INTRODUCTION
A maxillary sinus fungus ball is a chronic noninvasive mycosis that is commonly diagnosed in patients with a history of recurrent maxillary sinusitis recalcitrant to stan- dard medical therapy. Fungus balls frequently develop in healthy individuals with no obvious relation of fungal infection. Some studies have shown that endodontic treat- ment on maxillary teeth is a strong risk factor for forma- tion of a fungus ball of the maxillary sinus.1) 2) However, cases of extruded endodontic obturation materials into the nasal cavity and producing maxillary fungal sinusitis are rare. In this article, we report a case preoperatively diag- nosed as fungal sinusitis which postoperatively revealed a fungus ball with gutta-percha in the nasal cavity.
CASE
A 52-year-old woman was referred to the Department of Otorhinolaryngology-Head and Neck Surgery of Samsung Medical Center with history of right side purulent nasal discharge, obstruction and right facial pain. Although she
couldn’t remember exact data, more than 5years age, she took a dental treatment. From five-years before, she has got a pain in right cheek area. She visited several dental clinics, but she couldn’t get an answer about dental prob- lem. Because pain did not stop, and newly nasal obstruc- tion and discharge was occurred, she had undergone right J Rhinol 20(2), 2013
- 127 -
www.ksrhino.or.kr
- 127 -
Extrusion of Gutta-Percha into the Nasal Cavity Causing Maxillary Fungal Sinusitis: A Case Report
Myung Eun Nam, MD, Sang Duk Hong, MD, JunOh Park, MD and Seung-Kyu Chung, MD, PhD
Department of Otorhinolaryngology-Head and Neck Surgery, Sungkyunkwan University School of Medicine, Samsung Medical Center, Seoul, Korea
ABSTRACT
There have been few reports about extrusion of endodontic obturation materials into the maxillary sinus and inducing fungal sinusitis. Endodontic materials and fungus balls both are seen as high attenuation in a CT scan so may be overlooked. We report such a case in which the surgeon and radiologist had missed the foreign materials on preoperative CT scans, and recognized the filling defect on the alveolar bone and a foreign body in the nasal cavity postoperatively.
KEY WORDS : Fungus·Sinusitis·Odontogenic·Foreign Body.
Address correspondence and reprint requests to: Seung-Kyu Chung, MD, PhD, Department of Otorhinolaryngology-Head and Neck Sur- gery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Irwon-dong, Gangnam-gu, Seoul 135-710, Korea.
Tel: +82-2-3410-3579 · Fax: +82-2-3410-3879 E-mail: [email protected]
Received for publication on March 6, 2013 Accepted for publicatoin on August 26, 2013
A B
A B
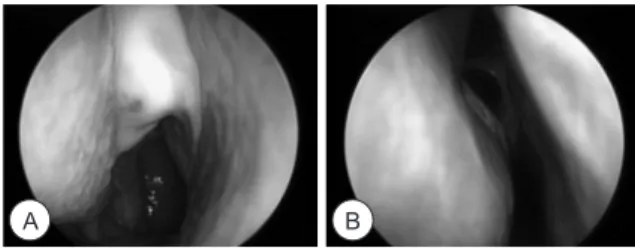
Fig. 1. Endoscopic view of right nasal cavity at first visit.
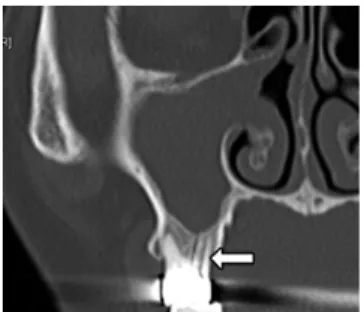
Fig. 2. (A) Preoperative coronal CT scans (bone window set- ting): Soft tissue lesion obliterating the right maxillary sinus and a mass-like lesion with a faint high-attenuation mottled calcifica- tion (white arrow) in the right nasal cavity medial to the maxil- lary sinus. (B) Preoperative coronal CT scans (soft tissue window setting; same cut with A): Prominent calcified rod (yellow arrow head) surrounded by a high-density mottled lesion.
128 / J Rhinol 20(2), 2013
sinus surgery for sinusitis at another ENT clinic 3 years previous.
The patient did not have other disease that could cause immune suppression. In nasal endoscopic examination, there was purulent discharge on right middle meatus (Fig.
1). CT scan revealed a soft tissue lesion with faint high-at- tenuated mottled calcification in the right maxillary sinus (Fig. 2A). She was diagnosed with right maxillary fungal sinusitis based on radiological results. Endoscopic sinus surgery under general anesthesia was performed. During operation, we incidentally detected and removed foreign bodies in the middle meatus, surrounded by typical fun- gus ball material. Pathology findings after surgery, authors could identify the presence of the fungal hyphae (Fig 3).
The extirpated foreign material was confirmed to consist of gutta-percha (Fig. 4). We postoperatively reviewed the preoperative CT scan and noted empty spaces in the roots on the right maxillary tooth where root-filling materials would be positioned (Fig. 5). Changing the window level
of the CT scan showed additional denser material, sug- gesting the presence of a foreign body surrounded by less dense mottled materials that had been missed in the bone window setting (Fig. 2B). The postoperative course was satisfactory.
DISCUSSION
A fungus ball of the maxillary sinus is the most com- mon fungal sinusitis and usually develops unilaterally in the maxillary sinus without bony invasion.2) 3) The patho- genesis of a fungus ball of the maxillary sinus remains largely unknown. However, it has been suggested that teeth having undergone a root canal with overextension of the root canal sealer into the sinus might be one of the etiological factors of aspergillosis of the maxillary sinus in healthy patients. The floor of the maxillary sinus or sinus mucosa can be damaged by chemical and physical trauma, causing inflammation as a result of endodontic treatment.
Furthermore, root-filling materials containing zinc oxide- eugenol have been reported to microbiologically promote the growth of Aspergiollosis fumigates.4-6)
In the view of endodontic treatment, when sealer and/or gutta-percha are extruded into the periapical tissue, there is always a severe inflammatory reaction. For best endo- dontic treatment, the obturation must remain at the apical constriction.
Radiographically, the unique appearance of a dense opacity in the maxillary sinus is considered a character- istic finding of a fungus ball. In this case, we diagnosed a fungus ball in the maxillary sinus.7) However, we were not aware of gutta-percha in the nasal cavity or a preoperative filling defect in the maxillary tooth. This case shows that we must consider the possibility of a foreign body such as root filling materials and perform a thorough evalua- tion around the maxillary teeth and sinus in the presence of unilateral maxillary fungal sinusitis with a history of endodontic treatment.
As far as we are aware, this is the first report of root filling material (gutta-percha) surrounded by a fungus ball located in the nasal cavity, though migration of gutta- percha from a root canal location into the ethmoid sinus without fungal sinusitis was reported in 2004.8)
저자역할(Author Contributions)
남명은, 홍상덕, 박준오, 정승규는 본 연구에서 모든 자료에 접근할 수 있으며, 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습 니다. 연구 기획 : 남명은, 홍상덕, 박준오, 정승규. 자료 해석 및 분 석 : 남명은, 홍상덕, 박준오, 정승규. 논문초안 : 남명은, 홍상덕, 연 구 총괄 : 정승규.
Fig. 3. Fungal hyphae (black) at microscopic view. (with Gro- cott’s methenamine silver stain)
Fig. 5. Preoperative coronal CT scans: Filling defects in the max- illary bone (white arrow).
Fig. 4. Gutta-Percha cone that was removed during the opera- tion (top), and an unused Gutta- Percha cone (botom).
Nam et al : Gutta-Percha induced sinusitis / 129
REFERENCES
1) Mensi M, Piccioni M, Marsili F, Nicolai P, Sapelli PL, Latronico N.
Risk of maxillary fungus ball in patients with endodontic treatment on maxillary teeth: a case-control study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:433-6.
2) Beck-Mannagetta J, Necek D. Radiologic findings in aspergil- losis of the maxillary sinus. Oral Surg Oral Med Oral Pathol 1986;62:345-9.
3) De Foer C, Fossion E, Vaillant JM. Sinus aspergillosis. J Crani- omaxillofac Surg 1990;18:33-40.
4) Kopp W, Fotter R, Steiner H, Beaufort F, Stammberger H. Asper- gillosis of the paranasal sinuses. Radiology 1985;156:715-6.
5) Krennmair G, Lenglinger F. Maxillary sinus aspergillosis: diag- nosis and differentiation of the pathogenesis based on computed tomography densitometry of sinus concretions. J Oral Maxillofac Surg 1995;53:657-63; discussion 63-4.
6) Legent F, Billet J, Beauvillain C, Bonnet J, Miegeville M. The role of dental canal fillings in the development of Aspergillus sinusitis.
A report of 85 cases. Arch Otorhinolaryngol 1989;246:318-20.
7) Park GY, Kim HY, Min JY, Dhong HJ, Chung SK. Endodontic treatment: a significant risk factor for the development of maxillary fungal ball. Clin Exp Otorhinolaryngol 2010;3:136-40.
8) Ishikawa M, Mizuno T, Yamazaki Y, Satoh T, Notani K, Fukuda H.
Migration of gutta-percha point from a root canal into the ethmoid sinus. Br J Oral Maxillofac Surg 2004;42:58-60.