online©ML Comm
- 152 -
J Rhinol 16(2), 2009 www.ksrhino.or.kr
A Case of Endoscopic Marsupialization of a Nasopalatine Duct Cyst
Young-Gi Cinn, MD, Moo-Kyun Park, MD, Hee Joon Kang, MD, PhD and Heung-Man Lee, MD, PhD
Department of Otorhinolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, Korea
ABSTRACT
Nasopalatine duct cysts (NPDC) are common cystic lesions of non- odontogenic origin of the maxilla. Patients with NPDC generally undergo surgical enucleation via transoral approach. However, with the recent introduction of sinonasal endoscopy and subsequent advances in surgical techniques, endoscopic management has become possible. This study reviews a case of a 40- year-old man had a one-month history of nasal obstruction and swelling of the hard palate. Nasal endoscopy revealed a cyst in the nasal floor and hard palate. He underwent successful endoscopic marsupialization of NPDC. This simple and less invasive surgical procedure should be considered in the future treatment of NPDC.
KEY WORDS
: Nasopalatine duct cyst·Nasal endoscopy·Endoscopic marsupialization.
INTRODUCTION
Nasopalatine duct cyst (NPDC) is a common nonodont- ogenic cyst of the oral cavity. It forms within the incisive ca- nals behind the alveolar process of the palatine bone or in the soft tissue of the palate where the canal opens. It is tho- ught to originate from oronasal ducts present within the incisive canals.
1)Presentation may be asymptomatic or includes swell- ing, pain, and drainage from the hard palate. A well-circum- scribed, round, ovoid, or heart-shaped radiolucent lesion in the midline of the maxilla is seen on computed tomographic (CT) scan of paranasal sinuses. Pathological findings re- veal squamous or respiratory cell types infiltrated by inflam- matory cells.
2)Most of the patients with NPDC have been advised to have surgical excision in the form of enucleation via the transo- ral approach. Although the results of treatment are gener- ally good with low recurrence rates, hematoma, wound de-
hiscence, and persistent oronasal fistula develop in some pa- tients.
3)4)We present a case of NPDC treated with transna- sal endoscopic marsupialization.
CASE REPORT
A 40-year-old man presented with a one-month history of nasal obstruction. He had been treated for chronic par- anasal sinusitis at other hospitals and was referred to our hospital for further examination. There was no previous his- tory of trauma to produce these symptoms. He presented with complaints of nasal obstruction and hard palate swel- ling. On palpation the lesion was elastic, soft, slightly ten- der, and somewhat fluctuant. The overlying mucosa ap- peared normal in color. Teeth in the anterior maxilla were vital and not carious. Nasal endoscopy revealed swelling in the nasal floor and hard palate(Fig. 1). The nasal floor and anterior half of the hard palate surrounding the cyst- like lesion were expanded, and the thin cortical bone in these regions remained. There was a round, clearly bordered radi- olucent area in the midline of the anterior premaxilla and its greatest diameter was 2.7 cm on CT scan of the paran- asal sinuses(Fig. 2). Fine needle aspiration demonstrated a straw-colored fluid with no evidence of malignancy. All other physical and laboratory findings were normal. A pro- visional diagnosis of an NPDC was made.
Address correspondences and reprint requests to Heung-Man Lee, M.D., Ph.D., Department of Otolaryngology-Head and Neck Surgery Korea University College of Medicine, 80 Guro-dong, Guro-gu, Se- oul 152-703, Korea
Tel : 82-2-2626-3185, Fax : 82-2-868-0475 E-mail : [email protected]
Received for publication on February 3, 2009
Accepted for publication on April 8, 2009
Cinn et al:Endoscopic Marsupialization of Nasopalatine Duct Cyst / 153
The patient underwent operation under general anesth- esia. In particular, he underwent marsupialization at the roof of the cyst into the left nasal cavity through an endos- copy-guided transnasal approach. The mass was succes- sfully marsupialized with the nasal endoscopic technique.
There were some crust and discharge in the left nasal cavi- ty after 2 weeks of operation. Histologic examination re- vealed a combination of squamous and respiratory epithe- lium with an inflammatory infiltrate compatible with NPDC.
Follow-up nasoendoscopic examinations have been per- formed with no sign of recurrence one year after surgery ( Fig. 3).
DISCUSSION
NPDC is classified among the epithelial nonodontogen- ic cysts according to the 1992 WHO histological typing of odontogenic tumors. NPDC is a common nonodontogenic cyst, occurring in approximately 1% of the general popula- tion.
5)The origin of NPDC was previously thought to be the entrapment of remnants during embryologic fusion;how-
ever, it is currently thought to originate from oronasal ducts within the incisive canal. The exact trigger that stimulates the development of the cysts has been theorized by sev- eral different authors. No definitive etiological factor has been identified. Factors that have been proposed include trauma, infection, and spontaneous proliferation.
6)It has been reported that the overall mean age of the patient at diagnosis of NPDC is 37.4 or 42.5 years. It has a slight male predilection, although it may present clinically at any age.
7)Many patients present without symptoms. When symp- toms are present, swelling is most commonly reported. As- sociated pain was thought to be secondary to concomitant infection. NPDC sometimes gives rise to acute infection, enlargement, and penetration through the overlying mu- cosa.
8)9)NPDC is typically recognized as a swelling in the midline of the anterior hard palate and sometimes exists in a relatively posterior hard palate. These patients are of- ten first recognized by either the dentist or primary phy-
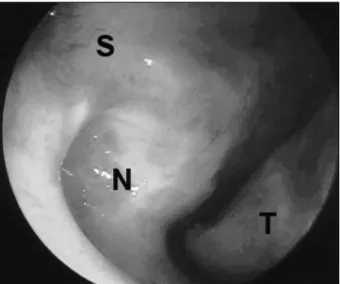
Fig. 1. Nasal endoscopic finding revealed the floor of the left- side nasal cavity to be elevated posteriorly and the nasal sep- tum deviated to the right. S:nasal septum, N:nasopalatine duct cyst, T:inferior turbinate.
Fig. 2. Coronal (A), axial (B) and sagittal (C). Computed tomographic scan of paranasal sinuses demonstrating a midline ovoid cystic lesion of the premaxilla.
A B C
Fig. 3. Nasal endoscopy revealed complete epithelialization at about one 1 year after marsupialization and no evidence of recurrence of the cyst. S:nasal septum, N:nasopalatine duct cyst, T:inferior turbinate.
154 / J Rhinol 16(2), 2009
sician and are subsequently referred for further diagnosis and treatment. Fistula formation or drainage or both were seen in up to 25% of patients in one large study.
4)There have been various types of masses described on the palate, including salivary gland tumors such as pleomorp- hic tumors;benign tumors, such as fibromas or granulo- ma;and various cysts. It is often difficult to differentiate NPDC from other types of tumors, regardless of fluctua- nce, especially at the posterior hard palate. When teeth ap- pear to be devitalized, a periapical lesion of the upper in- cisor must be ruled out as the correct diagnosis.
10)NPDC is diagnosed when plain radiography reveals a well-defined round unilocular radiolucency including the incisive canals in the palatal region. Conventional radiog- raphy is unable to reveal adequate information about the upper extension of the lesion. CT scan is often performed to obtain such information.
Aspiration of pathologic jaw radiolucencies can pro- vide useful information in distinguishing solid processes from cystic processes. Although a clear or straw-colored fluid aspirate is suggestive of NPDC, other cystic proces- ses such as lateral radicular cyst or cystic ameloblastoma cannot be excluded on the basis of this finding alone.
Bloody fluid is more indicative of a central hemangioma, a central giant cell lesion, an arteriovenous malformation, or an aneurysmal bone cyst. Negative aspiration indicates a solid process such as odontogenic myxoma or a solid ameloblastoma.
Both respiratory and squamous epithelium can be seen at the time of pathological diagnosis. The distribution of types of epithelium seen in NPDC depends on the proxim- ity to the nasal cavity. Respiratory epithelium is seen supe- riorly, followed by cuboid and then by squamous epitheli- um inferiorly, to the oral cavity. A large percentage of spec- imens also reveal the presence of nerves and blood ves- sels, because these structures often course the incisive ca- nal.
2)Of the reported cases in which surgical treatment was discussed, all but two were treated by enucleation.
3)Since squamous cell carcinoma in the maxilla originating from NPDC was also reported, NPDC should be treated even if it is only a small lesion. Marsupialization of the cyst ver- sus enucleation is also an accepted treatment and is even recommended for larger cysts, especially if the surgeon is
worried about the formation of a persistent fistula. No ab- solute size parameters or radiological findings have been established to date to specify which approach will best se- rve an individual patient. Therefore, surgeons should con- tinue to evaluate patients on a case-by-case basis. Ulti- mately, the decision to surgically treat suspected NPDC based on clinical impression is left to the patient and doc- tor. When symptoms are present, the standard of care is excision.
The advent of endoscopic surgical techniques provides another surgical approach for the treatment of NPDC. As a more convenient, effective, and safer method compared with the conventional method, the method of marsupializa- tion using a nasal endoscope can reduce morbidity and the hospitalization period.
3)6)11)Acknowledgments
This study was supported by a grant of the Korea Healthcare technol- ogy R&D Projects, Ministry for Health, Welfare & Family Affairs, Re- public of Korea(A090784).
REFERENCES
1) Gnanasekhar JD, Walvekar SV, al-Kandari AM, al-Duwairi Y.
Misdiagnosis and mismanagement of a nasopa-latine duct cyst and its corrective therapy: a case report. Oral Surg Oral Med Oral Pa- thol Oral Radiol Endod 1995;80:465-70.
2) Allard RB, Van Der Kwast WM, Van Der Waal I. Nasopalatine duct cyst: review of the literature and report of 22 cases. Int J Oral Surg 1981; 10:447-61.
3) Elliott KA, Franzese CB, Pitman KT. Diagnosis and surgical man- agement of nasopalatine duct cysts. Laryngoscope 2004;114(8):
1336-40.
4) Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst:
an analysis of 334 cases. J Oral Maxillofac Surg 1991;49:268-71.
5) Anneroth G, Hall G, Sturge U. Nasopalatine duct cyst. Int J Oral and Maxillofac Surg 1986;15:572-80.
6) Vasconcelos RF, Ferreira de Aguiar MC, Castro WH, Cavalcanti de Araujo V, Mesquita RA. Retrospective analysis of 31 cases of naso- palatine duct cyst. Oral Dis 1999;5:325-8.
7) Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology (ed 3).
Philadelphia, Saunders WB;1974.
8) Staretz LR, Brada BJ, Schott TR. Well-defined radiolucent lesion in the maxillary anterior region. J Am Dent Assoc 1990;120:335-6.
9) Hedin M, Klanfeldt A, Persson G. Surgical treatment of nasopala- tine duct cysts: a follow-up study. Int J Oral Surg 1978;7:427-33.
10) Wood NK, Doaz PW. Differential Diagnosis of Oral Lesions (ed 4).
Saint Louis, Mosby;1991.
11) Shin HW, Cha WJ, Kim IK, Jin HR. An infected median palatine cyst: report of a rare entity. Korean J Otorhinolaryngol-Head Neck Surg 2007;50:1058-61.