online©ML Comm
-
158
-J Rhinol 16(2), 2009 www.ksrhino.or.kr
원발성 접형동 후각신경아세포종 1예
부산대학교 의학전문대학원 부산대학교병원 이비인후과,1 양산부산대학교병원 이비인후과2
조규섭1·이현민1·최성원1·노환중2
A Case of Primary Olfactory Neuroblastoma of the Sphenoid Sinus
Kyu-Sup Cho, MD1, Hyun-Min Lee, MD1, Sung-Won Choi, MD1 and Hwan-Jung Roh, MD2
1
Department of Otorhinolaryngology-Head and Neck Surgery, Pusan National University Hospital, Busan
;and
2
Department of Otorhinolaryngology-Head and Neck Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea
ABSTRACT
Olfactory neuroblastoma is a rare malignant tumor of the nasal cavity arising from the olfactory neuroepithelium. It usually pres- ent as a polypoid mass in the superior nasal cavity including the cribriform plate, superior turbinate, and superior portion of nasal septum. The development of olfactory neuroblastoma outside of the region, in which olfactory epithelium exists, is exceedingly rare. In this report, we present an interesting case of an isolated sphenoid sinus olfactory neuroblastoma with a brief review of the literature.
KEY WORDS
: Olfactory neuroblastoma·Sphenoid sinus.
서 론
후각신경아세포종은 미분화된 신경 외배엽에서 기원하는 드 문 악성 종양으로 비강과 부비동에서 생기는 종양의 3~5%를 차지한다.1) 후각상피 점막의 기저세포에서 기원하므로, 비강 내 사골동 천정이나 비중격 등에서 주로 발생하여 주위 부비 동, 안와 및 두개 내로 침범하며 림프절 및 원격 전이를 잘하 는 것으로 알려져 있다.2) 후각상피가 존재하지 않는 부위에서 후각신경아세포종의 발생은 극히 드물어 접형동에서 원발한 예는 세계적으로도 단지 수례만이 보고되었으며,3-6) 국내에서 는 2007년에 1예가 보고되었다.7) 이에 저자들은 접형동에서 원발한 후각신경아세포종을 성공적으로 치험하였기에 문헌 고 찰과 함께 보고하는 바이다.
증 례
66세 남자 환자가 이비인후과 의원에서 촬영한 부비동전
산화단층촬영에서 우측 상악동의 완전 혼탁과 접형동 주위에 골 파괴를 동반하는 병변이 관찰되었으나, 우측 상악동에 대한 내시경 부비동수술만 받은 후 접형동의 병변은 진균구(fungal ball) 의심 하에 본원으로 전원되었다. 내원 당시 환자는 특별 한 접형동과 연관된 증상을 호소하지 않았으며, 비강 내시경 소견에서 우측 중비도 상악동 개방술 후 상태를 보이는 것 외 에는 특이 이상소견을 보이지 않았다.
본원에서 촬영한 부비동전산화단층촬영에서 이전 수술로 상 악동이 중비도로 확장되어 개구되어 있었고, 접형동을 가득 채 우고 있는 연부조직 음영은 여전히 관찰되었으며 접형동 주위 골을 침식시키고 경사대(clivus)도 파괴된 소견이 관찰되었다 (Fig. 1). 부비동 자기공명영상촬영에서 접형동 내에 T1 영상 에서 저신호, T2 영상에서 고신호 강도를 보이는 낭종성 병변 을 포함한 종양이 관찰되었다. 종양은 T1, T2 영상에서 저신 호, gadolinium으로 조영한 영상에서 조영증가가 잘 되는 양 상을 보였으며 양측 내경동맥을 둘러싸고 해면 정맥동으로 침 범되어 있었다(Fig. 2).
전신마취 하에 경비강 접형동 개방술을 시행하였다. 양측 중 비갑개와 상비갑개의 하부 1/3을 절제하여 공간을 확보한 후 양 측 접형동의 자연 개구부를 중심으로 접형동을 넓게 개방하니 접형동은 종양으로 둘려싸여 있었다. 종양의 전벽에서 시행한 동결절편검사결과 원형 소세포 종양(small round cell tumor) 본 연구는 2008년도 부산대학교병원 임상연구비 지원으로 이루어 졌음.
논문접수일:2009년 2월 4일 / 심사완료일:2009년 3월 31일 교신저자:노환중, 626-770 경남 양산시 물금읍 범어리 양산부산대학교병원 이비인후과
전화:(055) 360-1440·전송:(055) 360-2930 E-mail:[email protected]
조규섭 등:원발성 접형동 후각신경아세포증 / 159
으로 나왔으며 종양 내 갈색의 액체가 다량 흘러나왔다. 종양 의 전벽과 후벽사이는 액체로 차 있는 빈 공간이었으며 종양 의 후벽은 뇌경막(dura mater)과 유착되어 박동이 관찰되었 다. 후벽 제거 시 뇌경막 손상의 가능성이 높아 뇌경막과 유착 된 후벽 일부를 제외하고는 모두 종양을 제거하고 수술을 마 쳤다. 술 후 시행한 조직검사결과 혈관은 풍부하였으나 다형 태성(pleomorphism), 세포분열(mitoses), 괴사(necrosis) 및
신경섬유기질(neurofibrillary matrix)은 관찰되지 않았다.
면역조직화학검사에서 CD56과 synaptophysin에 양성 소견을 보이고, cytokeratin, S-100 protein, vimentin, LCA(leu- kocyte common antigen), HMB(human melanin black)-45 에 음성을 보이는 I 등급 후각신경아세포종으로 진단되었다 (Fig. 3).
전신 전이 유무 및 병기 결정을 위해 시행한 컴퓨터양전자단
Fig. 1. Paranasal sinus CT scan shows middle meatal antrostomy state in right maxillary sinus and total haziness in sphe- noid sinus with bone destruction in both sphenoid sinuses. A:Axial view. B:Cor-
onal view. A B
Fig. 2. Pituitary coronal MRI shows a well enhanced mass, which is low signal intensity on T1 and T2 weighted image (WI) in both sphenoid sinus invading into both cavernous sinus with cystic portion, which is low signal intensity in T1WI and high signal intensity in T2WI. A:T2WI, B:TIWI. C: gadolinium-enhanced T1WI.
A B C
Fig. 3. Histopathologic finding of olfactory neuroblastoma. A:The tumor cells show enlarged nuclei and indistinct cytoplasm without pleomorphism and mitoses (H&E stain, ×400). The neurofibrillary element is absent. B, C:Immnohistochemical staining shows the positive reaction in CD50 (B) and synaptophysin (C)(×400).
A B C
160 / J Rhinol 16(2), 2009
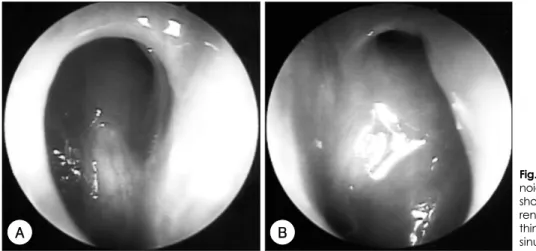
층촬영에서 경부 및 전신 전이 소견은 없었다. 환자는 수술 후 2차례의 항암치료(etoposide, ifosfamide, cisplatin)를 시행하였으나 치료에 전혀 반응을 보이지 않아, 방사선치료 (원발 종양 부위:60 Gy, 고위험부위:54 Gy, 양측 경부 부 위:48 Gy)를 시행하였다. 방사선 치료 종결 후 환자는 특별 한 증상을 호소하고 있지 않으며, 치료 종결 후 3개월에 검사 한 비강 내시경 소견에서 양측 접형동 내에 점막은 비후되어 있었으나 종양은 관찰되지 않았다(Fig. 4).
고 찰
후각신경아세포종은 1924년 Berger에8) 의해 처음 보고된 후각 상피세포로부터 발생하는 드문 비강 내 악성종양으로 후각 상피세포가 정상적으로 존재하지 않는 상악동, 사골동, 뇌하수체 부위에서는 후각신경아세포종의 발생이 보고된 적 이 있으나 접형동에 국한된 경우는 전 세계적으로도 단지 수 례만이 보고되었다.3-6) 이러한 부위에 발생한 원인에 대한 가설은 말초 신경절에서 기원하였을 가능성과 배아 발달기 중의 이소성 잔류세포(ectopic cell rests)로부터 발생하였을 가능성 등을 들 수 있다.6) 비강 내 후각신경아세포종은 모든 연령대에서 발생이 가능하며, 성별에 따른 발생빈도는 차이 가 없는 것으로 알려져 있다. 가장 흔하게 나타나는 증상은 일 측성 비폐색과 비출혈, 비루, 안 증상, 두통, 후각소실로 내 원하지만,2) 접형동에 국한된 경우는 무증상인 경우가 대부분 이며 우연한 부비동 촬영에서 발견하는 경우가 대부분이다.
본 증례도 특별한 증상이 없었지만 개인병원에서 촬영한 부비동전산화단층촬영에서 접형동 주위에 골 파괴를 동반하 는 병변이 관찰되어 본원으로 전원 되었다. 진단은 매우 어려 우나 최근 면역조직화학검사의 발달로 진단율이 좋아지고 있 다. 후각신경아세포종은 일반적으로 neurofilament protein, synaptophysin 및 neuron specific enolase에 강한 양성을
보이며, cytokeratin, TTF-1(thyroid transcription factor), CEA(carcinoembryonic antigen) 등에는 음성을 보인다. 더 욱이 전자 현미경상에 치밀 신경분비과립(dense core neuro- secretory granule), 세관(microtubule), 중간세사(interme- diate filament)를 발견하면 정확한 진단을 가능하게 한다.
전산화단층촬영이나 자기공명영상이 종양의 존재여부 및 침범 부위에 대한 정보를 제공하며 병기와 치료방향 결정에 도움이 된다. 전산화단층촬영에서는 균일한 조영증강을 보이 는 주변의 골 파괴소견이 관찰되며, 자기공영영상에서는 T1 과 T2 영상에서 모두 저음영을 보이지만, T2영상에서 조금 더 밝게 보이며, gadolinium으로 조영 시 조영증가가 잘되는 경향을 보인다.5)
치료는 수술과 방사선 치료가 가장 이상적인 것으로 되어 있 으나, 진행된 병기이거나 수술로 완전 절제가 불가능한 경우 는 항암치료를 할 수 있다. 최근에는 수술로 완전한 제거가 힘든 경우에 내시경수술만으로 종양을 제거하고 술 후 방사 선 치료를 시행하여 좋은 성과를 내기도 하였다.9) 특히 접형 동에만 국한된 후각신경아세포종의 경우에는 접형동 주위의 중요한 구조물로 인해 완전 절제가 불가능한 경우가 많아 주로 항암치료와 방사선치료를 병행하여 치료하고 있다, 그러나 본 증례에서는 내시경수술로 접형동 안의 종양을 최대한 제거하고, 2차례의 항암치료를 시행하였으나 반응이 좋지 않아 방사선 치료를 병용하였다.
비강에 생긴 후각신경아세포종의 예후는 현재까지 Kadish 병기 분류와 Hyams의 조직학상 분류가 중요한 것으로 알려 져 있고,10-12) 임파선의 전이와 나이도 생존률과 관계있다고 보 고되고 있다.12) 본 증례와 같이 접형동에 원발한 경우 그 증례 가 드물어 접형동의 침범여부가 병기 분류에 포함되지 않아 정 확한 Kadish 병기 분류는 할 수 없지만, Hyams 조직 분류에 따라 I 등급으로 분류되었다.10-12) Hyams의 조직 분류에 따라 저도 악성 환자(grade I, II)의 5년 평균 생존률은 56%정도이
Fig. 4. Endoscopic finding of both sphe- noid sinus 3 months after radiotherapy shows no evidence of residual or recur- rent tumor except mucosal edema wi- thin sphenoid sinus. A:Right sphenoid sinus. B:Left sphenoid sinus.
A B
조규섭 등:원발성 접형동 후각신경아세포증 / 161
고 고도 악성 환자(grade III, IV)일 경우에는 25%정도로 보 고되어 있다. 본 증례의 환자는 접형동 주위 골을 파괴시키 고 양측 해면 정맥동을 침범하고 있었지만 조직학적으로 I 등급에 해당되어 예후는 좋을 것으로 생각된다.
결론적으로 후각신경아세포종은 비강 상부에서만 발생하 는 것이 아니고 접형동에서도 발생이 가능하므로 고립성 접 형동 질환을 가진 환자에서 감별진단으로 염증성 질환 뿐 아 니라 후각신경아세포종과 같은 종양성 질환도 고려해야 할 것으로 생각된다.
중심 단어:후각신경아세포종·접형동.
REFERENCES
1) McCormack LJ, Harris HE. Neurogenic tumors of the nasal fossa. J Am Med Assoc 1995;157:318-21.
2) Bradley PJ, Jones NS, Robertson I. Diagnosis and management of esthesioneuroblastoma. Curr Opin Otolaryngol Head Neck Surg 2003;
11:112-8.
3) Chacko G, Chandi SM, Chandy MJ. Primary sphenoid and petrous apex esthesioneuroblastoma: case report. Br J Neurosurg 1998;12:
264-6.
4) Chirico G, Pergolizzi S, Mazziotti S, Santacaterina A, Ascenti G.
Primary sphenoid esthesioneuroblastoma studied with MR. Clin Im- aging 2003; 27:38-40.
5) Morris L, Govindaraj S, Genden EM. Primary sphenoid sinus esth- esioneuroblastoma. Am J Otolaryngol 2004;25:350-3.
6) Sharma SC, Reddy CE, Srinivasan SS, Rawal A, Singh DP. Isolat- ed esthesioneuroblastoma of sphenoid sinus. Am J Otolaryngol 2002;
23:287-9.
7) Pack CS, Choi HJ, Kim CS, Kim NS. A case of olfactory neuroblas- toma in sphenoid sinus. Korean J Otolaryngol 2007;50:836-40.
8) Berger L, Luc R, Richard D. The olfactory esthesioneuroepithelioma.
Bull Assoc Franc Etude Cancer 1924;13:410-21.
9) Castelnuovo PG, Delù G, Sberze F, Pistochini A, Cambria C, Batta- glia P, et al. Esthesioneuroblastoma: endonasal endoscopic treatment.
Skull Base 2006;16:25-30.
10) Kadish S, Goodman M, Wang CC. Olfactory neuroblastoma. A clin- ical analysis of 17 cases. Cancer 1976;37:1571-6.
11) Brown SR. Esthesioneuroblastoma. Otolaryngol Head Neck Surg 2007;
137:835-6.
12) Jethanamest D, Morris LG, Sikora AG, Kutler DI. Esthesioneurobl- astoma: a population-based analysis of survival and prognostic fac- tors. Arch Otolaryngol Head Neck Surg 2007;133:276-80.