- 66 -
The Effects of Adenoidectomy on Nasal Airway Resistance and Nasal Geometry
Chan Hee Park, M.D. 1 , Bon Seok Koo, M.D. 1 , A Young Kim, M.D. 1 , Yong De Jin, M.D. 2 , Yong Won Lee, M.D. 1 and Ki Sang Rha, M.D. 1
ABSTRACT
The primary objective of this study was to determine whether adenoid hypertrophy and subsequent adenoidectomy affect pediatric nasal airway resistance and nasal geometry. The secondary objective was to evaluate the relationships between the degree of adenoid hypertrophy and nasal airway resistance or nasal geometry. Fifty-one children, aged 5 to 10 years, selected for adenoidectomy due to chronic nasal obstruction and mouth breathing were enrolled. The size of adenoid was evaluated by cephalometric radiograph. Nasal airway resistance and nasal geometry were evaluated by active anterior rhinomanometry and acoustic rhinometry respectively. These measurements were repeated 3 months after operation. The size of adenoid was found well correlated to preoperative nasal airway resistance but was not to preoperative nasal geometry. Nasal geometry was not changed after operation. However, nasal airway resistance was reduced significantly at 3 months after operation and the size of adenoid was found well correlated to postoperative changes of nasal airway resis tances.
KEY WORDS :Adenoidectomy・Nasal airway resistance・Acoustic rhinometry.
INTRODUCTION
Nasal obstruction is the most common symptom in the otolaryngological field and may be caused by in- flammatory diseases such as infectious rhinosinusitis and allergic rhinitis, by structural deformities such as septal deviation, by congenital diseases such as choanal atresia and by malignant or benign tumors. Unlike in adults, adenoid hypertrophy is common in children and it may be an important cause of symptoms such as nasal obstruction, snoring, and mouth breathing. 1)2)
However there is a controversy about whether nasal resistance, an objective measures in the evaluation of nasal obstruction, increases in patients with adenoid
hypertrophy. Fielder reported that there was a signi- ficant correlation between the preoperative nasal re- sistance and the weight of the adenoid removed at operation. 2) Juliusson et al., also stated that rhinoma- nometry can be a useful method for the selection of children for adenoidectomy. 3) On the other hand, Parker et al., reported that the relationship between the nasal resistance and the size of the adenoid was not strong enough for rhinomanometry to be of use in sele- ction of children for adenoidectomy. 4)
It is suspected that nasal obstruction in patients with adenoid hypertrophy is usually caused by the mass effect of the adenoid tissue located in the nasopharynx.
However, there is also a possibility that adenoid hyper- trophy decreases the airflow passing through the nasal cavity, which may cause chronic congestion of the nasal mucosa causing decrease of the cross-sectional area and volume.
In this study, we wish to study the correlation bet- ween the degree of adenoid hypertrophy evaluated be- fore surgery and objective measures for evaluation of nasal obstruction such as nasal resistance, minimum cross-sectional area or nasal volume. We also wish to analyze the changes of such measures after surgery.
1
Department of Otolaryngology-Head and Neck Surgery, College of Medicine, Chungnam National University, Daejeon, Korea,
2
Department of Otolaryngology, Yanbian University, College of Medicine, Yanji, China
Address correspondences and reprint requests to Ki Sang Rha, M.D., Department of Otolaryngology-Head and Neck Surgery, College of Medicine, Chungnam National University, 640 Dae- sa-dong, Jung-gu, Daejeon 301-721, Korea
Tel:82-2-42-220-7698, Fax:82-42-253-4059 E-mail:[email protected]
Accepted for publication on August 12, 2004
MATERIALS AND METHODS
Fifty-one children, between the ages of 5 and 10, selected for adenoidectomy due to nasal obstruction and mouth breathing, were enrolled. There were 31 male and 20 female patients. Patients with diseases that may affect nasal resistance such as allergic rhinitis, infectious rhinosinusitis, nasal polyp, or nasal septal deviation have been excluded.
In order to evaluate the degree of adenoid hyper- trophy, a simple skull lateral view was taken and the adenoid/nasopharynx diameter ratio (A/N ratio) was obtained according to the method of Fujioka et al. 5) (Fig. 1). The A/N ratio was above 0.5 in all patients.
In order to evaluate subjective symptoms such as nasal obstruction and mouth breathing, a questionnaire was drawn up where 0 represented no symptoms, 1 represented symptoms that come occasionally, 2 for symptoms that come often and 3 for symptoms that always exist.
The nasal resistance and nasal geometry were mea- sured using the RHIN 2000 Acoustic rhinometer-Rh- inomanometer (RhinoMetrics, Denmark). An active anterior rhinomanometry was carried out and the nasal resistance was measured at 150Pa pressure point. The minimum cross sectional area and volume of the nasal cavity was measured by an acoustic rhinometry. It was measured before and 15 min after nasal spray of topical decongestants (0.5% phenylephrine).
An adenoidectomy was performed under endoscopic vision using a microdebrider through a transoral app- roach.
Three months after surgery, subjective symptoms were reevaluated and the active anterior rhinomano- metry and acoustic rhinometry was carried out for com- parison with measurements obtained before surgery.
The statistical evaluation of the data was performed by means of a paired t-test and Pearson correlation through use of the SPSS statistics program, version 10.0. It was considered significant when the p-value was <0.05.
RESULTS
Correlation between the degree of adenoid hy- pertrophy and preoperative nasal resistance or nasal geometry
There was no statistically significant correlation bet- ween the degree of adenoid hypertrophy and preope- rative nasal resistance, minimal cross sectional area, or volume measured before application of topical decon- gestant. However, there was a significant correlation between the degree of adenoid hypertrophy and pre- operative nasal resistance measured after application of topical decongestant (Table 1).
Changes of subjective symptoms after surgery
Symptom score of nasal obstruction significantly decreased from 2.21±1.06 before surgery to 0.13±
0.48 three months after surgery and symptom score of mouth breathing also significantly decreased from 2.62
±0.84 before surgery to 0.25±0.65 three months after surgery (Fig. 2).
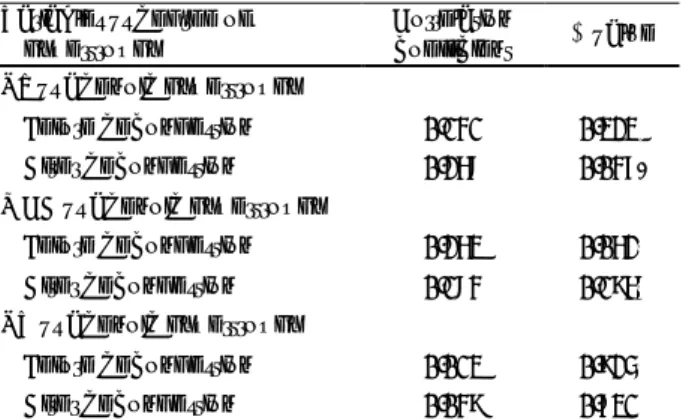
Table 1. Correlation between the degree of adenoid hyper- trophy and preoperative nasal resistance or nasal geometry Variables vs degree of
hypertrophy Correlation
coefficient p value NR vs adenoid hypertrophy
Before decongestion 0.171* 0.229*
After decongestion 0.304* 0.030*
MCA vs adenoid hypertrophy
Before decongestion 0.015* 0.916*
After decongestion 0.080* 0.576*
NV vs adenoid hypertrophy
Before decongestion 0.059* 0.683*
After decongestion 0.030* 0.832*
NR:nasal resistance, MCA:minimum cross-sectional area, NV:nasal volume, *:p<0.05
Fig. 1. A:Adenoidal measurement. “A” represents distance from A’, point of maximal convexity, along inferior margin of adenoid shadow to line B, drawn along straight part of anterior margin of bisiocciput. B:Nasopharyngeal measurement. “N”
is distance between C, posterior superior edge of hard palate, and D, anteroinferior edge of sphenobasioccipital synchon- drosis.
A B
A1
A
B
c N D
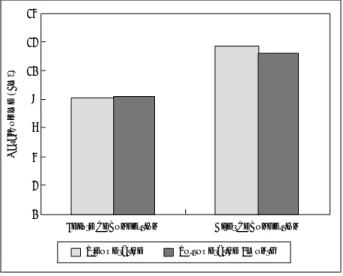
Changes in cross sectional area and volume of the nasal cavity after surgery
The cross sectional area or volume of the nasal cavity was not changed significantly after surgery in both untreated and decongested nose states (Fig. 3, 4).
Changes of nasal resistance after surgery
Nasal resistance before decongestion decreased from 0.76±0.39 Pa・s/cm 3 before surgery to 0.60±0.27 Pa・s/cm 3 three months after surgery but did not show any statistical significance. Nasal resistance in decon- gested state decreased from 0.44±0.19 Pa・s/cm 3 be- fore surgery to 0.38±0.18 Pa・s/cm 3 three months after surgery, showing a statistically significant decrease (Fig. 5).
The correlation of the degree of adenoid hyper- trophy with the postoperative changes of nasal resistance
There was no significant correlation between the degree of adenoid hypertrophy and the degree of pos- toperative changes of nasal resistance measured in un- treated state, however, there was a statistically signifi- cant correlation between the degree of adenoid hyper- trophy and the degree of postoperative changes of nasal resistance measured in decongested state (Table 2).
DISCUSSION
In order to be able to breath well through the nose, not only does the nasal cavity need to be opened but the
Fig. 2. Postoperative changes of symptom score. *:p<0.05.
*
Nasal obstruction 3 *
2.5 2 1.5 1 0.5
0
Mouth breathing
Symptom score