online©ML Comm
-
128
-J Rhinol 14(2), 2007 www.ksrhino.or.kr
비강에 발생한 방선균증 1예
성균관대학교 의과대학 강북삼성병원 이비인후과학교실
최현진·이종규·권희준·이경철 A Case of Actinomycosis in Nasal Cavity
Hyun-Jin Choi, MD, Jong-Kyu Lee, MD, Hee-Jun Kwon, MD and Kyung-Chul Lee, MD
Department of Otolaryngology, Kangbuk Samsung Hospital, School of Medicine, Sungkyunkwan University, Seoul, Korea
ABSTRACT
Actinomycosis is a rare form of disease which is caused by Actinomyces such as A. israelii and A. bovis. These anaerobic gram-positive organisms may take the form of an acute or a subacute disease progression. Only a few cases of actinomycosis in the nasal cavity have been reported previously. Actinomycosis is difficult to diagnose because of the fastidious nature of the organism in culture and a general lack of familiarity with the disease. In this paper, we report a case of actinomycosis pre- senting nasal cavity mass without prior mucosal trauma. Our patient had endonasal endoscopic removal of infected tissue and was treated with 2 days of intravenous antibiotics and 3 weeks of oral antibiotics therapy without any evidence of recurrence.
KEY WORDS
:Actinomycosis·Nasal cavity.
서 론
방선균증(Actinomycosis)은 주로 구강 및 경부, 호흡기, 소화관 등에 존재하는 그람 양성 혐기성 정상 상재균인 A.
israelii, A. bovis 등이 단백질 분해효소로 점막을 통과한 후 연부조직으로 침습하는 드문 만성 감염성 질환으로, 현미 경적으로 유황과립(sulfur granule)을 함유하는 종괴나 농 양을 형성하는 특징을 가지며, 주로 두경부 영역에 발생하는 것으로 알려져 있다.1)2) 이중 비인강과 비강에서 발생된 방 선균증은 매우 드물며 국내외적으로 각각 2예만이 보고되 었다.2-5)
저자들은 좌측 비강에서 우연히 발견된 종물이 조직학적 으로 방선균증으로 확진된 비강 내 방선균증 1예를 치험하 였기에 문헌고찰과 함께 보고하는 바이다.
증 례
24세 여자환자가 상기도 감염으로 개인병원에 방문하여
우연히 발견된 좌측 비강의 종괴를 주소로 전원되었다. 비 루나 코막힘 등의 증상은 없었으며, 구강 및 치아치료 등을 포함한 점막 손상을 일으킬 만한 병력은 없었고 코에 이물 질을 넣었거나 들어갔던 병력도 없었다. 이학적 소견 상 좌 측 비강의 비중격과 하비갑개 사이에 회갈색의 종괴가 관 찰되었고 표면은 거칠었으며 부서지기 쉬워 보이는 모양이 었다(Fig. 1). 그 외에 구강 및 구인두, 하인두, 후두, 경부에 특이소견은 없었다.
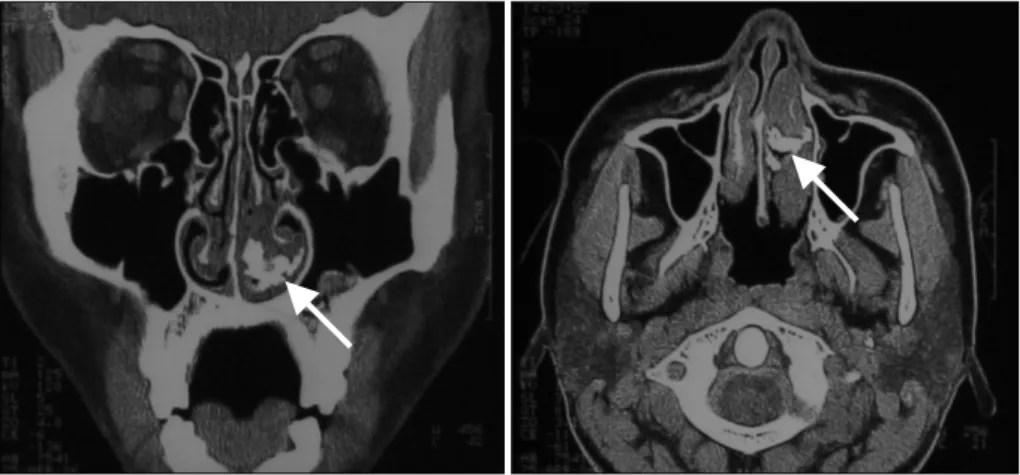
부비동 전산화 단층 촬영상 좌측 비강의 비중격과 하비갑 개의 후하방 사이에서 하비갑개를 바깥 방향으로 밀고 있는 고도로 석회화된 고음영의 종괴가 관찰되었고 주위 부비동 에서 특별히 관찰되는 병변은 없었다(Fig. 2).
치료 및 조직학적 확진을 위해 비내시경 하에서 종괴를 제 거하였다. 종괴는 하비갑개의 비점막과 쉽게 분리되었으며, 하비갑개 및 하비갑개 주위에 특별한 이상소견은 없었다. 병 리 조직학적 검사에서 특징적인 유황과립을 가지는 만성 염 증소견으로 방선균증이 확인되었다(Fig. 3).
수술 후 정맥으로 Augmentin 1.2 g을 하루 3회 2일 간 투 여하였으며 환자는 특별한 합병증 없이 수술 후 2일째에 퇴 원하였고, 퇴원 후 경구 Augmentin을 하루 3회 3주간 투여 하였다.
환자는 수술 후 3주까지 재발소견 보이지 않아 항생제 투 논문접수일:2007년 5월 28일 / 심사완료일:2007년 7월 23일
교신저자:이경철, 110-746 서울 종로구 평동 108번지 성균관대학교 의과대학 강북삼성병원 이비인후과학교실 전화:(02) 2001-2264·전송:(02) 2001-2273 E-mail:[email protected]
최현진 등:방선균증 치험 1예 / 129
여를 중단하고 6개월째 경과관찰 중이며 현재 비내시경 검 사상 비강점막 상태는 정상으로 합병증이나 재발 없이 추적 관찰 중이다.
고 찰
방선균은 동물과 인간에서 만성 화농성 감염을 일으키며 캡슐과 포자없이 세포 내에 존재하는 그람 양성 혐기성 박 테리아로, 건강한 사람에서 주로 편도나 치아 표면에 존재하 며 타액선이나 경부, 안면, 소화기, 호흡기 계통에 감염을 일 으킨다.6) 두경부 병변의 발생은 주로 외상, 수술 등에 의 해 정상 점막의 손상으로 방선균이 혐기성 환경에 유입되 어 증식이 활발하게 될 때 일어난다.6)7) 그러나 본 증례에 서는 점막 손상을 일으킬 만한 특별한 선행 요인이나 병력 이 없었다. 가장 흔한 원인균은 Actinomyces israelii 이며, 이 외에 A. viscous, A. odontolyticus, A. naeslundii 등이 있
다.1)6)8) 호발 연령은 30~60대의 중년층 이상이 대부분을 차
지하며 발생 부위는 두경부에 55%, 복부 20%, 흉부 15%, 기타부위 10%로 보고되어 있고,6)9) 진단은 일반적으로 배 양 결과 방선균이 검출되고 병리조직학적으로 만성 육아종 성 염증소견을 보이면서 특징적으로 병변 내에 유황과립이 존재할 때 진단할 수 있지만, 방선균증이 강하게 의심되는
Fig. 2. PNS CT shows the high density calcified lesion between the nasal se- ptum and left inferior turbinate (arr- ows).
Fig. 1. Endoscopic view of the left nasal cavity shows a whitish- brown granular mass between the nasal septum and inferior turbinate (arrow).
Fig. 3. Histopathologic finding shows characteristic sulfur gra- nules with chronic inflammation (arrow)(H & E stain, ×400).
Fig. 4. Endoscopic view of the left nasal cavity shows normal mucosa (2 weeks after the operation).
130 / J Rhinol 14(2), 2007
검체에서도 50% 이하에서만이 균이 동정되고 유황과립은 검체의 30%에서만 존재하므로 진단을 내리기 어려운 경우 가 있다.4)6)10)
치료는 약물 요법과 수술 요법이 있는데, 약물요법으로는 고용량의 penicillin 정맥주사와 amoxicillin 경구용 항생제 가 추천되고 있으며, 투여 기간에 대해서는 여러 가지 의견 이 있으나 감염의 중증도에 따라 2~6주간의 정맥주사 후 2~12개월간의 경구용 amoxicillin 복용이 일반적으로 통용 되고 있다.6)10-12) 그러나 주변의 심한 섬유화를 동반하고 혈 류량이 적어 항생제의 침투가 어려운 방선균증의 특성 때문 에 고용량, 장기간의 항생제 투여가 필요하다.6)13) 따라서 만 성적이며 항생제에 잘 반응하지 않은 방선균증의 경우 수 술적 요법과의 병합이 강조되어 왔다.6)13)14) Martin,11)15) King- dom과 Tami14)는 두경부 방선균증에서 수술적 요법과 경구 용 항생제 요법을 병행하여 좋은 결과를 보고한 바 있다. 본 증례에서는 비내시경적 접근법으로 비강내 종괴을 충분히 제 거한 후 2일간의 정맥내 항생제 주사와 3주간의 경구약물요 법 시행 후 재발없이 성공적으로 치료되었다. 기존 문헌과 비 교해 볼 때 항생제 사용 기간이 짧았지만 재발없이 성공적으 로 치료되었는데 이는 환자의 비강에서 발견된 종괴가 주변 조직으로의 침습없이 비강 내에만 국한되어 있었으며 주변 조직과 유착이 심하지 않아 비내시경하에서 수술적으로 쉽 게 제거될 수 있었기 때문인 것으로 생각된다. 따라서 비강 에 국한된 방선균증의 경우 비내시경적 병변 절제와 amoxi- cillin 경구 투여가 먼저 고려되어야 할 것으로 생각되며 또 한 완치를 위한 항생제 투여기간에 대해서는 병변의 위치 와 주변 조직으로의 침습여부 및 정도에 따라 결정되어야 할 것으로 생각된다.
중심 단어:방선균증·비강.
REFERENCES
1) Choi JW, Lee TB, Hwang SH, Kim BH. A rare case of actinomy- cosis in nasal cavity with aspergillus sinusitis. Korean J Otolaryn- gol 1997;40:1844-7.
2) Kim YH, Lee HS, Kang KH, Jung DH, Kim CG. A rare case of actinomycosis of the submandibular gland. Korean J Otolaryngol 1989;32:1205-7.
3) Osborne JE, Blair RL, Christmas HE, McKenzie H. Actinomycosis of the nasopharynx: A complication of nasal surgery. J Laryngol Otol 1988;102:639-40.
4) Scott A, Stansbie JM. Actinomycosis presenting as a nasopharyn- geal tumour: A case report. J Laryngol Otol 1997;111:163-5.
5) Roth M, Montone KT. Actinomycosis of the paranasal sinuses: A case report and review. Otolaryngol Head Neck Surg 1996;114:
818-21
6) Bennhoff DF. Actinomycosis: Diagnostic and therapeutic consider- ations and a review of 32 cases. Laryngoscope 1984;94:1198-217.
7) Burns BV, Ayoubi AL, Ray J, Schofield JB, Shotton JC. Actinomy- cosis of the posterior triangle: A case report and review of the literature. J Laryngol Otol 1997;111:1082-5.
8) Hong SJ, Joo JB, Kim YJ, Lee BJ. Three cases of actinomycosis of the head and neck. Korean J Otolaryngol 2000;43;1259-62.
9) Richtsmeier WJ, Johns ME. Bacterial causes of granulomatous dis- ease. Otolaryngol Clin North Am 1982;16:478-84.
10) Fradis M, Zisman D, Podoshin L, Wellisch G. Actinomycosis of the face and neck. Arch Otolaryngol 1976;102:87-9.
11) Martin MV. The use of oral amoxicillin for the treatment of actino- mycosis. Br Dent J 1984;156:252-4.
12) Lad SD, Chandy MJ. Craniofacial actinomycosis. Br J Neurosurg 1991;5:361-70.
13) Weese WC, Smith IM. A study of 57 cases of actinomycosis over a 36-year period. A diagnostic ‘failure’ with good prognosis after tre- atment. Arch Intern Med 1975;135:1562-8.
14) Kingdom TT, Tami TA. Actinomycosis of the nasal septum in a pa- tient infected with the human immunodeficiency syndrome-related complex. Arch Otolaryngol Head Neck Surg 1994;111:130-3.
15) Martin MV. Antibiotic treatment of cervicofacial actinomycosis for patients allergic to penicillin: A clinical and in vitro study. Br J Oral Maxillofac Srug 1985;23:428-34.