- 69 -
Transseptal-Transsphenoidal Approach: : : : Objective Assessment of Postoperative Nasal Functions
Weon-Jin Seong, M.D.
1, Chae-Seo Rhee, M.D.
1, Jeong-Hun Hah, M.D.
1Chul Hee Lee, M.D.
1, Yang-Gi Min, M.D.
1and Hee Won Jung, M.D.
2 ABSTRACTThe aim of study:The transseptal-transsphenoidal approach (TSA) for pituitary tumors may alter nasal functions, including nasal respiration and olfaction. The aim of this study was to investigate the efficacy of TSA in terms of nasal functions. Materials and Methods:Twenty two cases of pituitary tumors, managed at Seoul National University Hospital from May 1997 through March 1998, were included in this prospective study. Nasal functions were evaluated preoperatively and 2 months after the op- eration through symptom questionnaires, rhinomanometry, acoustic rhinometry and the butanol thres-hold test. Results:The subjective nasal symptoms, including nasal obstruction and olfaction, were not changed following the operation in 72% and 86% of the cases, respectively. In the objective findings, total nasal resistance was not grossly changed after the operation, ho- wever, cross-sectional areas at C-notch and 3.3 cm from the anterior nasal spine increased significantly after the operation. Mu- cosal response to a topical vasoconstrictor after the operation was less effective than before the preoperation. Conclusion:TSA for pituitary tumors may be a safe and effective technique in preserving nasal functions subjectively and objectively.
KEY WORDS:Transseptal-transsphenoidal approach (TSA)·Nasal function.
INTRODUCTION
Among operational approaches to the pituitary gland and its neighboring structures, the transseptal-transsp- henoidal approach (TSA), when compared to the tran- sfrontal approach, is faster in accessing the pituitary gland and allows a complete extracapsular enucleation through a direct extended view using a microscope. In addition, it causes less postoperative scarring and pain,1-4) making it the most popular method these days.
When the pituitary gland is operated on with TSA, the septal cartilage is inevitably pushed out to a nasal cavity, and parts of the perpendicular plate of the ethmoid, the vomer, and the anterior wall of the sphenoid sinus are removed, which may damage nasal function. But, patients
who have had the transsphenoidal approach have been cured of their endocrinologic problems and neurologic problems caused by lesions of the pituitary gland and skull base area rather than for their postoperative nasal function changes or rhinologic symptoms. Several stu- dies on subjective postoperative symptoms and rhinol- ogic complications have reported few cases where big rhinologic changes were caused by the transsphenoidal approach.5)6) But only a few studies have been made on objective changes of nasal function as well as subjective symptom changes after TSA.
Objective analyses were made in this study based on rhinomanometry, acoustic rhinometry and the butanol threshold test, in addition to subjective symptom chan- ges in order to find out how TSA influences on nasal function.
MATERIALS AND METHODS
We conducted a prospective study on 22 out of 54 pa- tients who had the TSA on pituitary tumors from May 1997 to March 1998 at Seoul National University Ho- spital. Patients who had growth hormone abnormality, endocrinologic disorders, such as Cushing disease, intr-
1Departments of Otorhinolaryngology-Head and Neck Surgery,
2Neurosurgery, Seoul National University College of Medicine, Seoul, Korea
Address correspondence and reprint requests to Chae-Seo Rhee, M.D., Department of Otorhinolaryngology-Head and Neck Su- rgery, Seoul National University Hospital, 28 Yongon-dong, Ch- ongno-gu, Seoul 110-744, Korea
Tel:82-2-760-3991, Fax:82-2-745-2387 E-mail:[email protected]
Accepted for publication on March 10, 2000
anasal operations in the past, the common cold or upper respiratory tract diseases at the time of testing, or a his- tory of allergic rhinitis and smoking were excluded from the study group.
In this study there were 13 males and 9 females with an average age of 43 years, ranging from 21 to 75 years of age. Of the 22, 12 cases were operated on with the columella flap technique and 10 cases had the external rhinoplasty approach. There was no specific criteria for the particular approach which was just decided based on the operators’ preference.
Before and two months after the operation, question- naires on subjective symptoms such as nasal breathing and olfaction were drawn up while rhinomanometry, ac- oustic rhinometry, and the butanol threshold test were conducted prospectively for objective tests.
Through a physical examination, abnormal findings were checked before and two months after the operation.
The questionnaire on subjective symptoms, the visual analogue scale (VAS)7) was used, in which the patients made marks on a 10 cm stick directly for their nasal br- eathing (nasal obstruction) and olfaction. When they felt no symptom they marked 0 and when they felt a severe symptom they marked 10. It was considered to be a change of symptom when the location of the mark on the visual analogue scale differed by more than than 1 cm.
For the rhinomanometry, the Rhinotest MP500 (Bre- hm+Jung elektronik GmbH, Darmstadt, Germany) was used in the active anterior rhinomanometry method.8)9) The average value was obtained by measuring all pat- ients three times on the same morning with the mask method while the patients were placed in a seat. The na- sal resistance was measured before contraction of nasal mucosa and measured again 15 minutes after contraction of mucosa with 0.1% pseudoephedrine, in order to make the comparison. While the reference point of nasal resi- stance was set at 150 Pa and 75 Pa which are known to be normal respiration pressure,10) the total nasal resista- nce of both nasal cavities was calculated. The total nasal resistance was computed based on the formula, RT=RR
×RL/(RR+RL) (RT, total nasal resistance;RR, right- side nasal resistance;RL, left-side resistance) using ri- ght and left side nasal resistance.7)
For the acoustic rhinometry, the Eccovision Acoustic Rhinometry System (E. Benson Hood Laboratories, Inc., Pembroke, MA) was used in a seated position. A nose
piece, the same size as the anterior nares, was inserted carefully so as not to distort the nasal vestibule and me- asurements were made three times both before and after contraction of nasal mucosa for obtaining the average value. The cross-sectional area was measured by using the area-distance curve at a location 3.3 cm distant from the C-notch and nares.11) The volume of the nasal cavity was computed from the anterior nasal spine to a location 6.0 cm distant from it.
The butanol threshold test was employed for the olf- actory evaluation.12)13) Beginning with the lowest-degree butanol concentration, the patient was given a bottle of specific concentration of butanol and another bottle of non-butanol and asked which bottle smelled stronger. The shape and color of each bottle was identical and the test was repeated four times for each butanol concentration.
The threshold score was recorded by adding 1 to the lo- west diluted stage which the patient could differentiate.
When the patient didn’t react to any concentration of butanol, the threshold score was 0.
For analysis of subjective symptoms, the Wilcoxon si- gned rank test was used while for objective symptoms, the paired t-test was used.
RESULT
Postoperative subjective nasal symptoms
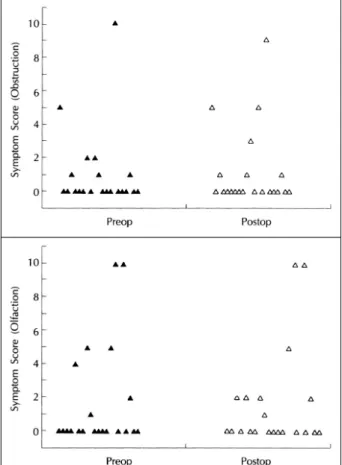
For 16 (72.8%) out of 22 cases, there was no post- operative change in nasal breathing compared to preop- erative symptoms, while improvement and deterioration showed in three cases (13.6%), respectively. Olfactory function showed no change in 19 cases (86.4%), impr- ovement in two cases (9.1%), and deterioration in one case (4.5%), though a complete loss of olfaction did not occur (Fig. 1).
Objective assessment of postoperative nasal functions
The change of total nasal resistance which was com- puted through rhinomanometry before and after the op- eration showed no statistical significance at 150Pa and 75Pa, and before and after the nasal mucosa contraction.
The nasal resistance before and after the contraction was compared to check the reaction of nasal mucosa to the topical vasoconstrictor. In the pre- and postoperative ch-
ange of total nasal resistance, the nasal resistance dif- ference before and after the nasal mucosa contraction showed a significant decrease at 150 Pa after the ope- ration (Table 1).
In the acoustic rhinometry, the cross sectional area of the nasal cavity showed significant postoperative incre- ase at locations of the C-notch and 3.3 cm distant from the nares before the contraction. After the contraction, however, there was no statistical significance though the cross sectional area of the nasal cavity showed an inc- rease (Table 2). The nasal cavity volume also increased significantly after the operation (Table 3). The difference of cross sectional area before and after the vasoconst- riction was compared before and after the operation to check the reaction of the nasal mucosa to the topical
vasoconstrictor. In all locations measured, the increase of the cross sectional area caused by the vasoconstrictor showed a significant decrease after the operation (p<0.
05). The change of the nasal cavity volume before and after the nasal mucosa contraction also showed the same result (p<0.05).
In the butanol threshold test, the average threshold sc- ore was 7.4±3.7 and 7.6±3.3 before and after the op- eration, showing no significant difference.
Postoperative physical examination findings
Five patients showed a severe case of nasal septum deviation before the operation which were all corrected after the operation. Preoperative abnormal findings in the nasal cavity were not reported. Any septal perforation or excessive crust formation were reported through anterior rhinoscopic examination and endoscopic examination of the nasal cavity conducted two months after the opera- tion. But synechia of the nasal septum and turbinate was observed in five cases.
DISCUSSION
In most cases, postoperative change of nasal breathing and olfaction is not reported in patients’ subjective sy- mptoms, but in this study three cases (13.6%) experie- nced deterioration of nasal breathing and one case (4.
5%) also showed deteriorated olfactory function, showing similar findings to other study results.5)6)14) In the case of nasal breathing, Lee et al.,14) reported a decrease of nasal breathing in 7.4% of patients after the TSA and improvement of nasal breathing in 20%. Gammert5) and Sherwen et al.,6) reported a decrease of nasal breathing in 7% and improvement of it in 24%. In this study, two out of three cases which showed a decrease of nasal breathing also showed an increase of the total nasal re- sistance and increase of the VAS value from 1,0 to 3,5 respectively, suggesting that nasal breathing can be wo- rsened after the operation in some cases. This is consi- dered to be caused by synechia in nasal cavity. Mean-
Table 1. Total nasal resistance (Pa/cm3/sec) before and after transseptal-transsphenoidal approach
Preop Postop
() BD AD BD-AD BD AD BD-AD
75 Pa 0.22±0.15 0.13±0.07 0.090±0.11 0.19±0.09 0.16±0.08 0.035±0.046 150 Pa 0.31±0.20 0.16±0.11 0.15 ±0.16 0.25±0.15 0.20±0.10 0.051±0.067*
*:Significantly different from preoperative values BD;before decongestion AD;after decongestion Fig. 1. Changes in subjective symptoms after transseptal-trans-
sphenoidal approach.
while, in 13.5% of patients, the nasal breathing showed improvement, which can be explained by the fact that correction of the nasal septum was conducted on patients with nasal septum deviation at the same time.
When considering olfactory function, one case showed a decline of olfactory function subjectively but in the butanol threshold test, it showed a normal range without any difference. But Gammert5) reported a partial decline of olfaction in 12% subjectively and Lee et al.,14) repo- rted the same symptom in 10.7%, which requires patients to be recognized on the subjective partial olfaction loss before the operation.
Compared to subjective symptoms, the total nasal resistance on the objective tests showed no significant changes, but the cross sectional area and volume of the nasal cavity showed a significant increase. The increase of the nasal cavity cross sectional area can be offset by the increased nasal resistance which resulted from narr- ower choanae by adipose tissue inserted into the sphen- oid sinus and the posterior part of the nasal septum at the time of suturing after transseptal pituitary surgery.
Postoperative increase of the cross sectional area and volume of the nasal cavity can be attributed to the si- multaneous correction of nasal septum deviation during the TSA, and outward fracture of the middle turbinate by Hardy nasal speculum during the neurosurgery ope- ration, which widened the common meatus area further.
This can also be related with the fact that the acoustic rhinometry reflects the wide area such as the common meatus better than narrow areas in the nasal cavity such as the middle and superior meatus.15)
Another observation worthy of note is that a consid- erable postoperative decrease of nasal mucosa reaction to the tropical vasoconstrictor was observed in changes
of total nasal resistance and cross sectional area of the nasal cavity. These facts suggest a possibility of contr- action of the nasal mucosa and decrease of reaction after the TSA though there was no change of subjective symptoms. Future changes of contracted nasal mucosa should be further studied over the long term to check wh- ether it is related with the turbinate being pressed for a long time by the Hardy nasal speculum during the TSA or is a temporary phenomenon.
CONCLUSION
TSA for pituitary tumors is a safe operative method in preserving nasal functions before and after the operation subjectively and objectively. In some patients, however, it may cause decline of nasal functions subjectvely, the- refore it is recommended to recognize the patient on the fact before surgery.
REFERENCES
1) Eisele DW, Flint PW, Janas JD, Kelly WA, Weymuller Jr EA, Cummings CW. The sublabial transseptal transsphenoidal approach to sellar and parasellar lesions. Laryngoscope 1988;98: 1301-8.
2) Hardy J. Transsphenoidal Hypophysectomy. J Neurosurg 1971;
34:582-94.
3) Kern EB. Transnasal pituitary surgery. Arch Otolaryngol 1981;107:
183-90.
4) Koltai PJ, Goldstein JC, Parnes SM, Price JC. External rhinoplasty approach to transsphenoidal hypophysectomy. Arch Otolaryngol 1985;111:456-8.
5) Gammert C. Rhinosurgical experience with the transseptal-transs- phenoidal hypophysectomy: Technique and long-term results. La- ryngoscope 1990;100:286-9.
6) Sherwen PJ, Patterson WJ, Griesdale DE. Transseptal, transsph- enoidal surgery: A subjective and objective analysis of results. J Otolaryngol 1986;15:155-60.
7) Kim CS, Moon BK, Jung DH, Min YG. Correlation between nasal obstructuion symptoms and objective parameters of acoustic rhin- ometry and rhinomanometry. Auris Nasus Larynx 1998;25:45-8.
8) Broms P,Jonson B, Lamm CJ. Rhinomanometry Ⅱ. A system for numerical description of nasal airway resistance. Acta Otolaryngol 1982;94:157-68.
9) Gordon ASD, McCaffrey TV, Kern EB, Pallanch JF. Rhinomano- metry for preoperative and postoperative assessment of nasal obs- truction. Otolaryngol Head Neck Surg 1989;101:20-6.
10) Kim CN, Yun JB, Kim CD, Min YG. Rhinomanometric measure- Table 2. The change of cross-sectional area before and after transeseptal-transsphenoidal approach
Preop Postop
BD AD BD-AD BD AD BD-AD
C-notch 1.33±0.40 2.04±0.58 0.65±0.31 1.84±0.53* 2.09±0.56 0.25±0.23*
3.3 cm 1.75±0.53 2.73±0.69 0.98±0.42 2.68±0.86* 3.16±0.94 0.48±0.50
*Significantly different from preoperative values (p<0.05) BD;before decongestion AD;after decongestion
Table 3. The change of nasal cavity volume (cm3) before and after transeseptal-transsphenoidal approach
Before decongestation After decongestation Preop 11.3±3.42 16.3±4.64 Postop 16.4±3.96* 18.4±3.43*
*Significantly different from preoperative values (p<0.05)
ments before and after septoplasty. Korean J Rhinol 1995;2(1):
52-6.
11) Min YG, Jang YJ. Measurements of cross-sectional area of the nasal cavity by acoustic rhinometry and CT scanning. Laryngos- cope 1995;105(7 Pt1):757-9.
12) Cain WS, Gent JF, Goodspeed RB, Leonard G. Evaluation of olf- actory dysfunction in the Connecticut chemosensory clinical res- earch center. Laryngoscope 1988;98:83-8.
13) Min YG, Yun YS, Song BH, Cho YS, Lee KS. Recovery of nasal physiology after functional endoscopic sinus surgery: Olfaction and
mucociliary transport. ORL J Otorhinolaryngol Relat Spec 1995;
57:264-8.
14) Rhee CS, Lee KS, Kim CS, Jung HA, Suh SJ, Moon BK, et al.
Transseptal-transsphenoidal approach: Rhinologic complications according to the types of approach. Korean J Otolaryngol 1996;39 (8):1249-52.
15) Rhee CS, Lee CH, Lee KS, Yun JB, Min YG. Correlation between cross-sectional areas along the nasal cavity measured using acoustic rhinometry and CT scanning in normal subjects. The 3rd Asian Re- search Symposium in Rhinology;1998, Abstract, p.39.