 patients. However, the visual field was narrower than Caton’s and it gave no difference in complications such as CSF leakage or meningitis.8) Since then ope- rative equipments as operative microscope and intra- operative C-arm fluoroscopy were developed and prospered. Hardy tried a sublabial transseptal approach which was a modified version of the Cushing’s app- roach and improved the operation outcome and resulted in less postoperative complications.1)
Anatomically, the cavernous sinus, the internal ca- rotid artery, and the optic nerve are situated on the lateral wall of the sphenoid sinus, and injuries to these structures resulted in serious complications. Particu- larly, damage to the internal carotid artery and the cavernous sinus caused various vascular complications, such as carotid cavernous fistulas and carotid false aneurysm.2)3) Therefore, it is essential to be well aware of the anatomic relationship of the surrounding im- portant structures while operation takes place.
The intra-operative C-arm fluoroscopy is the most widely used method for confirming the direction of
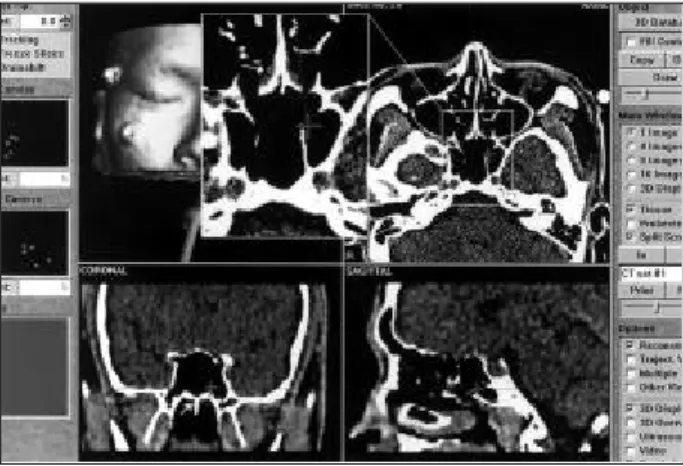
Fig. 4. Probe on the intrasphenoidal septum. The intrasphe- noidal septum is located on the paramedian portion of the sphenoid sinus, not in the midline. The nasal septum is deviated to left side. However, the posterior portion of bony nasal septum attached to the anterior wall of the sphenoid sinus is located on the midline of the sphenoid sinus (arrow).
Fig. 3. Probe on the left lateral wall of the sphenoid sinus.
34 / J Rhinol 11(1,2), 2004
approach during pituitary tumor surgery via the transs- phenoidal route.9) However, the images obtained from fluoroscopic techniques are limited to the sagittal plane, and may expose the patient and personnels to radiation.
When compared to the fluoroscopic technique, the navigation system provides the information for vital structures on the lateral side of the sphenoid sinus in the coronal and axial sections for the operator. Therefore, the location of the medial wall of the carotid eminence and the cavernous sinus can be confirmed. In addition, the navigation system demonstrates the relative position and orientation of the probe in real time. Especially, in cases of a deviated intrasphenoidal septum, not in the midline, we can identify the exact location through axial and coronal sections and differentiate the intrasphe- noidal septum from the lateral wall of the sphenoid sinus. In this study, an intrasphenoidal septum in the sphenoid sinus was not in the midline for 12 cases.
Subsequently, in those cases, the exact approach to the sella turcica may be difficult by conventional indentifi- cation methods such as intra-operative C-arm fluoro- scopy. However, using axial and coronal sections of the navigation system during operation, accurate pro- cedures are possible without any damage to the vital structures lying on the lateral wall of the sphenoid sinus.
Since the navigation system has no possibility of ra- diation exposure, there is no need for personnel to wear protective gear.
The superior turbinate, the inferior aspect of the middle turbinate, the nasal septum and the intrasphe- noidal septum have been as useful landmarks for safe pituitary surgery.10)11) Indeed, the nasal septum and in- trasphenoidal septum were not in the midline frequently.
Therefore, serious damage to the vital structures surr- ounding the sella can be possible in those situations. In this study, six patients had nasal septal deviation and 12 patients did not have the intrasphenoidal septum in the midline. However, the posterior portion of the bony septum attached to the anterior wall of the sphenoid sinus was located in the midline of the sphenoid sinus
in all cases. We have found that the posterior portion of the bony septum is a consistent and reliable anatomic marker for midline localization.
CONCLUSION
A navigation system can allow surgeons to confirm the sella turcica and surrounding vital structures in real time during operation, and to perform pituitary tumor resection successfully without interrupting these stru- ctures. And the posterior portion of the bony nasal septum attached to the anterior wall of the sphenoid sinus is a useful constant landmark for safe surgery, especially, in those cases where the intrasphenoidal septum is not located in the midline.
REFERENCES
1) Hardy J. Transsphenoidal hypophysectomy. J Neurosurg 1971;34:
582-94.
2) Pigott TJ, Holland IM, Punt JA. Carotico-cavernous fistula after trans- sphenoidal hypophysectomy. Br J Neurosurg 1989;3:613-6.
3) Reddy K, Lesiuk H, West M, Fewer D. False aneurysm of the caver- nous carotid artery: a complication of transsphenoidal surgery. Surg Neurol 1990;33:142-5.
4) Tong H, Wei S, Zhou D, Zhu R, Pan L, Jiang J. Vision deterioration after transsphenoidal surgery for removal of pituitary adenoma.
Zhonghua Wai Ke Za Zhi 2002;40:746-8.
5) Lasio G, Ferroli P, Felisati G, Broggi G. Image-guided endoscopic transnasal removal of recurrent pituitary adenomas. Neurosurgery 2002;51:132-6.
6) Ohhashi G, Kamio M, Abe T, Otori N, Haruna S. Endoscopic trans- nasal approach to the pituitary lesions using navigation system (Insta- Trak System). Acta Neurochir (Wien) 2001;143:501-3.
7) Anon JB. Computer-aided endoscopic sinus surgery. Laryngoscope 1998;108:949-61.
8) Collins WF. Hypophysectomy: historical and personal perspective.
Clin Neurosurg 1974;21:68-78.
9) Hardy J, Wigser SM. Trans-sphenoidal surgery of pituitary fossa tu- mors with televised radiofluoroscopic control. J Neurosurg 1965;23:
612-9.
10) Jho HD, Alfieri A. Endoscopic endonasal pituitary surgery: evolution of surgical technique and equipment in 150 operations. Minim In- vasive Neurosurg 2001;44:1-12.
11) Bolger WE, Keyes AS, Lanza DC. Use of the superior meatus and superior turbinate in the endoscopic approach to the sphenoid sinus.
Otolaryngol Head Neck Surg 1999;120:308-13.