서 론
요산은 퓨린의 대사과정의 최종산물이며 대부분이 간에서 요산 산화효소에 의해 알란토인으로 산화된다.1) 혈중 요산의 약 70%는 세 포의 내인성 퓨린 대사에 의해 생성되고, 30%는 음식으로 섭취된 퓨 린으로부터 형성되어 대부분 신장을 통해 배설된다.1) 혈중 요산 농 도는 인종에 따라 차이가 있으며 식습관과 체지방에 의해서도 영향
을 받는다.1) 1951년 Gertler 등2)에 의해 증가된 혈중 요산 농도와 심혈 관질환 사이의 연관성에 대한 보고가 있었다. 그 이후 National Health and Nutrition Examination Survey (NHANES I) 역학추적연구3) 에 의하면 증가된 혈중 요산 농도는 심혈관질환의 사망률과 독립적 으로 유의한 연관성이 있었고 Alderman 등4)이 시행한 연구에서 혈 중 요산 농도와 심혈관질환 발생률 사이의 독립적인 연관성을 관찰 할 수 있었다. 하지만 Framingham Heart Study5)에서는 혈중 요산이
Original Article
혈중 요산 농도와 심혈관질환 위험인자 및 관상동맥석회화 점수와의 관련성
최나영, 고현민*, 이정휘
성균관대학교 의과대학 삼성창원병원 가정의학교실
Association of Serum Uric Acid Level with Risk Factors of Cardiovascular Disease and Coronary Artery Calcium Score
Na-Young Choi, Hyun-Min Koh*, Jung-Hui Lee
Department of Family Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
Background: Many studies have investigated but failed to clarify the correlation between serum uric acid level, cardiovascular risk factors, and coronary artery calcification. This study attempted to elucidate this correlation in adult patients that visited a health promotion center.
Methods: Enrolled subjects included adult patients that visited a Samsung Changwon Hospital health promotion center for examinations, between January and December 2013, and whose serum uric acid levels and coronary artery calcium scores (CACS) were measured. Using a CACS of 0 as a standard, the subjects were divided into a non-calcification group with scores of 0 and a calcification group with scores exceeding 0. Differences in the general characteristics of the two groups were analyzed using the t-test and chi-square test. Pearson correlation coefficients were calculated to assess the correlation between serum uric acid level and cardiovascular risk factors. The odds ratio for the association of serum uric acid level with coronary artery calcification was analyzed by logistic regression analysis.
Results: Serum uric acid showed significant positive correlations with total cholesterol, triglyceride, and waist circumference. It was also significantly positively correlated with high-sensitivity C-reactive protein and CACS. The same results were obtained even after adjustment for age and sex, factors that exerted the most effects. Moreover, increased serum uric acid was a significant risk factor for coronary artery calcification (odds ratio, 1.107; 95% confidence interval, 1.012–1.210).
Conclusion: Serum uric acid level is independently and positively associated with cardiovascular risk factors and CACS.
Keywords: Serum Uric Acid; Cardiovascular Risk Factors; Coronary Artery Calcium Score; Subclinical Atherosclerosis
http://dx.doi.org/10.21215/kjfp.2016.6.4.215eISSN 2233-9116
Korean J Fam Pract. 2016;6(4):215-220
KJFP
Korean Journal of Family PracticeReceived March 15, 2016 Revised May 6, 2016 Accepted June 1, 2016 Corresponding author Hyun-Min Koh
Tel: +82-55-290-5522, Fax: +82-55-290-1224 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Na-Young Choi, et al. Serum Uric Acid Level and Coronary Artery Calcium Score
Korean Journal of Family Practice
KJFP
심혈관질환의 발생과 심혈관질환에 의한 사망에 독립적인 위험 요 인이 아니라고 보고하였고 Atherosclerosis Risk in Communities (ARIC) Study6)에서도 혈중 요산이 심혈관질환의 독립적인 위험요인 이 아니라고 보고하였다. 따라서 요산이 심혈관질환의 발생에 독립 적인 역할을 하는지에 대하여 아직 논란이 있다.
임상적 관상동맥질환이 없는 사람에서 심혈관질환의 위험도를 평가하기 위한 전통적인 지침으로는 미국의 Framingham risk score 와 유럽의 SCORE system 등이 알려져 왔다.7,8) 그러나 최근에는 다중 절편 방사선단층촬영(multidetector computed tomography, MDCT) 을 이용하여 관상동맥석회화(coronary artery calcium, CAC)를 진단 하는 비침습적인 방법이 새롭게 대두되고 있고 MDCT로 검출된 CAC를 수치로 나타낸 관상동맥석회화 점수(coronary artery calcium score, CACS)는 Framingham risk score 내의 전통적인 위험인자보다 심혈관질환 발생의 독립적인 예측도가 높은 것으로 알려져 있다.9-11)
혈중 요산과 동맥경화증의 관련성에 대한 연구는 많지 않으며 주 요 기전 또한 명확하지 않다. 최근 혈중 요산과 CACS 간의 관련성을 본 연구가 있었으나 의견의 일치가 이루어지지 않았고,12-14) 일부 군에 서 규명된 결과로 일반화하기에는 연구가 부족한 실정이다.
이에 본 연구는 삼성창원병원 건강증진센터를 내원한 건강한 성 인에서 혈중 요산과 전통적인 심혈관질환의 위험인자 및 CACS 간의 상관관계에 대하여 분석하고자 하였다.
방 법
1. 연구대상
본 연구는 2013년 1월부터 2013년 12월까지 12개월 동안 건강검진 을 목적으로 경남 창원시 삼성창원병원 건강증진센터에 내원하여 MDCT를 시행한 성인 수검자 5,155명 중 고요산혈증에 대한 약을 복용중이거나 통풍을 진단받은 환자 및 무응답자를 제외한 5,014명 을 대상으로 하였다. 연구참여자들을 대상으로 서면 사전 동의를 받 은 후 연구를 시행하였다. 본 연구는 본원 연구윤리심의위원회의 승 인을 받아 진행하였다(IRB No. 2016-SCMC-012-00).
2. 측정변수
건강증진센터에 내원한 모든 성인 수검자들은 사전에 문진표를 작성하였고, 문진표에는 사회인구학 요인들과 생활습관(흡연, 규칙 적인 운동), 질병 과거력 및 치료 유무(통풍, 고혈압, 당뇨병)에 관한 정보가 포함되었다. 흡연은 현재 흡연자, 비흡연자의 두 가지로 분류 하였고 운동은 주 3회 이상 걷기를 제외하고 평소보다 몸이 매우 힘 들거나 숨이 많이 가쁜 중등도 신체활동을 하는 경우를 운동군으
로, 그 이하를 비운동군으로 분류하였다. 신장과 체중은 신발을 벗 고 가벼운 옷차림으로 직립한 자세에서 자동화기기(BSM330; Bio- space, Seoul, Korea)를 이용하여 측정하였다. 비만도는 체질량지수를 산출하여 이용하였다. 허리둘레는 가벼운 옷을 입고 직립자세로 최 하위 늑골하부와 골반 장골능선 사이에서 가장 좁은 둘레를 지면 과 평행하게 측정하였다. 혈압은 수은 혈압계를 이용하였다. 혈압 측 정 전 10분 이상 안정을 취하게 한 후 앉은 자세에서 수축기와 이완 기 혈압을 측정하고, 5분 뒤 반복 측정하여 평균을 이용하였다. 혈압 측정 시 상완부 팔 둘레의 길이를 측정한 후 80% 이상을 감을 수 있 는 커프를 사용하였으며, 심장높이에 혈압 측정띠가 위치하게 하여 측정하였다.
최소 8시간 금식한 상태에서 정맥혈을 채혈하였고 혈당, 당화혈색 소(HbA1c), 인슐린, 총콜레스테롤, 저밀도지단백콜레스테롤(low density lipoprotein cholesterol, LDL-C), 고밀도지단백콜레스테롤 (high density lipoprotein cholesterol, HDL-C), 중성지방(triglyceride, TG), 고감도 C 반응성 단백질(high sensitivity C-reactive protein, hs- CRP), 크레아티닌, 요산을 측정하였다.
3. 관상동맥석회화 점수 측정
64절편 MDCT 스캐너(SOMATOM Definition AS+Excel Edition;
Siemens, Munich, Germany)를 사용하였으며, 관상동맥 조영을 위해 사용되는 표준방식에 따라 측정하였다. MDCT 촬영 전 최소 8시간 금식을 하였다. MDCT로 촬영된 영상은 관상동맥 경로를 따라 130 Hounsfild Unit (HU) 이상의 감쇠를 보이는 영역을 석회화로 정의하 였고, Agatston 등15)에 의해 발표된 방법에 따라 CACS를 측정하였다.
CACS는 0보다 큰 경우를 coronary artery calcification이 있는 것으로 간주하였으며 CACS=0인 경우를 비석회화군, CACS >0인 경우를 석 회화군으로 정하였다.
4. 통계 분석
데이터의 편향을 감소시키기 위해 인슐린, TG, hs-CRP는 Log로 변환시켜서 분석하였다. 수검자 중 일부에서만 CAC가 검출되었기 때문에 우측 편향을 감소시키기 위해 CACS 값에 1을 더한 후 Log로 변환시켜서 분석하였다. 연구대상자들을 연속형 변수들은 평균과 표준편차를 구하였으며 명목형 변수들은 chi-square 검정으로 분석 하였고 CACS=0, CACS >0인 두 그룹으로 나누어 분석하였다. 혈중 요산과 총콜레스테롤, Log TG, Log hs-CRP, 허리둘레, Log (CACS+1) 의 Pearson 상관계수를 구하였고 연령과 성별을 보정한 후의 값도 구 하였다. CACS에 영향 을 주는 위험인자 를 알아보기 위하여 CACS=0, CACS >0인 그룹에 대하여 성별, 연령, 공복혈당, 당화혈색
최나영 외. 혈중 요산농도와 관상동맥석회화점수 Korean Journal of Family Practice
KJFP
소, 총콜레스테롤, Log TG, 혈중 크레아티닌, 혈중 요산, 체질량지수, 수축기 혈압, 이완기 혈압, 당뇨, 고혈압, 흡연, 운동을 위험인자로 설 정하고 다변량 회귀분석을 하였다. 통계 분석 프로그램은 IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA)과 R 3.1.0 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/)을 이용하였고 유의수준은 P<0.05를 기준으로 하였다.
결 과
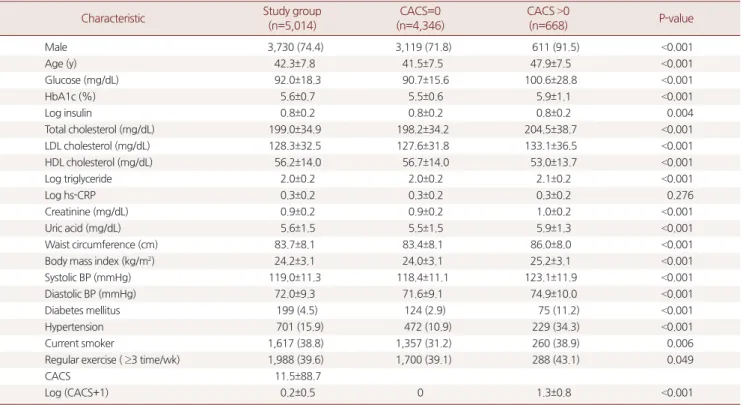
1. 연구대상자의 일반적인 특성(Table 1)
연구대상자는 총 5,014명으로 남자는 3,730명(74.4%)이었으며 평균 연령은 42.34세였다. 당뇨병을 진단받은 대상자는 199명(4.5%), 고혈 압을 진단받은 대상자는 701명(15.9%)이었다. CACS >0으로 석회화 군에 속하는 수검자는 668명(13.3%)이었으며 CACS의 평균은 11.54 였다.
평균 혈중 요산 농도는 전체 5.57 mg/dL였고 비석회화군에서 5.51
Table 1. Baseline characteristics of subjects according to the presence of CACS
Characteristic Study group
(n=5,014)
CACS=0 (n=4,346)
CACS >0
(n=668) P-value
Male 3,730 (74.4) 3,119 (71.8) 611 (91.5) <0.001
Age (y) 42.3±7.8 41.5±7.5 47.9±7.5 <0.001
Glucose (mg/dL) 92.0±18.3 90.7±15.6 100.6±28.8 <0.001
HbA1c (%) 5.6±0.7 5.5±0.6 5.9±1.1 <0.001
Log insulin 0.8±0.2 0.8±0.2 0.8±0.2 0.004
Total cholesterol (mg/dL) 199.0±34.9 198.2±34.2 204.5±38.7 <0.001
LDL cholesterol (mg/dL) 128.3±32.5 127.6±31.8 133.1±36.5 <0.001
HDL cholesterol (mg/dL) 56.2±14.0 56.7±14.0 53.0±13.7 <0.001
Log triglyceride 2.0±0.2 2.0±0.2 2.1±0.2 <0.001
Log hs-CRP 0.3±0.2 0.3±0.2 0.3±0.2 0.276
Creatinine (mg/dL) 0.9±0.2 0.9±0.2 1.0±0.2 <0.001
Uric acid (mg/dL) 5.6±1.5 5.5±1.5 5.9±1.3 <0.001
Waist circumference (cm) 83.7±8.1 83.4±8.1 86.0±8.0 <0.001
Body mass index (kg/m2) 24.2±3.1 24.0±3.1 25.2±3.1 <0.001
Systolic BP (mmHg) 119.0±11.3 118.4±11.1 123.1±11.9 <0.001
Diastolic BP (mmHg) 72.0±9.3 71.6±9.1 74.9±10.0 <0.001
Diabetes mellitus 199 (4.5) 124 (2.9) 75 (11.2) <0.001
Hypertension 701 (15.9) 472 (10.9) 229 (34.3) <0.001
Current smoker 1,617 (38.8) 1,357 (31.2) 260 (38.9) 0.006
Regular exercise ( ≥3 time/wk) 1,988 (39.6) 1,700 (39.1) 288 (43.1) 0.049
CACS 11.5±88.7
Log (CACS+1) 0.2±0.5 0 1.3±0.8 <0.001
Values are presented as number (%) or mean±standard deviation. P-values were calculated using the independent t-test and chi-square test.
CACS, coronary artery calcium score; LDL, low-density lipoprotein; HDL, high-density lipoprotein; hS-CRP, high sensitive C-reactive protein; BP, blood pressure.
Table 2. Pearson correlation coefficients between uric acid and clinical variables before and after adjustment for age and sex
Variable Uric acid Total-C Log TG Log hs-CRP WC Log (CACS+1)
γ P-value γ P-value γ P-value γ P-value γ P-value γ P-value
Uric acid - - 0.18 <0.001 0.34 <0.001 0.11 <0.001 0.39 <0.001 0.08 <0.001
Total-C 0.16* <0.001 - - 0.32 <0.001 -0.01 0.453 0.2 <0.001 0.05 <0.001
Log TG 0.21* <0.001 0.31* <0.001 - - 0.07 <0.001 0.43 <0.001 0.11 <0.001
Log hs-CRP 0.11* <0.001 -0.02* 0.151 0.07* <0.001 - - 0.19 <0.001 0.02 0.282
WC 0.27* <0.001 0.18* <0.001 0.37* <0.001 0.18* <0.001 - - 0.09 <0.001
Log (CACS+1) 0.04* 0.01 0.04* 0.029 0.05* 0.002 0.03* 0.09 0.08* <0.001 - -
Coefficients and P-values were calculated using Pearson's correlation analysis.
Total-C, total cholesterol; TG, triglyceride; hs-CRP, high sensitive C-reactive protein; WC, waist circumference; CACS, coronary artery calcium score.
*Correlations below the diagonal are adjusted for age and sex.
Na-Young Choi, et al. Serum Uric Acid Level and Coronary Artery Calcium Score
Korean Journal of Family Practice
KJFP
mg/dL, 석회화군에서 5.94 mg/dL로 석회화군에서 통계적으로 유의 하게 높은 수치를 보였다(P<0.001).
비석회화군에 비해 석회화군에서 평균 연령이 47.9세로 유의하게 높았으며 공복혈당과 당화혈색소도 유의하게 높은 평균값을 보였 다. 총콜레스테롤, LDL-C, Log TG의 평균은 석회화군에서 유의하게 높은 수치를 보였으며 HDL-C의 평균은 유의하게 낮은 수치를 보였 다. 그리고 허리둘레, 체질량지수의 평균은 석회화군에서 유의하게 높은 수치를 보였으며 수축기 혈압과 이완기 혈압 모두 석회화군에 서 유의하게 높은 수치를 보였다.
2. 혈중 요산의 위험요인 분석(Table 2)
혈중 요산은 전통적인 심혈관질환 위험인자인 총콜레스테롤 (γ=0.18, P<0.001), TG (γ=0.34, P<0.001), 허리둘레(γ=0.39, P<0.001)와 유 의한 양의 상관관계를 보였다. 또한 염증의 지표이며 심혈관질환 예 측인자인 hs-CRP (γ=0.11, P<0.001)와도 유의한 양의 상관관계를 보였 으며 CACS (γ=0.08, P<0.001)와도 유의한 양의 상관관계를 보였다. 가 장 영향력이 많은 연령과 성별을 보정한 후에도 결과는 동일하였다.
3. 관상동맥석회화 점수의 위험요인 분석(Table 3)
관상동맥석회화와 통계적으로 유의한 관련성이 있는 위험인자 를 확인하기 위해 로지스틱 회귀분석을 시행하였다. 비석회화군과 석회화군 간의 단변량 회귀분석 후 유의한 결과를 나타낸 성별, 연 령, 공복혈당, 당화혈색소, 총콜레스테롤, Log TG, 혈중 크레아티닌, 혈중 요산, 체질량지수, 수축기 혈압, 이완기 혈압, 당뇨, 고혈압, 흡연,
운동을 위험요인으로 설정하고 다변량 회귀분석을 하였다.
남성이 여성보다 관상동맥석회화 위험이 3.231배(95% confidence interval [CI], 2.030–5.143) 높았고, 연령이 증가할수록 석회화 위험이 1.121배(95% CI, 1.103–1.138) 유의하게 높았다. 공복혈당과 당화혈색 소의 상승은 석회화 위험이 높았지만 유의하지는 않았다. 총콜레스 테롤의 상승은 odds ratio (OR) 1.003 (95% CI 1.000–1.006), 체질량지수 의 증가는 OR 1.052 (95% CI, 1.012–1.092)로 CAC의 유의한 위험인자 였다. 혈중 요산의 상승은 OR 1.107 (95% CI, 1.012–1.210)로 CAC의 유 의한 위험인자였다. 수축기혈압과 이완기혈압은 상승할수록 석회화 위험이 높았으나 유의하지는 않았다. 고혈압의 빈도는 높을수록 석 회화 위험이 2.301배(95% CI 1.801–2.940) 유의하게 높았고 당뇨의 빈 도는 높을수록 석회화 위험이 높았으나 유의하지는 않았다. 흡연과 운동은 CAC와 유의한 상관성을 보이지 않았다.
고 찰
본 연구에서 혈중 요산 농도는 심혈관질환 위험인자인 총콜레스 테롤, TG, 허리둘레, hs-CRP와 통계적으로 유의한 관련이 있는 것으 로 나타났다. 이러한 결과는 나이와 성별을 보정한 후에도 여전히 의 미 있는 것으로 나타났다. 또한 CAC로 측정된 무증상의 동맥경화와 혈중 요산 간의 독립적인 연관성을 확인하였다. 국내 연구에서도 Kim 등16)이 혈중 요산 농도와 CACS와의 연관성에 대해 보고하였으 나 CACS가 11 이상인 경우에만 그 연관성이 입증되어 일반화시키기 에 한계가 있다. 하지만 본 연구에서는 비석회화군과 석회화군 모두 를 포함하여서도 혈중 요산과 CACS 간의 독립적인 연관성을 보여주 었다는 데에 의의가 있다.
과거에 혈중 요산 농도의 증가는 요산 결정이 관절에 침착되어 염 증반응을 유발하는 통풍의 원인으로만 간주되었으나, 통풍을 진단 받은 환자에서 다양한 형태의 신장질환이 동반된다는 보고 이후 다 른 장기에서의 혈중 요산의 역할에 대한 관심이 증가되었다.1) 또한 혈중 요산이 심혈관질환의 위험인자인가에 대한 여러 연구들이 발 표되면서 혈중 요산이 심혈관질환의 발생에 어떠한 영향을 미치는 지에 대한 관심도 증가되었다. 혈중 요산에 의한 혈관질환 발생의 주 요기전은 혈관내피세포 기능 부전일 것으로 추정된다.17) 요산에 의 한 산화질소(nitric oxide) 생성의 감소는 혈관 저항성을 증가시키고, 혈관 확장을 억제하며 국소염증 반응을 유도하고 국소 renin-angio- tensin system 활성화를 유도하여 직접적으로 혈관내피세포의 생존 을 억제하는 것으로 보고된 바 있다.17,18) 쥐를 이용한 동물 연구에서 혈관내피세포 산화질소 생성(endothelial nitric oxide synthese)의 장애 는 심혈관질환 위험인자들의 집합인 대사증후군과 관련이 있다는 Table 3. Multivariable logistic regression analysis of predictors of coro-
nary artery calcium score
Variable Odds ratio 95% confidence interval P-value
Male 3.231 2.030–5.143 <0.001
Age 1.121 1.103–1.138 <0.001
Glucose 1.002 0.994–1.011 0.585
HbA1c 1.103 0.867–1.403 0.424
Total cholesterol 1.003 1.000–1.006 0.043
Log triglyceride 1.141 0.689–1.888 0.424
Creatinine 0.425 0.180–1.004 0.051
Uric acid 1.107 1.012–1.210 0.026
Body mass index 1.052 1.012–1.092 0.009
Systolic BP 1.007 0.992–1.021 0.351
Diastolic BP 1.007 0.990–1.024 0.430
Diabetes mellitus 1.461 0.891–2.396 0.133
Hypertension 2.301 1.801–2.940 <0.001
Smoking 1.151 0.921–1.437 0.216
Exercise 1.054 0.853–1.302 0.629
Odds ratios and P-values were calculated using logistic regression.
BP, blood pressure.
최나영 외. 혈중 요산농도와 관상동맥석회화점수 Korean Journal of Family Practice
KJFP
것을 보여주었다.19)
국내에서 혈중 요산과 대사증후군의 관련성에 대한 여러 연구가 발표되었는데 Kim 등20)은 혈중 요산 농도의 증가는 체질량지수, 수 축기 혈압, 이완기 혈압, 공복 인슐린, TG와 유의한 양의 상관관계가 있으며 고밀도 콜레스테롤은 유의한 음의 상관관계가 있음을 보여 주었다. 그 후 Lim 등21)의 연구에서도 복부비만이 혈중 요산 농도의 증가와 유의한 관련성이 있음을 보여주었고 노인을 대상으로 진행 한 국내 연구에서 혈중 요산농도와 허리 둘레, TG, 공복 혈당의 양의 상관관계 및 고밀도 콜레스테롤의 음의 상관관계를 보여주었다.22) 본 연구에서는 혈중 요산과 총콜레스테롤, TG, 허리둘레와 의미 있 는 양의 상관관계를 보여주었고, 염증의 지표이며 심혈관질환 발생 의 예측인자인 hs-CRP와도 유의한 관련성을 보여주었다.
CACS는 향후 관상동맥 질환의 발생률과 관련이 있으며 이는 심 혈관질환의 단기간의 예측인자로서 혈청 지질 등의 어떤 위험인자 보다 우수하다고 알려져 있다.23) Krishnan 등24)이 Coronary Artery Risk Development In Young Adults (CARDIA) 연구에서 2,498명의 건 강한 성인들을 대상으로 분석하였을 때 혈중 요산 농도가 CACS와 양의 상관관계를 보이고 있었다. 이들의 분석에 의하면 혈중 요산이 1단위 증가할 때, Agatston score는 22% 증가하고 있었다(P=0.008).
1,107명을 대상으로 한 Coutinho 등12)의 연구에서도 혈중 요산은 CACS와 유의한 연관성을 보이고 있었는데, 이들의 연구는 수축기 혈압, 당뇨, 총콜레스테롤, HDL-C, 흡연, 체질량지수 등을 보정하지 않은 상태에서의 결과였다. 본 연구에서는 혈중 요산이 CACS에 독 립적으로 영향을 미치는 위험인자라는 것을 확인하였다. 이는 무증 상의 성인에서 혈중 요산이 죽상동맥경화증의 발생 및 진행 위험을 높인다는 것을 설명하는 근거가 될 수 있겠다.
본 연구의 제한점은 첫째, 단면연구로서 혈중 요산과 CAC 간의 인 과관계는 알 수 없으며 죽상동맥경화증이 진행되는 과정에서 혈중 요산의 역할을 분명히 하기 위해서는 전향적 연구가 필요할 것이다.
둘째, 연구대상자들이 삼성창원병원에서 건강검진을 받은 사람들 중 64절편 MDCT 스캐너로 CACS를 측정한 수검자들만을 대상으 로 하였기 때문에 결과의 대표성에 한계가 있으며 일반화하기 어렵 다. 셋째, 약물복용 여부는 설문조사를 통해 얻은 정보로써 객관적 인 확인이 불가능하며, 혈중 요산 농도에 영향을 미칠 수 있는 특정 약제의 복용 여부를 자세히 알 수 없다. 넷째, 심혈관질환 및 혈중 요 산 농도에 영향을 미칠 수 있는 음주력에 대한 조사가 이루어지지 못하여 연구에 포함되지 않았다.
이번 연구를 통해 혈중 요산 농도가 심혈관질환 위험인자 및 CACS와 독립적으로 양의 관련성이 있음을 알 수 있었다. 혈중 요산 농도의 증가가 심혈관질환과 관련이 있다는 연구결과들이 축적되
면서 요산과 심혈관질환의 단순한 연관이 아니라 일차진료 현장에 서 무증상 고요산혈증을 포함한 혈중 요산 농도 증가의 임상적 의의 와 치료의 가이드라인 확립에 기여할 수 있을 것으로 기대된다. 하지 만 이에 대한 생화학적인 기전 및 병태생리를 규명할 수 있도록 보다 진전된 설계의 후속연구가 더 필요할 것으로 사료된다.
요 약
연구배경:
혈중 요산 농도와 심혈관질환의 위험인자 및 관상동맥석 회화의 상관관계를 밝히기 위한 연구들이 많지만 아직 논란이 많은 상태이다. 이에 본 연구는 건강증진센터를 방문한 성인들을 대상으 로 혈중 요산 농도와 심혈관질환의 위험인자 및 관상동맥석회화 점 수와의 상관관계를 분석하였다.방법:
2013년 1월부터 2013년 12월까지 12개월 동안 건강진단을 목적 으로 삼성창원병원 건강증진센터에 내원한 성인 중 혈중 요산과 관 상동맥석회화 점수를 측정한 사람들을 대상으로 하였다. 관상동맥 석회화 점수 0을 기준으로 0인 그룹을 비석회화군, 0 초과인 그룹을 석회화군으로 나누어 두 군간의 일반적인 특성들의 차이점을 t-검 정, 카이제곱검정을 사용하여 분석하였다. 혈중 요산 농도와 심혈관 질환 위험인자들 간의 연관성을 보기 위해 Pearson 상관계수를 구하 였다. 관상동맥석회화에 대한 혈중 요산 농도의 교차비를 분석하기 위해 로지스틱 회귀분석을 시행하였다.결과:
혈중 요산은 전통적인 심혈관질환 위험인자인 총콜레스테롤, 중성지방, 허리둘레와 유의한 양의 상관관계를 보였다. 염증의 지표 이며 심혈관질환 예측인자인 고감도 C 반응성 단백질과도 유의한 양의 상관관계를 보였으며 관상동맥석회화 점수와도 유의한 양의 상관관계를 보였다. 가장 영향력이 많은 연령과 성별을 보정한 후에 도 결과는 동일하였다. 또한 혈중 요산의 상승은 교차비가 1.107로 관상동맥석회화의 유의한 위험인자였다(95% confidence interval, 1.012–1.210).결론:
혈중 요산 농도는 심혈관질환 위험인자 및 관상동맥석회화 점수와 독립적으로 양의 관련성이 있다.중심단어:
혈중 요산 농도; 심혈관질환 위험인자; 관상동맥석회화 점수; 무증상 죽상동맥경화증REFERENCES
1. Kang DH. Does hyperuricemia play a causative role in the development and/or aggravation of renal, cardiovascular and metabolic disease? Korean J Med 2011; 80: 524-8.
Na-Young Choi, et al. Serum Uric Acid Level and Coronary Artery Calcium Score
Korean Journal of Family Practice
KJFP
2. Gertler MM, Garn SM, Levine SA. Serum uric acid in relation to age and physique in health and in coronary heart disease. Ann Intern Med 1951;
34:1421-31.
3. Fang J, Alderman MH. Serum uric acid and cardiovascular mortalitiy the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey. JAMA 2000; 283: 2404-10.
4. Alderman MH, Cohen H, Madhavan S, Kivlighn S. Serum uric acid and cardiovascular events in successfully treated hypertensive patients. Hyper- tension 1999; 34: 144-50.
5. Culleton BF, Larson MG, Kannel WB, Levy D. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann Intern Med 1999; 131: 7-13.
6. Moriarity JT, Folsom AR, Iribarren C, Nieto FJ, Rosamond WD. Serum uric acid and risk of coronary heart disease: Atherosclerosis Risk in Communities(ARIC) study. Ann Epidemiol 2000; 10: 136-43.
7. Anderson KM, Odell PM, Wilson PW, Kannel WB. Cardiovascular disease risk profiles. Am Heart J 1991; 121: 293-8.
8. De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dal- longeville J, et al. European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice. Eur J Cardiovasc Prev Rehabil 2003; 10: S1-10.
9. LaMonte MJ, FitzGerald SJ, Church TS, Barlow CE, Radford NB, Levine BD, et al. Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women. Am J Epidemiol 2005; 162:
421-9.
10. Pletcher MJ, Tice JA, Pigonoe M, Browner WS. Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis. Arch Intern Med 2004; 164: 1285-92.
11. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, et al. ACCF/AHA 2007 clinical expert consensus document on coro- nary artery calcium scoring by computed tomography in global cardiovas- cular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Con- sensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2007; 49: 378-402.
12. Coutinho Tde A, Turner ST, Peyser PA, Bielak LF, Sheedy PF 2nd, Kullo IJ.
Associations of serum uric acid with markers of inflammation, metabolic syndrome, and subclinical coronary atherosclerosis. Am J Hypertens 2007;
20: 83-9.
13. Grossman C, Shemesh J, Koren-Morag N, Bornstein G, Ben-Zvi I, Gross- man E. Serum uric acid is associated with coronary artery calcification. J Clin Hypertens (Greenwich) 2014; 16: 424-8.
14. Neogi T, Terkeltaub R, Ellison RC, Hunt S, Zhang Y. Serum urate is not asso- ciated with coronary artery calcification: the NHLBI family heart study. J Rheumatol 2011; 38: 111-7.
15. Agatston AS, Janowitz WR, Hildmer EJ, Zusmer NR, Viamonte M Jr, Detra- no R. Quantitation of coronary artery calcium using ultrafast computed to- mography. J Am Coll Cardiol 1990; 15: 827-32.
16. Kim HY, Baek SH, Kim MJ, Park KS, Kim YS, Oh MJ, et al. Relationships be- tween serum uric acid level and coronary artery calcium score. Korean J Fam Pract 2015; 5: 198-203.
17. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med 2008; 359: 1811-21.
18. Kang DH, Park SK, Lee IK, Johnson RJ. Uric acid-induced C-reactive pro- tein expression: implication on cell proliferation and nitric oxide produc- tion of human vascular cells. J Am Soc Nephrol 2005; 16: 3553-62.
19. Cook S, Hugli O, Egli M, Vollenweider P, Burcelin R, Nicod P, et al. Cluster- ing of cardiovascular risk factors mimicking the human metabolic syn- drome X in eNOS null mice. Swiss Med Wkly 2003; 133: 360-3.
20. Kim SK, Park HA, Nam OY, Beck SH, Whang DH, Hwang UK, et al. Risk of the metabolic syndrome according to the level of the uric acid. Korean J Fam 2007; 28: 428-35.
21. Lim JH, Kim YK, Kim YS, Na SH, Rhee MY, Lee MM. Relationship between serum uric acid levels, metabolic syndrome, and arterial stiffness in Korean.
Korean Circ J 2010; 40: 314-20.
22. Oh JE, Cho CY. Relationship between serum uric acid level and metabolic syndrome in the elderly. Korean J Clin Geri 2011; 12: 176-82.
23. Detrano R, Hsiai T, Wang S, Puentes G, Fallavollita J, Shields P, et al. Prognos- tic value of coronary calcification and angiographic stenoses in patients un- dergoing coronary angiography. J Am Coll Cardiol 1996; 27: 285-90.
24. Krishnan E, Pandya BJ, Chung L, Dabbous O. Hyperuricemia and the risk for subclinical coronary atherosclerosis-data from a prospective observa- tional cohort study. Arthritis Res Ther 2011; 13: R66.