- 57 -
Total Septal Cartilage Reconstruction in the Severely Deviated Nose
Hun-Jong Dhong, M.D. and Byung-Sik Kim, M.D.
ABSTRACT
Background and Objectives:Surgical correction of the severe septal deviation associated with the twisted nose is a difficult surgical challenge. Many maneuvers have been devised to correct and maintain correction of a severely deviated nose, especially a deviated caudal septum or a dorsally deviated L-shaped strut. But few of these reported techniques have corrected and maintained correction satisfactorily. Total septal cartilage reconstruction is a technique by extramucosal excision of the cartilaginous septum (total harvest of deviated septum) and replacement as a free graft (reinsertion of surgically straighten septum). We evaluated the validity of total septal cartilage reconstruction with regard to functional results as well as aesthetic results. Materials and Methods:This retrospective study reviewed the patients’ records in case of total septal cartilage reconstruction for a severely deviated nose. Information included the patient's age, sex, pre/postoperative gross view, pre/postoperative acoustic rhinometry, and subjective satisfaction rate as well as complications. Ten patients underwent total septal cartilage reconstruction from 1996 to 1999. Their age ranged from 17 to 46 years. 8 patients were men and 2 patients were women. Results:All patients noted marked improvement of nasal blockade. Aesthetic improvement of the nose was obtained in all patients. No infections, hematoma, graft extrusions, saddle nose deformity, or distortion occurred in this series. Conclusion:Total septal cartilage reconstruction is a good technique suitable for those patients in whom severe obstruction, especially high in the vault in combination with severe deviation of the external nose so that more conservative techniques are insufficient to achieve the desired results.
KEY WORDS:Deviated nose·Septoplasty·Total septal reconstruction.
INTRODUCTION
Nasal septal deviation is a common disease but corr- ection of highly severe cases, which cause deformity of the external nose, is not easy. These cases usually come with nasal obstruction, thus functional and aesthetic as- pects should both be considered. Traditional surgical co- rrection based on septoplasty has not been applied part- icularly when the nasal valve becomes narrower due to deviation of the nasal dorsum or when the nasal vestibule is blocked by deformity of the caudal end of the nasal septum. Preservation of the L-shaped strut, which refers to anterior part of the vertical line linking the rhinion
and the anterior nasal spine, is known to be important because when it is removed it may result in a deformity such as saddle nose.1) As a result, correction of severe deviation in the cartilaginous part of the L-shaped strut is usually made in a passive manner with anxiety on the postoperative deformity. This, though, will lead to ina- dequate improvement of nasal obstruction functionality and unsatisfactory aesthetic results. When the nasal do- rsum is severely deviated, causing scoliotic nose, the bony septum can be corrected by using the osteotomy.2)3)
But in cases of cartilaginous septum, severe deviat- ion is difficult to correct with the existing method us- ing spreader graft.4) Due to these difficulties, correction of nasal septal deviation accompanying nasal dorsum deviation has been a challenge to many surgeons. In this respect, total septal cartilage reconstruction in wh- ich the nasal septal cartilage is all harvested to be re- modeled and then reinserted between the mucoperic- hondrium of the nasal septum is effective in cases of severe deviation in the nasal dorsum or the caudal end of the nasal septum. This study is to examine the ef- fectiveness of total septal cartilage reconstruction by applying it to patients with severe deviation in the na- Department of Otorhinolaryngology-Head and Neck Surgery,
Sungkyunkwan University School of Medicine, Samsung Medi- cal Center, Seoul, Korea
Address correspondences and reprint requests to Hun-Jong Dhong, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, Sungkyunkwan University School of Medicine, Samsung Medical Center, Seoul 135-710, Korea
Tel:82-2-3410-3579, Fax:82-2-3410-3879 E-mail:[email protected] Accepted for publication on April 4, 2000
sal dorsum and the caudal end of the nasal septum for the last four years.
MATERIALS AND METHODS
10 patients who had total septal cartilage reconstruc- tion from 1996 to 1999 in the department of Otorhinol- aryngology-Head and Neck Surgery, Samsung Medical Center in Seoul were collected (Table 1). All of them showed scoliotic nose, two of them with saddle nose at the same time. Eight were men and two were women with an average age of 25.3, ranging from 17 to 46 ye- ars of age. Under general anesthesia, total septal cartilage reconstruction was carried out;eight of them had ost- eotomy and the two who had saddle nose were treated with augmentation rhinoplasty at the same time. Posto- perative improvement of nasal obstruction and aesthetic satisfaction were measured with a visual analogue scale and objective changes were measured using acoustic rh- inometry. Through a retrospective study on patients’ me- dical records, changes of their external nose and occu- rrence of any complications were checked. Outpatient follow-up was carried out for 34 months on average, ranging from 7 months to 49 months.
Surgical technique
A hemitransfixion incision is made 1-2 mm behind of the caudal end of nasal septum to expose the entire nasal septal cartilage and the maxillary crest at the inf- erior part. The incision is usually taken on the concave side of the deviation, but it will be easier for a right-
handed person to make the incision on left side. After exfoliating the mucoperichondrium from the nasal sep- tal cartilage, the anterior and inferior tunnels are made along the dissection plane. By extending the dissection plane of the anterior nasal septum to the posterior part, the anterior tunnels should be extended in the direction of the nasal dorsum, passing the cartilaginous part and bony part. Then the posterior chondrotomy is conducted and the basal area of the nasal septum is separated from the anterior nasal spine, premaxillary, and maxillary crest.
The nasal septal cartilage is separated from the upper and lower lateral cartilage by using a Beaver knife or Freer elevator to completely remove the nasal septal ca- rtilage from surrounding structures and take it out to the
Table 1. Patient profile of total septal cartilage reconstruction Case Sex/age External
deformity
Combined operation method 1 M/25 scoliotic nose osteotomy 2 M/30 scoliotic nose osteotomy 3 M/19 scoliotic nose osteotomy 4 M/17 scoliotic & saddle
nose
osteotomy &
augmentation*
5 F/23 scoliotic & saddle nose
osteotomy &
augmentation* & tip† 6 M/19 scoliotic nose osteotomy
7 F/29 scoliotic nose
8 M/19 scoliotic nose osteotomy 9 M/46 scoliotic nose
10 M/25 scoliotic nose osteotomy
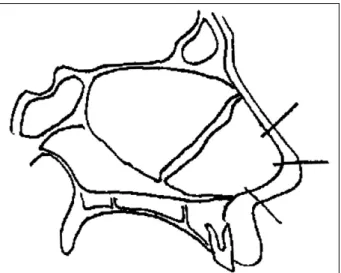
*:augmentation rhinoplasty, †:tip surgery Fig. 2. Remodelling of nasal septum.
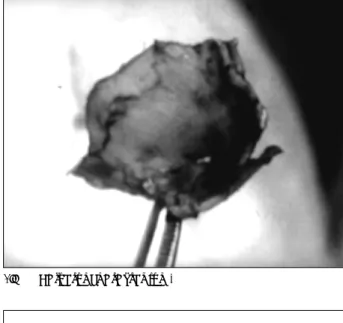
Fig. 1. Harvest of nasal septum.
nasal cavity (Fig. 1).
After measuring the removed nasal septum in vari- ous directions, it is cut to make a new L-shaped strut.
If necessary, the conchal cartilage can be added as gr- aft or suturing is made (Fig. 2). The height of caudal end of transplant should be around 25 mm, with V-C angle (ventro-caudal corner) of around 110 degree, in order to prevent the postoperative deformity of saddle
nose or in the nasal tip. The nasal septal graft is rein- serted into the original location and fixed by suturing in three places;one in the nasal dorsum, the other in the nasal tip and finally in the basal area by piercing the external nose (Fig. 3). Finally, to enhance stability and survival of the nasal septum and prevent hemato- ma, a through-and-through suture of the nasal septum should be made.
RESULTS
All of the 10 patients came to the hospital with a main complaint of nasal obstruction, which was too se- vere to maintain normal life, as recorded in a new pat- ient questionnaire of the hospital. In seven patients, the one-side nasal cavity was almost obstructed due to na- sal septal deviation on the physical examination and nine of them showed a narrower nasal valve from the nasal dorsum deviation. All of them had accompanying scoliotic nose in the external nose (Fig. 4). The ten pa- tients were treated with total septal cartilage reconstr- uction and of the eight who were able to answer a qu- estionnaire, we studied their subjective satisfaction by using a visual analogue scale.
Fig. 3. Reinsertion of the cartilaginous plate and fixation.
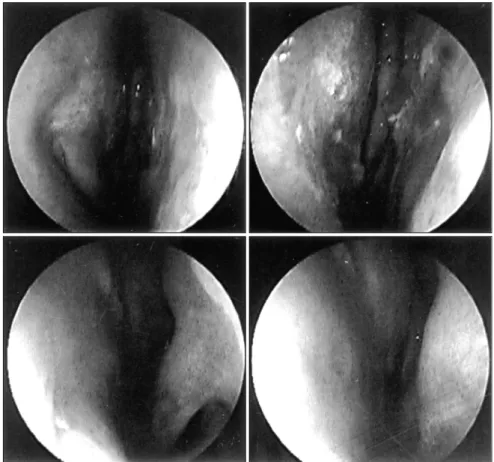
Fig. 4. Preoperative view of a 28-year-old patient with severe right nasal obstruction and scoliotic nasal deformity. Observe severely narrowed right nasal cavity.
When the optimal satisfaction is set at 100, the aest- hetic satisfaction degree was 83.3 on average, ranging from 70 to 90, while their subjective satisfaction on re- spiratory function was 93.3, ranging from 80 to 100, a relatively high degree (Fig. 5). On the physical exam- ination, the preoperative severe nasal septum deviation is confirmed to be almost corrected (Fig. 6). To check objective changes, acoustic rhinometry was conducted before and after the operation and results were obtained from four patients. To avoid variables other than analysis of the difference between the right and the left, analyses were made on the status after spraying a vasoconstrictor and the results were taken from the narrower nasal cav- ity only (Table 2).5)
Analyses on pre/postoperative examinations show in- crease of nasal cavity volume by 86.75% on average, ranging from 57.3% to 112.8%. The minimum cross- sectional area, which is used for determining the volume of the nasal valve, also is increased by 157.4% on aver- age, ranging from 62.7% to 300%. The difference bet-
ween the left and the right side also improved by 88%
on average, ranging from 65% to 99%, proving that the difference is almost gone after the operation. In all pati- ents, complications such as postoperative infection, hem- atoma, graft extrusion, saddle nose or nasal tip deformity were not found. Throughout the outpatient follow-up period, which ranged from 7 months to 49 months, 34 months average, deformity of the nasal septum over time was not found.
DISCUSSION
By far, various surgical methods have been developed for correction of nasal septum deviation and of them, septoplasty is the most widely used. The submucous re- section (SMR), which was presented by Killian and Freer in 1904, is difficult to apply in cases of deviation of the marginal area. It often causes nasal septal perfo- ration and deformity of the external nose, which results in change of the physiological status of the nasal cavity.
It is also difficult to dissect septal mucosa again when septal cartilage was removed in previous SMR. To sup- plement this, Cottle, et al., introduced the septoplasty in 1947 which removes the excessively grown cartilag- inous part or fractured cartilage only without making the dissection of the one-side mucoperichondrium of the na- sal septal cartilage. This maintains the blood supply to the cartilaginous part to minimize absorption and also stabilize and maintain the position of the nasal septum which features mobilization.7)
In conducting the septoplasty, it is very important to maintain the L-shaped strut to prevent saddle nose or postoperative deformity of the nasal tip but practically it has been a challenge because patients with severe na- sal septal deviation have often shown deviation in the L-shaped strut itself. When there is deviation in the ca- udal end of the nasal septum, corrections have been made
Table 2. Acoustic rhinometry measurements taken in both nasal cavities of 4 patients
Preoperative Postoperative Case
Vol (small)* Vol (large)* MCA† Vol (small) Vol (large) MCA Diff‡
1 4.67 12.48 0.16 9.80 10.99 0.64 99
3 6.77 11.71 0.26 10.65 11.16 0.51 89
7 6.47 9.94 0.59 10.73 10.80 0.96 65
9 4.69 7.71 0.24 8.6 9.98 0.65 98
*:volume (cm3) in small/large nasal cavity, †:minimal cross-sectional area (cm2) in small nasal cavity, ‡:Improvement scale (%) of volume differences between right and left nasal cavity. {Preop (volume differences between right and left nasal cavity)-Postop (volume differences between right and left nasal cavity)}/Preop (volume differences between right and left nasal cavity)×100
Fig. 5. Subjective satisfaction rate of postop states with regard to functional and aesthetic results (visual analogue scale).
by using the swing door technique which has been dev- eloped by Becker8) and Smith9) and the spreader graft application. There came relatively good results in cases of angular deviation in the caudal end of the nasal septum, but in cases of curved deviation, making the correction was difficult using those techniques.7) Peer10) and Mali- niac11) devised a technique which removes the deviated part of the L-shaped strut of the caudal end of the nasal septum and split it into fine pieces to retransplant in the columella bed. But this will eventually weaken the car- tilaginous part, and with the passage of time nasal septal deviation can reoccur due to the memory phenomenon where the remaining nasal septum is deviated again. Th- erefore it is hard to predict the results of the technique.12) To complement this, a technique which added spreader graft after correction of nasal septal cartilage has been attempted many times4) but this can be applied only to cases with a minor degree of deviation. Even in cases of nasal dorsum deviation, correction based on the swing door flap is possible in part if the L-shaped strut is angular.12)
But when the deviation is severe or in cases of curved deviation, the technique is not sufficient for correction.
Some attempted correction by placing multiple through- and-through incisions (cross-hatching) into the cartila- ginous part, but it is also hard to predict the result, thus sometimes results in either under-correction or someti- mes in over-correction. Therefore, correction of such severe nasal septal deviation including the L-shaped st- rut has been a big challenge to surgeons. Major challe- nges were correction of the deviated nasal septum while avoiding deformity of the nasal septum and external nose.
For this, Jost and Legent,13) Denecke and Meyer,14) and Rees12) developed total septal cartilage reconstruction technique through which the deviated nasal septum is completely taken out from the nasal cavity to transform into a totally new septum through incision or suture, and the new septum is then connected to skin of the na- sal dorsum with suturing thread to maintain support of the L-shaped strut. Total septal cartilage reconstruction allows correction, which was not available with traditi- onal techniques, while preserving the nasal septal carti-
Fig. 6. Postoperative view of nasal cavity with straightened nasal septum.
lage, which prevents the sinking of the nasal septal mu- cosa which can other-wise occur when the cartilaginous septum is removed.
It also generates fewer nasal septal perforations and causes less contraction of the nasal septal mucosa which facilitates operation in case of resurgery. Severely devi- ated nasal septum often comes with deviation of nasal bone or bony septum, or cartilaginous parts of small size.
This can be treated by making a partial incision of the perpendicular plate of the ethmoid, making a new carti- lage-bone nasal septum through suturing with the carti- laginous part and positioning it in the cartilaginous part of the nasal septum. We applied this technique to a pat- ient and succeeded in reconstruction without any parti- cular problems. Ten patients who had total septal cartilage reconstruction revealed functional improvement in the subjective view and high satisfaction with the aesthetic result. Those results were also supported by objective studies using acoustic rhinometry. But this method is more invasive compared to existing ones and requires longer surgery time, which may cause higher morbidity of patients.
Thus surgeons are required to get used to the techni- que sufficiently to reduce postoperative complications such as saddle nose or deformity of the nasal tip. Gene- rally, it is known that smoother blood supply is available to the cartilage when the nasal septal mucosa of one-side cartilage is preserved during the nasal septum surgery.
Accordingly, there is a concern that this technique, which dissects mucosa of both sides, may cause sinking of nasal septum due to necrosis of the cartilaginous part over time. But according to Rees,12) who followed up patients for 15 years maximum, 22 out of 25 patients obtained highly satisfactory results without any deformity with time passage, and the remaining three also required re- surgery only for minor aesthetic improvement, suggest- ing no need for concern. This study also found no post- operative complications such as saddle nose or deformity of the nasal tip in all patients, although the follow-up period was not long.
Even in case of complications, the degree was very minor. More recently, attempts are being made to apply the technique through an open approach, which can be recommended to patients for whom it would be hard to be correct with the endonasal approach only. But in this study, satisfactory corrections were made in all patients
with the endonasal approach only. Patients who have severe nasal obstruction or have external nose deformity caused by deviation of the upper vault and are not likely to have satisfactory results with traditional methods are recommended.12) Total septal cartilage reconstruction is more invasive compared to existing methods but is co- nsidered to be effective in functional improvement and aesthetic satisfaction in cases having nasal obstruction and scoliotic nose at the same time due to severe devia- tion of the nasal dorsum and the caudal end of the nasal septum.
CONCLUSION
Corrections of severe nasal septal deviation, especially deviation of the L-shaped strut, have been a big challe- nge to surgeons. The existing methods based on cross- hatching or spreader graft were not sufficient in obtaining satisfactory correction. Total septal cartilage reconstru- ction which takes deviated total nasal septum out of the nasal cavity, makes the correction, and then places it into the original site can enhance subjective and objective sa- tisfaction of patients with nasal septal deviation in co- mbination with severe nasal dorsum deviation which have been difficult to treat with traditional techniques. It is also considered to be a safe technique, which causes less co- mplication when the surgeons accustom themselves with the technique sufficiently.
REFERENCES
1) Bernstein L. Submucous operations on the nasal septum. Otolary- ngol Clin North Am 1973;6:675.
2) Stucker FJ. Management of the scoliotic nose. Laryngoscope 1982;
92:128-34.
3) Wright WK. Lateral osteotomy in rhinoplasty. Arch Otolaryngol 1963;78:680-5.
4) TerKonda RP, Jonathan MS. Repairing the twisted nose. Otolary- ngol Clin North Am 1999;32:53-64.
5) Kemker B, Liu X, Gungor A, Moinuddin R, Corey JP. Effect of nasal surgery on the nasal cavity as determined by acoustic rhin- ometry. Otolaryngol Head Neck Surg 1999;121:567-71.
6) Hinderer KH. Fundamentals of anatomy and surgery of the nose.
Birmingham, Ala, Aesculapius Publishing;1971.
7) Gunter JP, Rohrich RJ. Management of the deviated nose. The im- portance of septal reconstruction. Clin Plast Surg 1988;15:43-55.
8) Becker OJ. Problems of the septum in rhinoplastic surgery. Arch Otolaryngol 1951;53:622.
9) Smith F. Plastic and reconstructive surgery. Philadephia: Saunders;
1950.
10) Peer LA. Plastic surgery of the nose. J Med Soc N J 1933;30:123.
11) Maliniac JW. Role of the septum in rhinoplasty. Arch Otolaryngol
1948;48:189.
12) Rees TD. Surgical correction of the severely deviated nose by ext- ramucosal excision of the osseocartilaginous septum and replace- ment as a free graft. Plast Reconstr Surg 1986;78:320-30.
13) Jost G, Legent F. Atlas de Chirurgie Esthetique Plastique. Paris:
Masson & Cie;1975. p.30-46.
14) Denecke HJ, Meyer R. Plastic surgery of head and neck. Vol 1:
corrective and reconstructive rhinoplasty. New York: Springer-Ve- rlag;1967. p.121.