INTRODuCTION
Nasal packing is used for prevention of bleeding and synechiae, and for internal stabilization after sino-nasal surgery involving the cartilaginous-bony skeleton of the nose. Nasal packing is usually left in place for less than 1 week owing to the possibility of infection. Retained nasal packing for a long-time is rare, but can lead to se- rious complications. Herein we report a case of ethmoid sinusitis and a sinocutaneous fistula due to retained non- absorbable nasal packing for 3 months. This report was approved by the institutional review board of the Korea university college of medicine.
CASE REpORT
A 32-year-old man presented with a 2-month history of painful swelling of the left medial canthal area. Three months ago he was hit by a baseball and treated with closed reduction for a nasal bone fracture at a private
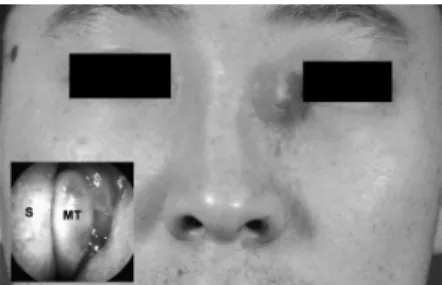
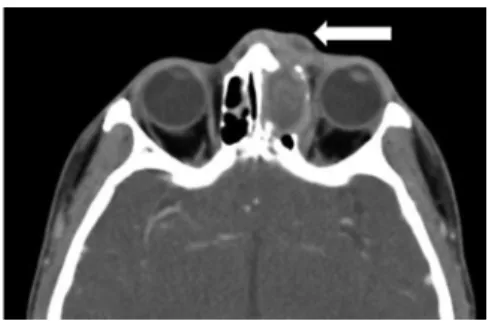
plastic surgery clinic. The physical examination revealed a 2 cm × 2 cm fluctuant mass above the left medial canthal area and over the ethmoid sinus with surrounding celluli- tis (Fig. 1). On endoscopic examination, generalized mu- cosal swelling of the left middle meatus was noted. Clini- cal examination of the cranial nerves, the visual fields, and the vision were normal. Computed tomographic scans of the paranasal sinuses showed left ethmoid sinusitis with an anterior bone defect, and a rim-enhanced low density lesion in the frontal recess and ethmoid sinus which was initially recognized as a mucocele (Fig. 2).
To evaluate the lesion, a detailed endoscopic exami- nation with topical analgesia was performed. A foreign body behind the edematous mucosa deep inside the mid- dle meatus was visualized. The material was not easy to
- 132 -
Sinocutaneous Fistula Induced by Long-Standing, Retained, Non-Absorbable Nasal Packing in The Paranasal Sinus
So-Hea Ok, Nam-Hyung Ryou, Il-Ho Park and Heung-Man Lee
Department of Otorhinolaryngology-Head and Neck Surgery, Guro Hospital, Korea University College of Medicine, Seoul, South Korea
ABSTRACT
Orbital complications after endoscopic sinus surgery (ESS), such as optic nerve or medial rectus injuries, are well known, but isolated complete oculomotor nerve palsy has never been reported. In this case, a 31-year-old male was transferred to our hospital after ESS. Physical examination showed complete left oculomotor nerve palsy, with a bony defect on the sellar floor, which had not fully recovered after more than 1 year. We hypoth- esized that blunt trauma could be the main cause of the oculomotor palsy. Surgeons performing ESS must keep in mind the possibility of oculomotor palsy due to blunt trauma, especially when operating around the sphenoid and posterior ethmoid sinus.
KEY WORDS : Nasal PackingㆍComplicationㆍEthmoid SinusitisㆍSinocutanueous Fistula.
Address correspondence and reprint requests to Heung-Man Lee, MD, PhD Department of Otorhinolaryngology-Head and Neck Surgery Ko- rea University College of Medicine, 80 Guro-dong, Guro-gu, Seoul, 152- 703, South Korea
Tel: +82-2-2626-3185 Fax: +82-2-868-0475 E-mail: [email protected]
Received for publication on August 5, 2014 Accepted for publicatoin on October 22, 2014
Fig. 1. The physical examination revealed a 2 cm×2 cm fluc- tuant mass above the left medial canthal area and over the ethmoid sinus with surrounding cellulitis (inlet; nasal endoscopic finding).
J Rhinol 21(2), 2014 www.ksrhino.or.kr
133 / J Rhinol 21(2), 2014
remove due to adhesions. Thus, we planned endoscopic sinus surgery under general anesthesia. During surgery, the material appeared to be non-absorbable nasal packing (Merocel HemoX, 1.5 cm × 2 cm sized) and was meticu- lously removed. There were numerous adherent remnants, all of which were completely removed. The frontal recess was widened due to the space-occupying effect of the non-absorbable nasal packing. The ethmoidectomy was completed and the frontal sinus recess was widened ad- equately, we did not do further procedure such as incision and drainage.
The patient was discharged 3 days after surgery and one week after, the symptoms had resolved without any com- plications. At the 6-month post-operative visit, the frontal sinus ostium was patent on nasal endoscpic examination and no skin wound complications were observed. There was no medicolegal prolem in this patient.
DISCuSSION
Nasal packing is widely used after sinonasal proce- dures. Even though nasal packing prevents bleeding and synechiae, there are potential complications, such as sep- tal perforation, dislocation with possible aspiration, dis- turbance of breathing during sleep or a decrease in noc- tural arterial pO2, eustachian tube dysfunction, allergic reactions, toxic shock syndrome, paraffin granulomas, and infections.1) In the case of non-absorbable packing, there is a high possibility of bacterial growth by formation of bacterial biofilm.2) To prevent these complications, the packing should be removed at the appropriate time and the surgeon should confirm that packing material has not been retained at the surgical site. In most cases, nasal packing is unlikely to be retained owing to the need for endoscopic debridement after surgery.4)
Merocel HemoX is a polymer made from esterified hy- aluronic acid. Merocel HemoX absorbs liquids and trans- forms liquids into a mucoadhesive gel at the site of the surgical wound. Weber et al.1) reported that occlusion of
the drainage of the maxillary sinus and anterior ethmoid by a piece of Merocel HemoX encourages the develop- ment of post-operative acute sinusitis.
Sinocutaneous fistulas are uncommon complications of chronic sinusitis, usually developed secondary to frontal sinusitis. Patients with sinocutaneous fistulas may present symptoms of headache, sinus pressure and pain, conges- tion, rhinorrhea, forehead swelling, visual complaints, and neurologic changes. A sinocutaneous fistula can be devel- oped after an injury to the anterior frontal bone, creating communication between the sinus and skin. Such an inju- ry can be the result of osteomyelitis and necrosis of bone, erosion of the bone via a mucocele or tumor, or traumatic injury to the bone.3) In our case, frontal and ethmoid si- nusitis caused by long-standing, retained, non-absorbable nasal packing and a ethmoid sinus anterior wall fracture caused ethmoid sinusitis resulted in a sinocutaneous fis- tula. There is no other literature about sinocutaneous fis- tula developed secondary to ethmoid sinusitis or foreign body reaction.
We concluded that if nasal packing is performed by a surgeon who is not familiar with the anatomy of the nasal cavity and sinus, there is a possibility of missing and re- taining the packing. Retained nasal packing can result in serious complications. Therefore careful insertion in the appropriate anatomical site as well as attentive removal is important.
저자역할(Author Contributions)
옥소혜, 박일호는 본 연구에서 모든 자료에 접근할 수 있으며, 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습니다. 연구기획 : 옥 소혜, 박일호. 환자진찰 및 분석 : 옥소혜, 류남형. 논문초안 : 옥소 혜, 류남형. 연구 총괄 : 이흥만.
REFERENCES
1) Weber R, Keerl R, Hochapfel F, et al. Packing in endonasal sur- gery. Am J Otolaryngol 2001;22:306-20.
2) Yanjun Wang, Shan Chen, Jianjun Chen, et al. Bacterial biofilm formation after nasal packing in nasal mucosa – wounded mice.
Am J Rhinol Allergy 2013;27: e91-5.
3) Wu VF, Smith TL, Poetker DM. Sinocutaneous fistula second- ary to chronic frontal rhinosinusitis: case series and litera ture review. Ann Otol Rhinol Laryngol 2008;117:759-63.
4) Weber R, Hochapfel F, Draf W. Packing and stents in endonasal surgery. Rhinology 2000;38:49-62.
5) Huang IT, Podkomorska D, Murphy MN, et al. Toxic shock syn- drome following septoplasty and partial turbinectomy. J Otolar- yngol 1986;5:310-2.
6) Beste DJ, Capper DT, Shaffer K, et al. Antimicrobial effect on rabbit sinusitis after temporary ostial occlusion. Am J Rhinol 1997;11:485-9
Fig. 2. Axial computed tomogram of paranasal sinuses shows opacification of the left ethmoid sinus with bone erosion and swelling of overlying soft tissue and skin (white arrow).