- 66 -
KISEP Case Reports J Rhinol 9(1,2 ), 2002
A Case of Endoscopic Surgical Treatment of the Middle Turbinate Headache Syndrome
Seok-Chan Hong, M.D., Chol Chang, M.D., Beom-Seung Kang, M.D. and Song-Won Lee, M.D.
ABSTRACT
Middle turbinate headache syndrome is rare, and the true incidence of headache from this cause is unknown. Pneumatization or hypertrophy of the middle turbinate can result in its contact with the septum or the lateral nasal wall and may give rise to headache in the periorbital region. It may occur in the absence of inflammatory sinus disease. Clinical history, nasal endoscopic examination, and coronal CT -scan should point to the diagnosis. Treatment is achieved by relieving the contact point by medical or surgical means. The authors experienced a case of middle turbinate headache syndrome, therefore we report this case with a review of literature.
KEY WORDS:Middle turbinate・Headache・Endoscopic surgical treatment.
INTRODUCTION
Middle turbinate headache syndrome is rare and its incidence is not well known. Pneumatization or hyper- trophy of the middle turbinate can result in its contact with the septum or the lateral nasal wall and may give rise to headache in the periorbital and frontal region.
Inflammatory findings of the paranasal sinus were not observed and it can be diagnosed through clinical sym- ptoms, anterior rhinoscopy or paranasal sinus compu- terized tomography.1) For treatment, medical or surgical treatment is used.2) We treated a 65 year old female with middle turbinate headache syndrome through en- doscopic surgery and report this along with docum- entary investigation.
CASE STUDY
A 65 year old female visited our outpatient depart-
ment with bilateral headache of the preorbital region that onset a year ago. The pain was intermittent and could last for several hours at times and was lessened by lying down. Nasal obstruction was accompanied and it showed a temporary reaction to analgesics.
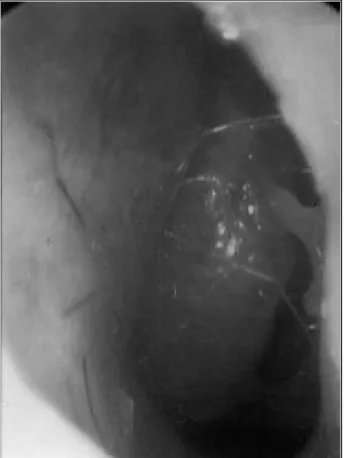
Middle turbinate hypertrophy that was in contact with the nasal septum was observed on nasal endoscopy (Fig. 1, 2). From the view point of paranasal sinus computerized tomography, both paranasal sinuses showed normal appearances with no inflammatory findings. However, a hypertrophied middle turbinate in contact with the nasal septum was observed (Fig. 3).
Under general anesthesia, a bilateral middle tubinop- lasty was executed using nasal endoscopy to maintain the inner mucosa of both middle tubinates. The patient was discharged two days after surgery. The patient was followed up for 2 months after discharge and we ob- served that reoccurring headaches have been com- pletely cured and reoccurring findings and compli- cations such as crust formation, infection and atrophic rhinitis did not occur.
DISCUSSION
Nasal headache takes up less than 10% of all head- aches and is considered an extremely uncomfortable Department of Otorhinolaryngology, College of Medicine, Po-
chon Cha University, Sungnam, Korea
Address correspondences and reprint requests to Seok-Chan Hong, M.D., Department of Otorhinolaryngology, College of Medicine, Pochon Cha University, 351, Sungnam 463-070, Korea Tel:82-31-780-5348, Fax:82-31-780-5347
E-mail:[email protected]
Accepted for publication on August 6, 2002
Hong et al:Middle Turbinate Headache Syndrome / 67
symptom to nasal patients.3) When headache is accom- panied in patients with nasal obstruction and rhinorrhea, a careful history and physical examination is necessary to determine whether or not a paranasal disorder may be the cause of such symptoms. Also, in addition to vascular headaches such as migraines and cluster head-
aches, which are the most common headaches, tension headaches, neuralgias, temporomandibular joint dis- order, ophthalmic headache and so forth must also be distinguished.4) Headaches originated from the tur- binate and paranasal sinus can cause referred pain through the 1st and 2nd branch of the trigeminal nerve.
The 1st branch of the trigeminal nerve is distributed to the frontal region, inner and outer canthus and lateral side of the nose skin and when the anterior side of the middle turbinate is stimulated, referred pain is induced in the frontal region, medial and lateral side of the eye and lateral side of the nose.6) The 2nd branch of the trigeminal nerve is distributed to the skin of the buccal and temporal area and when the posterior side of the middle turbinate is stimulated, patients complain of pain of the buccal and temporal area. Contact headache can be one example. When the hypertrophied middle turbinate is in contact with the nasal septum and nasal sinus wall the sensory division of the trigeminal nerve is stimulated which can cause headache with no spe- cific inflammatory findings of the paranasal or nasal sinus. Wolff7) was the first to report this where he stated that stimulation of the mucosa, where the sensory branches of the trigeminal nerve of the nasal sinus are distributed, induces pain. Becker8) reported that stimu- lation of the anterior middle turbinate and nasal septum where the anterior ethmoidal nerve is distributed may induce referred pain of the inner canthus and orbital area. Greenfield9) stated that that nasal mucosal branch and the afferent fiber of the skin sensory branch of the
Fig. 2. Nasal endoscopy reveals the contact between the left middle turbinate and the nasal septum.
Fig. 1. Nasal endoscopy reveals the hypertrophic change in the anterior end of the right middle turbinate obstructing the mi- ddle meatus.
Fig. 3. Coronal section of computerized tomography reveals the contact points between the hypertrophied middle tur- binate and the septum bilaterally.
68 / J Rhinol 9(1,2), 2002
trigeminal nerve all reach the same area of the cerebral cortex. Stammberger and Wolff6) reported that stimu- lation of the nasal mucosa secretes substance P, a neur- oprotein, and that this substance contributes in vaso- dilatation, hypersecretion and pain transmission mech- anism. Morgenstein and Krieger10) reported a typical middle turbinate headache syndrome irrelevant with inflammatory findings of the paranasal sinus and Blau- grund11) and Goldsmith et al.,12) reported an affiliation of this matter with pneumatization or hypertrophy of the middle turbinate. Patients complain of pain in the orbit region, medial canthus or temporozygomatic re- gion and symptoms may vary according to the nasal cycle and presence of swelling. Pain may subside by pressure while the patient stands or when the affected area is pushed down.1) The presence of contact of a hypertrophied middle turbinate with the nasal septum or lateral wall of the nasal cavity can be distinguished by an anterior rhinoscopy or nasal endoscopy and the presence of mucosal hypertrophy and pneumatization can be distinguished through a paranasal sinus com- puterized tomography. Clerico13) and Chow14) stated that relief of pain by local injection or spray of lido- caine in the contacted area can confirm the diagnosis.
Dissimilarly from other headaches, when there is no reaction to ergotamine or vasoconstrictors and where sympathomimetics and antihistamines that reduce mu- cosal edema or topical steroids are more effective and medication is not, a surgical approach for reduction of the contact area through partial middle turbinoplasty or middle turbinectomy is available or if necessary a septoplasty of the nasal septum may be accompanied.
Morgenstein and Krieger10) successfully treated 17 out of 19 patients surgically and complications such as crust formation, atrophic rhinitis, infection and nasal dryness did not occur.
Chow14) reported an 82% success rate in treating pa- tients with contact headache through nasal endoscopic surgery and Parsons and Batra15) reported a 91% su- ccess rate in treating 19 adults and 15 children by nasal
endoscopic surgery.
CONCLUSION
An accurate diagnosis of contact headac he of the paranasal sinus is necessary through clinical symptoms, nasal endoscopy and paranasal sinus computerized to- mography and it is evaluated that medical and surgical treatment can both successfully treat it.
REFERENCES
1) Anselmo-Lima WT, de Olivera JA, Speciali JG, Bordini C, dos Santos AC, Rocha KV, Pereira ES. Middle turbinate headache syndrome. Headache 1997 Feb;37:102-6.
2) Ramadan HH. Nonsurgical versus endoscopic sinonasal surgery for rhinogenic headache. Am J Rhinol 1999 Nov-Dec;13(6):455-7.
3) Zilkha KJ. Headaches and facial pain. In: Scott B, Walter G, eds.
Scott Brown’s Otolaryngology. 5th ed. Butterworth 1987;4:341-7.
4) Chow JM. Evaluation of rhinologic headaches. In: Stankiewicz JA.
Advanced endoscopic sinus surgery. St. Louis: Mosby;1991. p.121-6.
5) Wolf G, Saria A, Gamse R. New aspects of the autonomic innervation of human nasal mucosa. Laryngol Rhinol Otol 1987;66:149-51.
6) Stammberger H, Wolf G. Headaches and sinus disease: the endo- scopic approach. Ann Otol Rhinol Laryngol Suppl 1988;97(suppl 134):3-23.
7) Wolff HG. The nasal, paranasal, and aural structures as sources of headache and other pain. In: Wolff HG, Headache and other pain.
New York: Oxford University Press;1948. p.532-60.
8) Becker SP. Anatomy for endoscopic sinus surgery. Otolaryngol Clin North Am 1989;22:677-82.
9) Greenfield HG. Headache and facial pain associated with nasal and sinus disorders: a diagnostic and therapeutic challenge. Insights Otolarygol 1990;5:1-4.
10) Morgenstein KM, Krieger MK. Experiences in middle turbinectomy.
Laryngoscope. 1980 Oct ;90(10 Pt 1):1596-603.
11) Blaugrund SM. The nasal septum and concha bullosa. Otolaryngol Clin North Am 1989;22:291-306.
12) Goldsmith AJ, Zahts GD, Stegnjajic A, Shikowitz M. Middle tur- binate headache syndrome. Am J Rhinol 1993;7:17-30.
13) Clerico DM. Sinus headaches reconsidered: referred cephalgia of rhinologic origin masquerading as refractory primary headaches.
Headache 1995 Apr;35(4):185-92.
14) Chow JM. Rhinologic Headaches. Otolalyngol Head Neck Surg 1994;
111:211-8.
15) Parsons DS, Batra PS. Functional endoscopic sinus surgical out- comes for contact point headaches. Laryngoscope 1998 May;108 (5):696-702.