- 154 -
KISEP Case Reports J Rhinol 4((((2)))), 1997
Mucoepidermoid Carcinoma of the Ethmoid Sinus: : : : Report of a Case with Bizarre Manifestations
Jae Yong Lee, M.D., Woo Jung Kim, M.D., Young Ho Kim, M.D., Sang Hoon Shin, M.D., Heung Man Lee, M.D. and Sang Hag Lee, M.D.
ABSTRACT
Mucoepidermoid carcinoma is a common malignant tumor of the major salivary glands but it rarely arises in the nasal cavity and paranasal sinuses. Like other paranasal sinus carcinomas, mucoepidermoid carcinoma of the ethmoid sinus may first be no- ticed by the extension of tumor mass to adjacent structures such as nasal cavity, orbit, other paranasal sinuses, and anterior skull base. We recently encountered a patient with complaints of right conjunctival edema and drowsy mentality who was initially treated under the impression of the maxillary, ethmoid and sphenoid sinusitis with cavernous sinus thrombosis. The patient underwent sinus surgery for control of ethmoid and sphenoid infection that was refractory to antibiotic treatment. During the operation, there was only inflammatory mucosal thickening without any specific mass lesion. But, the final diagnosis was mu- coepidermoid carcinoma of intermediate grade.
KEY WORDS:Mucoepidermoid carcinoma·Ethmoid sinus.
INTRODUCTION
Ethmoid sinus lesions represent a small percentage of all malignancies;paranasal sinus tumors are 3% of upper aero- digestive tract cancers and ethmoid sinus carcinomas are 5% to 25% of all sinus malignancies.1) Because of their proximity to the skull base, central nervous system, and orbit, these lesions may cause considerable complications involving those areas.
Thus, it is generally believed that the signs and symptoms of ethmoid and sphenoid sinus carcinomas depend on the spread of tumor to adjacent structures, and many reported cases com- posed largely of mass lesions occupying the nasal cavity.
We recently encountered a case of mucoepidermoid carci- noma with bizzare manifestations that occurred in the ethmoid and sphenoid sinus. A case report and review of literatures are presented.
CASE REPORT
A 72-year-old woman with a history of drowsy mentality
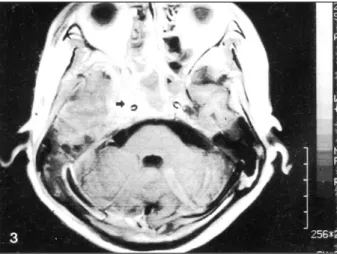
and mild eyelid/conjunctival swelling on the right side had been refered from another hospital. Initially, she was managed at the hospital for right facial weakness and headache for a few months. Physical examination revealed right periorbital and cheek swelling with reddish discolored skin and tender- ness over the cheek. She had a limited ocular motility on right side. Plain radiographic findings of paranasal sinus showed right maxillary and ethmoid sinus opacification. She was tre- ated with antibiotics under the impression of acute sinusitis with complications. But, her symptoms were not improved. In November 13, 1996, she was transfered to our hospital for further evaluation and treatment. When first seen at our hos- pital, her mentality was drowsy and there was mild conjunctival edema, but facial swelling and fever was absent. Endoscopic examination of the nasal cavity did not reveal any significant inflammatory or mass lesion in the nasal cavity. Computed to- mography revealed mucosal thickening in right maxil-lary and ethmoid sinuses, and soft tissue density in both sphenoid sin- uses without erosion of the fovea ethmoidalis and cribriform plate (Fig. 1). Paranasal sinus magnetic resonance imaging showed enhanced high signal intensity of right posterior eth- moid sinus mucosa (Fig. 2). Brain magnetic resonance imaging showed abnormal increased signal intensity lesion in right ca- vernous sinus (Fig. 3), and slight compression of right lateral ventricle was noted. These findings suggested chronic infla- mmatory maxilloethmoid and sphenoid sinusitis associated with intracranial complications or cavernous sinus thrombosis. Tr- eatment with intravenous antibiotics was initiated, and cont- Department of Otolaryngology-Head and Neck Surgery, Col-
lege of Medicine, Korea University, Seoul, Korea
Address correspondense and reprint requests to Sang Hag Lee, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Korea University, 126-1, 5 Ka, Anam-Dong, Sungbuk-Ku, Seoul 136-705, Korea
Tel:82-2-920-5486, 5761, Fax:92-2-925-5233 Accepted for publication on October 14, 1997
Lee et al:Mucoepidermoid Carcinoma of Ethmoid Sinus / 155
inued over several days. However, it failed to improve her symptoms, and mentality worsened.
We decided to explore and remove ethmoid and sphenoid
sinus lesion, and an unilateral endoscopic ethmos-phenoidectomy was performed. All sinuses were found to have only thickened mucosa without mucopurulent secretions. During the operation, no specific mass-like lesion was observed. On histopathologic
Fig. 3. Axial section of brain magnetic resonance imaging sho- wing abnormal increased signal intensity lesion in right caver- nous sinus (arrow) suggesting cavernous sinus thrombosis.
Fig. 2. Coronal section of paranasal sinus magnetic resonance imaging showing an enhanced lesion of posterior ethmoid sinus and thickening of right maxillary sinus mucosa.
Fig. 1. Coronal section of paranasal sinus computed tomogra- phy showing mucosal thickening in maxillary sinus and ethmoid sinus without bony erosion.
Fig. 6. Axial section of brain computed tomography taken on the fifth postoperative day showing generalized brain edema, especially severe in the right temporal lobe, and severe com- pression of ventricles.
Fig. 5. Alcian blue stain showing mucinous material stained as blue color in mucous glands (100).
Fig. 4. Intermediate and squamous tumor cells and glands lined with mucous cell (H & E stain, 200).
156 / J Rhinol 4(2), 1997
examinations, it was revealed as an intermediate grade muco- epidermoid carcinoma. Permanent microscopic sections showed irregular submucosal solid nests that mainly composed of in- termediate cells and squamous cells (Fig. 4), and these cells formed tumor cell nests in vascular lumen. Intracellular mucin was observed in many cells lining the glandular lumen (Fig.
5). On follow up brain computed tomography taken on the fifth postoperative day, brain edema was aggravated especially in the right temporal lobe, and the ventricles on both sides were severely compressed due to the brain edema (Fig. 6). Despite of aggressive medical therapy, she expired at one week after surgery.
DISCUSSION
Tumors arising from mucosa of the nasal cavity and par- anasal sinuses represent less than 1% of all malignancies. Sq- uamous cell carcinoma comprises 80-90% of these tumors with 4-8% being of salivary gland origin. The latter group includes adenoid cystic carcinoma, adenocarcinoma, pleomo- rphic carcinoma, and mucoepidermoid carcinoma in descen- ding order of incidence. Mucoepidermoid carcinoma is very rarely found in the nasal cavity and paranasal sinuses although it is the most common cancer in major salivary glands.2)
The etiologic factors responsible for the development of mucoepidermoid carcinoma remain obscure. However, minor trauma and chronic irritation have been implicated as etiolo- gies. Chronic wood dust exposure poses a high risk for ethmoid sinus carcinoma, trapping of particles in the anterior ethmoid air cells during normal nasal respiration and decreased ciliary motility may be responsible for this association.3-6) Spiro et al.7) reported a case of mucoepidermoid carcinoma in a 7- year-old girl which was developed 2 years after the impaction of a button in her nose. Heenan and Schaefer reviewed the literature on the Canadian eskimo population, who has a very high incidence of salivary gland tumors, up to 30 times than the white Saskatchewan population.8) Bridger et al. suggested that paranasal sinus carcinoma is related to chronic anemia and radiation exposure, especially, radium has been repeatedly im- plicated as a cause for mucoepidermoid carcinoma.9)
Clinically, the symptoms and signs of mucoepidermoid ca- rcinoma of ethmoid sinus depend on the spread of tumor to adjacent structures. These include facial pain, nasal obstruction, epistaxis, facial weakness, headache, visual discomfort, etc. The common findings of ethmoid sinus mucoepidermoid carcinoma are unilateral nasal obstruction, intranasal mass, and purulent hemorrhagic discharge. Less common signs include proptosis, diplopia, broadening of the nasal dorsum, and anosmia.1-6) St- udies on the biological behaviors of ethmoid sinus carcinoma showed that the most common pathway of tumor spread is
through the middle meatus to involve the nasal cavity and the nasal septum. Direct extension to the contralateral ethmoid sinus is also frequently observed. Superior extension into the skull base at the cribriform plate, fovea ethmoidalis, and fro- ntal sinus is frequent, and lateral extension into orbital apex is also possible.1) These extension is associated with tumor erosion through bony wall. Assessment of ethmoid sinus car- cinoma is successfully achieved by endoscopic and radiologic examinations, providing important information on deciding the treatment of these lesions. That is, nasal endoscopic examin- ation and biopsy is needed for confirmation of ethmoid sinus carcinoma. Computed tomography documents the expansile nature of paranasal sinus carcinoma with erosion of bony sinus wall, and magnetic resonance imaging delineates the invo- lvement of adjacent soft tissue structures. However, in the present case no tumor mass was found by these diagnostic procedures.
These minor salivary gland tumors have been previously observed to have a strong tendency to cause bone remodeling rather than aggressive bone destruction.10) The lesion of our case was limited to ethmoid sinus mucosa with little, if any, marginal bone destruction. Interestingly it was difficult to de- fine tumor mass in the surgical field of the ethmoid sinus.
Preoperative brain magnetic resonance imaging showed incr- eased signal intensity lesion in right cavernous sinus suggesting the cavernous sinus thrombosis of inflammatory origin. But, there was no fever in this case which is one of the most com- mon signs of cavernous sinus thrombosis, and permanet hist- opathologic finding revealed mucoepidermoid carcinoma with tumor cell nests in vascular lumen. Thus, it is possible to assume that worsened mentality in this patient may be due to the can- cer invasion to the cavernous sinus resulted in obstruction of venous drainage and brain edema. However, the definite etio- logic factors responsible for comatose mentality and death in this case still remain obscure.
REFERENCES
1) Rice DH. Benign and malignant tumors of the ethmoid sinus. Ot- olaryngol Clin North Am 1985;18:113-24.
2) Batsakis JG. Tumors of the head and neck: clinical and pathologi- cal considerations. 2nd ed. Baltimore: Williams and Wilkins 1979;
79-99.
3) Kraus DH, Sterman BM, Levine HL, Wood BG. Factor influencing survival in ethmoid sinus cancer. Arch Otolaryngol Head Neck Surg 1992;118:367-72.
4) Hadfield EH, Macbeth RG. Adenocarcinoma of ethmoids in fu- rniture workers. Ann Otolaryngol 1971;80:699-703.
5) Shklar G. Recent advances in experimental oral and salivary gland tumors. J Oral Surg 1970;28:495-500.
6) Klintenberg C, Olofsson J, Hellquist H, Sokjer HJ. Adenocar-cin- oma of the ethmoid sinuses: a review of 28 cases with special ref-
Lee et al:Mucoepidermoid Carcinoma of Ethmoid Sinus / 157
erence to wood dust exposure. Cancer 1984;54:482-8.
7) Spiro RH, Huvos AG, Berk R, Strong EW. Mucoepidermoid car- cinoma of salivary gland origin. Am J Surg 1978;136:461-8.
8) Heenan H, Schaefer DJ. Malignant tumors of the salivary glands.
J Otolaryngol 1977;6:374-80.
9) Bridger MWM, Beale FA, Bryce DP. Carcinoma of the paranasal sinuses-a review of 158 cases. J Otolaryngol 1978;7:379-88.
10) Som PM. The paranasal sinuses. Head and neck imaging excluding the brain. St Louis: CV Mosby 1984;1-142.