- 102 -
Glucocorticoid Receptor-β Overexpression According to Nasal Polyp Severity:Immunohistochemical Study
Yong-Hwi An, MD1, Sung-Lyong Hong, MD1, Doo Hee Han, MD1, Jee Hye Wee, MD1, Chae-Seo Rhee, MD1,2,3, Chul Hee Lee, MD1,2 and Yang-Gi Min, MD1,2
1Department of Otorhinolaryngology, Seoul National University Hospital; and
2Research Center for Sensory Organs; and 3Institute of Allergy and Clinical Immunology, Seoul National University Medical Research Center, Seoul, Korea
ABSTRACT
Background and Objectives:The aims of the study were to reintroduce a surgical technique for a “mini” Caldwell-Luc operation and to determine its efficacy. Materials and Methods:A prospective study was performed in 23 patients undergo- ing the “mini” Caldwell-Luc operation. Improvements in clinical symptoms and endoscopic and computed tomographic (CT) findings were evaluated postoperatively over a follow-up period ranging from 6 to 21 months. All patients were surveyed for nasal symptoms (nasal obstruction, rhinorrhea, posterior nasal drip, headache, and anosmia), complications (tooth or gum pain, numbness, persistent facial pain, and facial hypo-paresthesia), and recurrence. Preoperative nasal polyps were classified by the Gaskins method, and preoperative paranasal sinusitis was graded according to the Kennedy CT staging system. Re- sults:Symptom scores were all significantly reduced postoperatively (paired t-test, p<0.05). There were no major complica- tions specific to this technique. Among 29 maxillary sinuses that received the “mini” Caldwell-Luc operation, seven showed recurrence (24%). Conclusion:The “mini” Caldwell-Luc operation provides an alternative method of obtaining access to the maxillary antrum and is associated with minimal morbidity.
KEY WORDS:Caldwell-Luc operationㆍChronic maxillary sinusitisㆍEndoscopic sinus surgery.
Address correspondences and reprint requests to Yang-Gi Min, M.D., Department of Otorhinolaryngology, Seoul National University Hospital, 101 Daehangro, Jongno-gu, Seoul 110- 744, Korea
Tel:82-2-2072-2446, Fax:82-2-745-2387 E-mail:[email protected] Received for publication on May 10, 2010 Accepted for publication on September 27, 2010
INTRODUCTION
Nasal polyposis which is characterized by edematous inflamed mucosa is a chronic inflammatory disease of the nose and paranasal sinuses.1) Although glucocorti- coids have been widely used for the treatment of nasal polyp, responses to corticosteroid therapy are frequently unsatisfactory. Recent studies regarding glucocorticoid receptor (GR) have demonstrated its important role in the cellular regulation against glucocorticoid resistance.2-4) This study is based on the assumption that the mecha- nisms of steroid insensitivity in human tissues are related to the change in receptor distribution.
Two subclasses of GRs have been identified : GR-α
which performs normal functions, and GR-β which struc- turally does not bind to glucocorticoid and, therefore, functionally related to steroid insensitivity.5) The patho- genesis of steroid dependency and resistance is thought to be a complex network of many different factors though there is no general agreement on these responses. Focused on a molecular basis of corticosteroid receptors in human nasal tissues, an up-regulation of GR-β expression has been reported to be a landmark of steroid resistance in na- sal polyps.6)
In this study, we used immunohistochemistry to evalu- ate the expression of GRs in steroid-insensitive nasal polyps and compared it with that in normal nasal muco- sae. We also determined whether the expression of GR-β in nasal polyps would differ according to their severity.
MATERIALS AND METHODS
Patients
Nasal biopsy specimens including the nasal polyp and
middle turbinate mucosae were obtained from 16 patients diagnosed with chronic rhinosinusitis and nasal polypo- sis between September 2006 and September 2007 (9 males, 7 females ; mean±SEM, 48±12 years) who un- derwent endoscopic sinus surgery (the nasal polyp group). These patients did not have a history of asthma, aspirin sensitivity or allergic rhinitis. In this study, oral or intranasal corticosteroids were administered in all pa- tients. Eleven patients were treated with topical cortico- steroids for at least 4 weeks. Five patients were treated with systemic glucocorticoids for at least 2 weeks. None of the nasal polyps responded to steroid therapy. System- ic and intranasal steroids were discontinued for minimum 1 month before biopsy. Samples of the middle turbinate tissue from 4 patients (2 males, 2 females ; mean±SEM, 42±15 years) who underwent septorhinoplasty or transs- phenoidal hypophysectomy were used as controls (the control group). These 4 patients had no history of airway diseases including sinonasal disease. All patients in the nasal polyp and control groups gave written informed consent to the study. This study was approved by the In- stitutional Review Board of Seoul National University Hospital (H-1008-049-326).
Staging of nasal polyps
The classification system described by Lund and Mackay for grading nasal polyposis7) was used : grade 0, no visible polyp ; grade 1, mild polyp(s) confined to middle meatus ; grade 2, moderate polyp(s) beyond mid- dle meatus but not completely obstructing the nasal cavi- ty ; and grade 3, severe polyp(s) completely obstructing the nasal cavity. Endoscopic grading of nasal polyps was recorded by a single observer the day before operation.
Immunohistochemistry
Biopsy samples from the polyps and normal nasal mu- cosae were processed for immunohistochemical staining using the avidin-biotin complex method as previously described.8) GR-α specific polyclonal rabbit antibody (Santa Cruz Biotechnology, Santa Cruz, CA) at a dilution of 1 : 200, and rabbit GR-β polyclonal antibody (Calbio- chem, San Diego, CA) at a dilution of 1 : 100 were pre- pared as primary antibodies. Biotinylated anti-rabbit per- oxidase secondary antibody (Vector Laboratories, Burlingame, CA) was used at a dilution of 1 : 200 to de- tect these primary antibodies. The brown immunoperoxi- dase reaction was developed with diaminobenzidine, and
the sections were counterstained with hematoxylin. For negative control preparations, primary antibodies were replaced with nonspecific rabbit immunoglobulin.
Quantification
Positive cells for each of the primary antibodies were counted through use of a light microscope (Leitz micro- scope, Wetzlar, Germany) with an eyepiece reticule at x200 magnification. To avoid the observer bias, tissue sections were assessed by a single investigator in a blind fashion. The 0.2-mm2 reticule was oriented beneath the epithelial basement membrane, and both positive and nega- tive cells were counted at 5 randomly selected fields.
Statistics
Data were expressed as mean±SEM. Between-group comparisons were performed by using the Mann-Whit- ney U test. The relationship between the expression of GR-β and the severity of nasal polyps was determined by the Wilcoxon signed rank test. Differences were consid- ered statistically significant at p<.05.
RESULTS
Grading of nasal polyp
Of the total 16 patients, 1 had mild polyps (grade 1 nasal polyp), 10 had moderate polyps (grade 2 nasal polyp) and 5 had severe polyps (grade 3 nasal polyp). The control group had no polyp (Table 1).
Distribution of GRs in nasal tissues
Immunostaining was positive for GRs in the nasal pol- yp and control groups as illustrated in Fig. 1. Receptor- positive cells were stained brown and were predominant- ly localized in the epithelial cells and submucosal
Table 1. Demographics and endoscopic grading of nasal polyp Nasal polyp
group (n=16)
Control group
(n=4) Sex (male : female)
Median age (year) NP grade* No NP Mild NP Moderate NP Severe NP
9 : 7 48
0 1 10 5
2 : 2 42
4 0 0 0 NP : nasal polyp. * : According to the Lund and Mackey stag- ing system by endoscopic findings
inflammatory cells. There were more cells expressing GRs in the epithelium than in the submucosa of the nasal polyp and control groups.
Comparison of GR-α expression
GR-α-positive cells were found in both nasal polyps (53±15 cells/mm2) and middle turbinate mucosae (51±
8 cells/mm2) from the nasal polyp group as well as mid- dle turbinate mucosae (43±11 cells/mm2) from the con- trol group. The absolute numbers of these cells in nasal polyps from the nasal polyp group were not significantly different from those in the control group (p>.05). The absolute numbers of these cells in nasal polyps from the middle turbinate from the nasal polyp group were not significantly different from those in the control group (p>.05)(Fig. 2).
Comparison of GR-β expression
GR- β was expressed in the nasal polyps (36±8 cells/
mm2) and middle turbinate mucosae (25±4 cells/mm2) from the nasal polyp group and the middle turbinate mu- cosae (17±3 cells/mm2) from the control group. GR-β was more expressed in nasal polyps from the nasal polyp group than in middle turbinate mucosae from the control group (p=.01). In addition, the number of GR-β-positive cells was significantly increased in the middle turbinate mucosae from the nasal polyp group as compared to the middle turbinate mucosae from the control group (p=.03) (Fig. 3).
Association of GR-β expression with the severity of nasal polyps
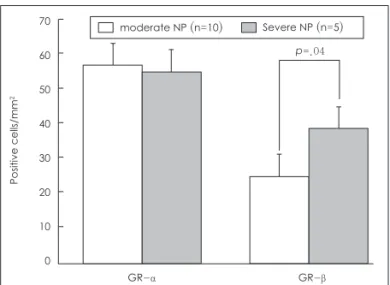
For grade 2 nasal polyps, immunohistochemical stain-
Fig. 1. Immunolocalization of GR-α (A) and GR-β (B) in a nasal polyp and GR-α (C) and GR-β (D) in a normal middle turbinate mucosa.
GR-α and GR-β are more localized in the epithelial cells and infiltrating inflammatory cells of the subepithelial layer than in the endothe- lial cells (×200).
A B C D
Fig. 2. Expression of GR-α in the nasal polyps and middle turbi- nate mucosae of the nasal polyp group (n=16) and in the con- trol group (n=4). There was no significant difference in GR-α ex- pression between the nasal polyps of the nasal polyp group and the middle turbinate mucosae of the normal control group (p>.05). There was no significant difference in GR-α expression between the middle turbinate mucosae of the nasal polyp group and the middle turbinate mucosae of the normal control group (p>.05). NP : nasal polyp, MT : middle turbinate mucosa.
70 60 50 40 30 20 10
0
Nasal polyp group Control group
NP MT
Positive cells/mm2
Fig. 3. Expression of GR-β in the nasal polyps and middle turbi- nate mucosae of the nasal polyp group (n=16) and in the mid- dle turbinate mucosae of the control group (n=4). The number of GR-β positive cells was more increased in the nasal polyp of the nasal polyp group than in the control group (p=.01). Also, the number of GR-β-positive cells was more increased in the middle turbinate mucosae of the nasal polyp group than in the middle turbinate mucosae of the control group (p=.03). Abbre- viations as in Fig. 2.
50 45 40 35 30 25 20 15 10 5 0
Nasal polyp group Control group
NP MT
Positive cells/mm2
p=.01 p=.03
from those of previous study with multiple human tis- sues17) and are similar to those of previous studies with nasal polyps.6)11) Expression of GR-β in the epithelium may not have clinical implications because most types of inflammatory cells such as eosinophils and T lympho- cytes were predominant in the submucosa. However, our results indicate that the epithelium has a crucial role in the interactions between insensitivity to glucocorticoid and polyp development. There is no doubt that the sub- mucosa is the main site of the inflammatory process in polyp formation.1)18)
We demonstrated in this study that the number of GR- β-positive cells was increased in nasal polyps. In con- trast, there was no evidence of overexpression of GR-α in nasal polyps compared to normal mucosae. The ratio of GR-β-positive to GR-α-positive cells representing cor- ticosteroid unresponsiveness has been shown to differ among previous studies.6)11)16)Our results revealed that the ratio of GR-β-positive to GR-α-positive cells was higher in grade 3 nasal polyps than in grade 2 nasal polyps. Fur- thermore, the GR-β/GR-α ratio tended to increase in ste- roid-resistant nasal polyps compared to normal turbinate mucosae, but this difference was not statistically signifi- cant (p=.058, data not shown). Although there is still controversy regarding GR-β function, we assumed that up-regulation of GR-β is a marker of steroid insensitivity for nasal polyps. GR-β was more expressed in severe na- sal polyps than in moderate polyps. This potentially ex- plains the molecular basis of unresponsiveness to gluco- corticoid therapy in nasal polyposis. Such possibility may be supported by in vitro superantigen-induced GR-β expression in a nasal explant model19) and by in vivo GR-β overexpression in topical steroid-insensitive nasal polyps.6)
The small number of specimens is a limiting factor in this study. In contrast to many studies on nasal polyps, in which samples of nasal polyps were used as study group, we think that using both nasal polyps and middle turbi- nate mucosa will give a more accurate representation, as the majority of nasal polyps arise from middle turbi- nate.20) This choice, however, limited the number of specimens, as removal of middle turbinate mucosa is not often performed in patients with nasal polyposis. Non- specific immunostaining of inflammatory cells is also a weak point of our study. Some studies showed the details of immunoreactivity for inflammatory cells such as T lymphocytes, eosinophils, and macrophages,6)11) but oth- ers didn’t.8)16) To understand the significance of the loca- tion of GR-β expression in nasal polyps, a detailed analy- ing was positive for GR-α in 57±9 cells/mm2 and for
GR-β in 25±6 cells/mm2, whereas for grade 3 nasal pol- yps, it was positive for GR-α in 55±9 cells/mm2 and for GR-β in 39±5 cells/mm2. No difference in GR-α expres- sion was found between grade 2 and 3 polyps (p>.05), while a significant increase of GR-β expression was ob- served in grade 3 nasal polyps as compared to grade 2 nasal polyps (p=.04)(Fig. 4). In addition, the ratio of GR- β-positive cells to GR-α-positive cells was higher in grade 3 nasal polyps than in grade 2 nasal polyps (0.73±
0.15 vs. 0.42±0.09 ; p=.03).
DISCUSSION
The etiology and pathogenesis of nasal polyposis has not yet been elucidated. However, there is evidence that glucocorticoid-related cellular immune responses may play an important role in its pathophysiology.9)10) Expres- sion of GR-β is increased in steroid-insensitive nasal pol- yps6)11) as well as in another glucocorticoid-resistant dis- eases, such as persistent asthma,8)12) ulcerative colitis13) and chronic lymphoblastic leukemia.14) However, until recently, there has been controversy regarding this.15)16) We hypothesized that GR-β may expressed in nasal pol- yps as compared to normal nasal mucosae, and that as steroid unresponsiveness becomes higher, GR-β expres- sion will be more increased.
In this study, it was found that GR-β was significantly more expressed in nasal polyps, especially in the epithe- lium than in the submucosa. These results are different
Fig. 4. Expression of GR-α and GR-β in the nasal polyps of the nasal polyp group according to the severity of nasal polyps.
The number of GR-β-positive cells was more increased in severe nasal polyps (N=5) than in moderate nasal polyps (N=10) (p=.04), whereas the number of GR- α-positive cells was not in- creased in severe nasal polyps as compared in moderate nasal polyps. Abbreviations as in Fig. 2.
70 60 50 40 30 20 10
0
GR-α GR-β moderate NP (n=10) Severe NP (n=5)
Positive cells/mm2
p=.04
sis of cell types should be continued.
CONCLUSION
We demonstrated that GR-β is more-expressed accord- ing to nasal polyp severity by using the immunohisto- chemical staining. The results of this study suggest that increased expression of GR-β in nasal tissue may con- tribute to the pathogenesis and progression of nasal pol- yposis and that the relationship between the expression of GR-β and the severity of nasal polyps may be related to the progression of nasal polyposis and steroid resis- tance. Further studies are needed to confirm our results.
Acknowledgments
This work was supported by grant No. 04-2006-071-0 from the Seoul National University Hospital Research Fund.
저자역할(Author Contributions)
안용휘, 이재서, 이철희, 민양기는 본 연구에서 모든 자료에 접근 할 수 있으며 자료의 완전성과 자료 분석의 정확성에 책임을 지고
있습니다. 연구 구상과 설계:안용휘, 홍성룡, 이재서, 이철희,
민양기. 자료 분석 및 해석:안용휘, 홍성룡, 한두희, 위지혜, 이 철희, 이재서, 민양기. 논문초안:안용휘, 한두희, 이재서, 이철희.
논문수정:안용휘, 홍성룡, 한두희, 위지혜, 이재서, 이철희, 민 양기. 연구 감독:한두희, 이재서, 이철희, 민양기.
REFERENCES
1) Mygind N. Nasal polyposis. J Allergy Clin Immunol 1990;86:827-9.
2) Vanderbilt JN, Miesfeld R, Maler BA, Yamamoto KR. Intracellu- lar receptor concentration limits glucocorticoid-dependent en- hancer activity. Mol Endocrinol 1987;1:68-74.
3) Chrousos GP, Castro M, Leung DY, Webster E, Kino T, Bam-berger C, et al. Molecular mechanism of glucocorticoid resistance/hyper- sensitivity - Potential clinical implications. Am J Respir Crit Care Med 1996;154:S39-44.
4) Knutsson PU, Bronnnegard M, Marcus C, Stierna P. Regulation of glucocorticoid receptor mRNA in nasal mucosa by local adminis- tration of fluticasone and budesonide. J Allergy Clin Immunol 1996;97:655-61.
5) Oakley RH, Jewell CM, Yudt MR, Bofetiado DM, Cidlowski JA.
The dominant negative activity of the human glucocorticoid recep- tor beta isoform. Specificity and mechanisms of action. J Biol Chem 1999;274:27857-66.
6) Hamilos DL, Leung DY, Muro S, Kahn AM, Hamilos SS, Thawley SE, et al. GRbeta expression in nasal polyp inflammatory cells and its relationship to the anti-inflammatory effects of intranasal fluticasone. J Allergy Clin Immunol 2001;108:59-68.
7) Lund VJ, Mackay IS. Staging in rhinosinusitis. Rhinology 1993;31:
183-4.
8) Hamid QA, Wenzel SE, Hauk PJ, Tsicopoulos A, Wallaert B, Lafitte JJ, et al. Increased glucocorticoid receptor beta in airway cells of glucocorticoid-insensitive asthma. Am J Respir Crit Care Med 1999;
159:1600-4.
9) Larocca LM, Maggiano N, Capelli A, Bevilacqua P, Ruscito P, Maurizi M, et al. Immunopathology of nasal polyps: an immunohisto- chemical approach. Ann Allergy 1989;63:508-12.
10) Stoop AE, van der Heijden HA, Biewenga J, van der Baan S. Clin- ical aspects and distribution of immunologically active cells in the nasal mucosa of patients with nasal polyps after endoscopic sinus surgery and treatment with topical corticosteroids. Eur Arch Oto- rhinolaryngol 1992;249:313-7.
11) Pujols L, Mullol J, Benítez P, Torrego A, Xaubet A, de Haro J, et al. Expression of the glucocorticoid receptor alpha and beta iso- forms in human nasal mucosa and polyp epithelial cells. Respir Med 2003;97:90-6.
12) Sousa AR, Lane SJ, Cidlowski JA, Staynov DZ, Lee TH. Gluco- corticoid resistance in asthma is associated with elevated in vivo ex- pression of the glucocorticoid receptor b-isoform. J Allergy Clin Im- munol 2000;105: 943-50.
13) Honda M, Orii F, Ayabe T, Imai S, Ashida T, Obara T, et al. Ex- pression of glucocorticoid receptor beta in lymphocytes of patients with glucocorticoid-resistant ulcerative colitis. Gastroenterology 2000;118:859-66.
14) Shahidi H, Vottero A, Stratakis CA, Taymans SE, Karl M, Longui CA, et al. Imbalanced expression of the glucocorticoid receptor isoforms in cultured lymphocytes from a patient with systemic gluco- corticoid resistance and chronic lymphocytic leukemia. Biochem Biophys Res Commun 1999;254:559-65.
15) Hecht K, Duke JC, Stierna P, Gustafsson JA, Bronnegard M, Wik- strom AC. Evidence that the β-isoform of the human glucocorticoid receptor does not act as a physiologically significant repressor. J Biol Chem 1997;272:26659-64.
16) Gagliardo R, Chanez P, Vignola AM, Bousquet J, Vachier I, Godard P, et al. Glucocorticoid receptor alpha and beta in glucocorticoid de- pendent asthma. Am J Respir Crit Care Med 2000;162:7-13.
17) Okret S, Dong Y, Bronnegard M, Gustafsson JA. Regulation of gluco- corticoid receptor expression. Biochimie 1991;73:51-59.
18) Kirtsreesakul V. Update on nasal polyps: etiopathogenesis. J Med As- soc Thai 2005;88:1966-72.
19) Fakhri S, Tulic M, Christodoulopoulos P, Fukakusa M, Frenkiel S, Leung DY, et al. Microbial superantigens induce glucocorticoid receptor beta and steroid resistance in a nasal explant model. Laryn- goscope 2004;114:887-92.
20) Stammberger HR. Rhinoscopy: endoscopic diagnosis. In: Naclerio RM, Durham SR, Myrind H, eds. Rhinitis: mechanisms and manage- ment. New York, NY: Marcel Dekker;1999. p.165-73.