Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):599-603
KJFP
Korean Journal of Family PracticeOriginal Article
pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3, suppl. 2):PB-1
KJFP
Korean Journal of Family Practice서 론
고칼슘혈증은 암환자의 20 ~ 30 %에서 나타나는 흔한 합병증으로, 의식변화나 신부전 등으로 이어지는 심각한 전해질 이상이다.
1)다발 성 골수종이나 폐암, 유방암, 두경부암에서 빈번하게 발생한다고 보 고되며,
2-4)특히 말기 암환자에서 발생하는 고칼슘혈증은 예후가 매 우 나쁜 것으로 알려져 있다.
5)기존의 한 연구에 따르면 암환자 중 고칼슘혈증이 나타난 환자의 50 %가 30 일 이내 사망한 것으로 보고 되었다.
6)완화의학과 환자 259 명 대상의 연구에서도 칼슘 농도 증가 에 따라 재원 환자의 사망률이 유의하게 높아지는 결과를 제시한 바 있다.
7)이처럼 말기 암환자에서도 여명 예측 인자로서의 고칼슘혈증 에 대한 관심을 가질 필요가 있으나 아직 그에 대한 연구는 미비한
실정이다. 이에 본 연구에서는 국내 호스피스 병동에 입원한 말기 암 환자를 대상으로 혈청 칼슘 농도와 생존기간 사이의 연관성을 분석 하여 말기 암환자에서 고칼슘혈증이 여명 예측에 미치는 영향에 대 해 알아보고자 한다.
방 법
1. 연구 대상과 방법
본 연구는 후향적 관찰연구로 2010 년 1 월부터 2012 년 12 월까지 서울 소재 대학병원 호스피스센터에 입원한 말기 암환자들의 전자 의무 기록을 이용하였다. 의무기록을 통해 환자의 나이, 성별, 암의 종류, 전이 유무, 생존 기간, 완화 수행 지수( Palliative performance
말기암환자에서의 고칼슘혈증과 예후와의 연관성
신은경, 김철민
*, 이용주, 윤조히, 정하지, 윤현수, 최나은, 이글라라
가톨릭대학교 의과대학 서울성모병원 가정의학교실
Association between blood calcium level and survival time in terminal cancer patients
Eun-Kyung Shin, Chul-Min Kim*, Yong-Joo Lee, Jo-Hi Yoon, Ha-Ji Jung, Hyun-Soo Yoon, Na-Eun Choi, Clara Lee.
Department of Family Medicine, Seoul St. Mary’s Hospital, College of medicine, The Catholic University of Korea
Background: Hypercalcemia is a common cancer-related complication, and is associated with shorter survival time than patients with normocalcemia. However, hypercalcemia’s role as a
prognostic factor in terminal cancer patients is poorly understood. Therefore, we investigated whether hypercalcemia might be a valuable predictor for survival time in terminal cancer patient.Methods: We reviewed electronic medical records of hospitalized terminal cancer patients who had serum calcium levels measured between January 2010 and December 2012 in a
palliative care unit of a tertiary hospital . Hypercalcemia was defined as a corrected serum calcium≥10mg/dl. Univariate and multivariate Cox regression analyses were performed to determine factors affecting survival time.Results: Among 552 patients, 72(13%) were hypercalcemic. Multivariate analysis showed that serum CRP, PPS, sodium levels and hypercalcemia were significantly associated with survival
time; hazard ratio was 1.12(95% CI, 1.02~1.22; p=0.003), 0.70(95% CI, 0.64~0.76; p<0.001), 0.84(95% CI, 0.77~0.93; p=0.001), and 1.78(95% CI, 1.37~2.31; p<0.001), respectively.The Kaplan-Meier curve showed that patients with hypercalcemia had shorter length of survival time compared to patients with serum calcium<10mg/dl (Log rank test <0.001).
Conclusion: In terminal cancer patients, hypercalcemia is an independent prognostic factor. In the future, more prospective trials are needed in order to examine the clinical benefit of
early intervention for hypercalcemia.Keywords: cancer, palliative care, hypercalcemia, prognosis
Received February.28, 2015 Revised August 31, 2015 Accepted September 22, 2015 Corresponding Author Chul-Min Kim
Tel: +82-2-2258-2894, Fax: +82-2-2258-2907 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Eun-Kyung Shin, et al. Association between blood calcium level and survival time in terminal cancer patients
Korean Journal of Family Practice
KJFP
scale , PPS ), 혈액 검사 결과를 수집하였다.
그 중 혈액검사 상 칼슘, 알부민, 크레아티닌, C -반응 단백 ( C - reactive protein , CRP ), 나트륨, 칼륨 검사 결과가 있는 환자, 그리고 사망일이 확인된 환자만을 연구대상으로 하였다. 입원 당시 의 혈액검사 결과를 알 수 없거나 정확한 사망일이 기록되지 않은 환자는 제외하여, 연구 기간 중 입원한 총 1053 명의 환자 중 552 명 의 환자가 최종 분석에 포함되었다.
혈액검사 결과는 호스피스 병동에 첫 입원하여 1 주일 이내 에 시행한 혈액검사 결과값을 기록하였으며, 환자의 생존기간 은 호스피스센터에 처음 입원한 날부터 임종할 때까지의 기간으 로 정의하였다. 고칼슘혈증의 정의는 혈중 교정 칼슘( Corrected Calcium ) 10mg / dl 이상인 경우로 하였으며 교정혈중칼슘은 혈중 칼슘 + 0 . 8 × ( 4 -혈중 알부민) 의 수식으로 계산하였다.
연구는 서울 성모병원의 의료윤리위원회( institutional review board )의 승인을 받았다. ( IRB No : KC14RIS10879 )
2. 통계 분석
기술통계를 이용하여 연구 대상자의 성별, 암의 종류, 전이 유 무, 동반질환을 분석하였으며 나이, PPS , 혈중 칼슘, 나트륨, 칼 륨, 크레아티닌, CRP 는 평균 값으로, 평균 생존기간은 중간값으로 표시하였다. 혈중칼슘농도와 연관성이 높은 변수들은 Spearman ’ s correlation 을 이용하여 분석하였고, 단변량( univariate )과 다변량 생존분석( multivariate Cox regression analysis )을 이용하여 각 변수 들이 생존기간에 미치는 위험도( Hazard Ratio , HR )을 분석하였다.
또한 Kaplan - Meier 생존 분석을 이용하여 고칼슘혈증 환자군과 비고칼슘혈증 환자군의 생존곡선을 비교하였다. 통계 분석은 SAS Statistical Package Release 9 . 3 ( SAS Institute , Cary , NC )을 사용하 였으며, P
<0 . 05 인 경우 통계적으로 유의성이 있는 것으로 정의하 였다.
결 과
1. 대상환자들의 일반적인 특징
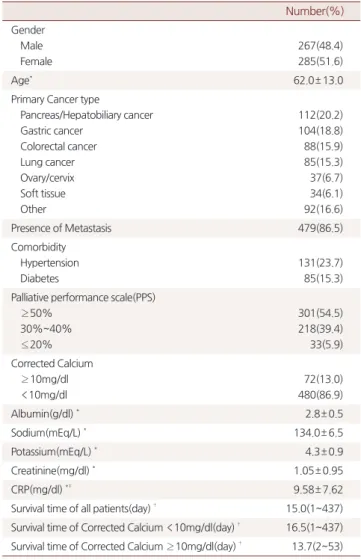
총 552 명의 환자 중 남자 267 명 ( 48 . 4 %), 여자 285 명 ( 51 . 6 %) 이 었고, 평균 연령은 62 . 0 (± 13 . 0 ) 세였다. 대상자 평균 연령은 62 . 0 세였다. 원발 암 병소는 간담췌암이 112 명( 20 . 2 %)로 가장 많았으 며, 그 뒤로 위암, 대장암, 폐암, 자궁/난소암 순이었다. PPS 50 % 이상인 환자가 301 명( 54 . 5 %), PPS 20 % 이하는 33 명( 5 . 9 %) 이었다.
고칼슘혈증( corrected Ca ≥ 10mg / dl )인 환자는 72 명으로 전체 대 상자의 13 %를 차지하였다. 전체 연구 대상자 생존기간 중앙값은 15 . 0 일 이었다 ( Table 1 ).
2. 생존 기간과 혈중칼슘농도간의 상관관계
Table 2 와 같이 환자들의 생존기간과 나이, CRP , 나트륨, 칼륨, 크레아티닌, PPS , 교정 칼슘 수치와의 상관관계를 분석하였다. 그 중 CRP , 크레아티닌, 교정 칼슘 수치가 통계적으로 유의하게 생존 기간과 음의 상관관계를 보였다 ( p
<0 . 001 ). 나트륨, PPS 은 생존기 간과의 양의 상관관계가 확인되었다. 나이, 칼륨 수치는 생존기간 과 통계적으로 유의한 상관관계를 보이지 않았다.
3. 단변량, 다변량 Cox 비례위험모형을 이용한 생존분석
단변량과 다변량 Cox 비례위험모형을 통해 생존기간에 영향을 미치는 변수의 사망할 위험도( Hazard Ratio , HR )를 구하였다. 관련 변수는 앞서 상관관계에서 유의한 결과를 보인 변수를 선택하였다.
각 변수를 보정한 다변량 분석 결과, 교정 칼슘과 CRP 의 위험도는 각각 1 . 15 ( 95 % CI , 1 . 07 ~ 1 . 23 ), 1 . 16 ( 95 % CI , 1 . 07 ~ 1 . 25 )으로, 통 계적으로 유의하게 생존기간과의 연관성을 보였다 ( p
<0 . 001 ). 반
Table 1. General characteristics of study population
Number(%) Gender
Male Female
267(48.4) 285(51.6)
Age* 62.0± 13.0
Primary Cancer type
Pancreas/Hepatobiliary cancer Gastric cancer
Colorectal cancer Lung cancer Ovary/cervix Soft tissue Other
112(20.2) 104(18.8) 88(15.9) 85(15.3) 37(6.7) 34(6.1) 92(16.6)
Presence of Metastasis 479(86.5)
Comorbidity Hypertension Diabetes
131(23.7) 85(15.3) Palliative performance scale(PPS)
≥ 50%
30%~40%
≤ 20%
301(54.5) 218(39.4) 33(5.9) Corrected Calcium
≥ 10mg/dl
<10mg/dl
72(13.0) 480(86.9)
Albumin(g/dl) * 2.8± 0.5
Sodium(mEq/L) * 134.0± 6.5
Potassium(mEq/L) * 4.3± 0.9
Creatinine(mg/dl) * 1.05± 0.95
CRP(mg/dl) *‡ 9.58± 7.62
Survival time of all patients(day) † 15.0(1~437) Survival time of Corrected Calcium <10mg/dl(day) † 16.5(1~437) Survival time of Corrected Calcium ≥ 10mg/dl(day) † 13.7(2~53)
* mean(±SD)
† median(Q1,Q3)
‡ CRP: C-reactive protein
신은경 외. 말기암환자에서의 고칼슘혈증과 예후와의 연관성 Korean Journal of Family Practice
KJFP
면 PPS 와 혈중 나트륨 농도의 위험도는 각각 0 . 71 ( 95 % CI , 0 . 65 - 0 . 78 ; p
<0 . 001 ), 0 . 88 ( 95 % CI , 0 . 88 ; p = 0 . 011 )으로, 높을수록 위험 도가 감소하였다( Table 3 ).
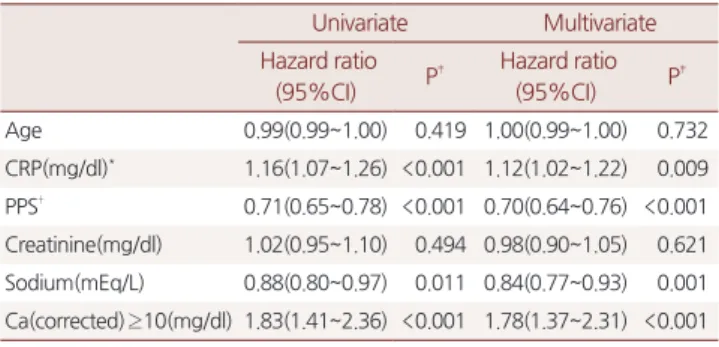
Table 4 에서는 Cox 비례위험모형에서 연속변수였던 교정 칼슘
농도 10mg / dl 이상인 고칼슘혈증 환자군의 위험도를 구하였다. 다 른 변수를 보정한 후, 고칼슘혈증의 위험도는 1 . 78 으로, 생존기간과 의 통계적으로 연관관계를 보였다( 95 % CI , 1 . 37 ~ 2 . 31 ; p
<0 . 001 ).
Figure 1 은 Kaplan - Meier 생존분석을 통해 교정 칼슘수치 10 이 상의 고칼슘혈증 환자군과 비고칼슘혈증 환자군 간의 생존기간을 비교하였다. 고칼슘혈증이 통계적으로 유의하게 더 짧은 생존기간 을 보였다( Log rank test
<0 . 001 ).
고 찰
본 연구는 말기암 환자의 혈중 칼슘 농도와 생존기간이 통계적으 로 유의한 상관관계가 있으며, 고칼슘혈증이 말기 암환자에서 독립 적 예후 예측인자임이 확인되었다. 또한 고칼슘혈증 외에도 CRP , PPS , 혈중 나트륨 농도가 생존기간과 각각 독립적인 연관성을 가지 는 것으로 확인할 수 있었다. Zhang 등
8)의 연구에서도 암 진단 후 140 일 이상 고칼슘혈증을 보인 그룹이 비칼슘혈증 환자 그룹에 비 해 사망률이 높은 결과를 보인 바 있다.
환자에서 호발하는 고칼슘혈증을 설명하는 데는 몇 가지 기전이 알려져 있다.
9)뼈 전이로 인한 국소 골용해에 의해 혈중 칼슘농도 가 높아지는 경우는,
10)말기 암에서 고칼슘혈증을 일으키는 원인의 20 % 정도를 차지하며 골수 내 악성 세포 주변에 파골세포성 뼈 흡 수가 증가하여 발생하게 된다.
11)뼈 전이가 잘 되는 암종으로는 유 방암, 전립선암, 다발성 골수종, 임파종 등 있다.
12)뼈 전이는 고칼 슘혈증 이외에도 병적 골절이나 척수 압박 등을 일으켜 입원률 증 가 등의 질병 부담을 일으키는 심각한 합병증을 초래하는 것으로 알 려져 있다.
13)한편, 말기 암인 고칼슘혈증 환자의 80 % 정도는 원발 성 종양으로부터 발생한 부갑상선 관련 단백( parathyroid hormone
Table 2. Correlations between survival time and serum corrected calcium level over 10mg/dl, age, PPS, sodium, potassium, creatinine, and CRP.
Variables Correlation coefficient P‡
Age 0.069 0.104
CRP(mg/dl)* - 0.157 <0.001
Sodium(mEq/L) 0.105 0.013
Potassium(mEq/L) - 0.001 0.980
Creatinine(mg/dl) - 0.115 0.007
PPS† 0.358 <0.001
Calcium(Corrected)(mg/dl) - 0.186 <0.001
*CRP: C-reactive protein
†PPS: palliative performance scale on first admission
‡ P value were derived from Spearman’s correlation analysis
PPS, Sodium, Potassium, Creatinine, CRP, and Calcium level were standardized.
Standardized scale=(raw scale average) / standard deviation
Table 3. Univariate and multivariate Cox proportional hazard ratios of survival
Univariate Multivariate Hazard ratio
(95%CI) P‡ Hazard ratio
(95%CI) P‡
Age 0.99(0.99~1.00) 0.419 1.00(0.99~1.00) 0.580
CRP(mg/dl)* 1.16(1.07~1.26) <0.001 1.14(1.04~1.24) 0.003 PPS† 0.71(0.65~0.78) <0.001 0.70(0.64~0.76) <0.001 Creatinine(mg/dl) 1.02(0.95~1.10) 0.494 0.97(0.90~1.05) 0.476 Sodium(mEq/L) 0.88(0.80~0.97) 0.011 0.85(0.77~0.93) 0.001 Ca(corrected)(mg/dl) 1.15(1.07~1.23) <0.001 1.15(1.07~1.23) <0.001
* CRP: C-reactive protein
† PPS: palliative performance scale on first admission
‡ P value was derived according to the Cox proportional hazard model.
CRP, PPS, Creatinine, and Sodium level were standardized. Standardized scale=(raw scale average)/standard deviation
Table 4. Univariate and multivariate Cox proportional hazard ratios of survival
Univariate Multivariate Hazard ratio
(95%CI) P‡ Hazard ratio
(95%CI) P‡
Age 0.99(0.99~1.00) 0.419 1.00(0.99~1.00) 0.732
CRP(mg/dl)* 1.16(1.07~1.26) <0.001 1.12(1.02~1.22) 0.009 PPS† 0.71(0.65~0.78) <0.001 0.70(0.64~0.76) <0.001 Creatinine(mg/dl) 1.02(0.95~1.10) 0.494 0.98(0.90~1.05) 0.621 Sodium(mEq/L) 0.88(0.80~0.97) 0.011 0.84(0.77~0.93) 0.001 Ca(corrected) ≥10(mg/dl) 1.83(1.41~2.36) <0.001 1.78(1.37~2.31) <0.001
* CRP: C-reactive protein
† PPS: palliative performance scale on first admission
‡ P value was derived according to the Cox proportional hazard model.
CRP, PPS, Creatinine, and Sodium level were standardized. Standardized scale=(raw scale average)/standard deviation
Figure 1. Differences in survival time categorized by groups of Ca level.
P values were derived according to the log-rank test
P value < 0.001
Eun-Kyung Shin, et al. Association between blood calcium level and survival time in terminal cancer patients
Korean Journal of Family Practice
KJFP
related protein , PTHrP )이 receptor activator of nuclear factor kappa ligand ( RANKL ) 과 파골세포 전구체가 분비되도록 파골세 포를 자극하여 발생하는데,
14)주로 두경부암, 식도암, 자궁경부암 및 폐암, 신세포암, 난소암 등의 암종에서 관찰된다.
15, 16)또한 소세 포성폐암이나 난소암, 췌장암 등에서 이소성 PTH 분비를 통해 고 칼슘혈증을 일으키는 기전도 보고된 바 있다.
17)암과 관련된 고칼슘혈증은, 흔하지만 치명적인 대사성 합병증으 로 특이적인 증상을 보이지 않기 때문에, 적절한 진단과 이에 대한 치료가 지연되는 경우가 많다.
18)고칼슘혈증은 치료는 pamidronate 나 zoledronic acid 와 같은 bisphosphonates 와 Calcitonin 투여와 수액치료 및 이뇨제 투여가 주를 이룬다.
19, 20)최근에는 Denosumab 이 골흡수 매개 RANKL 과 결합하여 이전에 bisphosphonate 치료 로 조절되지 않는 불응성 고칼슘혈증 환자에서도 효과가 있는 것으 로 발표되고 있다.
21, 22)Qu 등
5)의 연구에서 175 명의 간세포암 환자 에서 paraneoplastic syndrome 여부에 따른 생존기간을 비교하였 다. 이 연구에 따르면 고칼슘혈증을 가진 경우 그렇지 않은 환자에 비해 통계적으로 유의하게 짧은 생존기간을 보였다. 또한 두경부암 대상 연구에서 고칼슘혈증 환자가 그렇지 않은 두경부암 환자와 비 교하여, 마지막 생애 3 개월 동안 병원 재원기간이 더 길고 응급실을 방문하는 경우가 더 많은 것을 확인할 수 있었다.
23)본 연구의 강점은 고칼슘혈증이 말기암 환자의 예후 예측인자가 된다는 첫 번째 연구라는 점이다. 또한 특정 암종 환자군이 아닌 다 양한 암종의 환자를 대상으로 2 년간 수집된 자료를 통해 얻어진 결 과이다. 또한 본 연구는 선행연구에서 독립적 예후예측 인자로 알 려진 PPS , CPR , 혈중 나트륨 역시 통계적으로 유의한 예후예측 인 자임이 확인되어 본 연구의 신뢰도를 더해주었다. 그러나 본 연구 에는 후향적 관찰연구였고, 단일기관에서만 수집된 정보를 바탕으 로 하였다는 한계가 있다. 또한 수액치료를 포함한 고칼슘혈증 교 정을 약물 사용 유무에 대한 자료가 수집되지 않았으며, 입원기간 중의 고칼슘혈증 교정 여부 또한 확인하지 않았다. 그리고, 말기 암 환자에서 환자의 생존률에 영향을 미칠 수 있는 모든 교란인자를 포 함하지 않아 결과에 영향을 주었을 수 있다. 향후 말기 또는 진행암 환자를 대상으로 하여 예후 예측 인자로서의 고나트륨혈증에 대한 다기관 전향적 연구가 필요하다. 또한 말기암환자의 고칼슘혈증의 교정이 예후에 미치는 영향에 대한 추가적인 연구도 시행되어야 할 것이다.
요 약
연구배경: 고칼슘혈증은 흔한 암 관련 합병증으로, 정상 칼슘혈증 에 비해 생존기간이 짧은 것으로 보고되고 있다. 그러나 말기 암환 자에서의 나쁜 예후인자로서 가능성에 대해서는 잘 알려져 있지 않
았다. 본 연구에서 고칼슘혈증이 말기환자의 생존기간에 대한 예측 인자로서의 가능성에 대해 알아보고자 한다.
방법: 2010 년 1 월부터 2012 년 12 월까지 일개 대학병원 호스피스센 터에 입원한 환자의 의무기록과 칼슘 수치를 조사하였다. 고칼슘혈 증은 교정 혈중 칼슘농도가 10mg / dl 이상인 경우로 정의하였다. 단 변량 및 다변량 Cox 회귀분석을 이용하여 고칼슘혈증을 포함하여 말기 암환자의 생존기간과 관련된 인자를 분석하였다.
결과: 총 552 명의 환자의 환자 중 72 명( 13 %)이 고칼슘혈증이었 다. 다변량분석에서 혈중 CRP , PPS ( Palliative performance scale ), 혈중 나트륨농도 및 고칼슘혈증의 위험비가 각각 1 . 12 ( 95 % CI , 1 . 02 ~ 1 . 22 ; p = 0 . 003 ), 0 . 70 ( 95 % CI , 0 . 64 ~ 0 . 76 ; p
<0 . 001 ), 0 . 84 ( 95 % CI , 0 . 77 ~ 0 . 93 ; p = 0 . 001 ), 1 . 78 ( 95 % CI , 1 . 37 ~ 2 . 31 ; p
<0 . 001 )이었다. 또한 Kaplan - Meier 생존분석에서 고칼슘혈증 환 자의 생존기간이 그렇지 않은 말기암환자의 생존기간보다 통계적 으로 유의하게 짧은 것으로 분석되었다( Log rank test
<0 . 001 ).
결론: 말기 암환자에서 고칼슘혈증은 독립적인 예후인자로 확인되 었으며, 향후 대규모의 전향적인 연구가 필요하다.
중심단어: 말기암, 완화의료, 고칼슘혈증, 예후
REFERENCES
1. John TP, Jr., Harald J. Harrison’s principles of internal medicine, 18th ed.: McGraw-Hill; 2012.
2. Djulbegovic B, Wheatley K, Ross J, Clark O, Bos G, Goldschmidt H, et al. Bisphosphonates in multiple myeloma. Cochrane Database Syst Rev. 2002;(3):CD003188
3. Kanaji N, Watanabe N, Kita N, Bandoh S, Tadokoro A, Ishii T, Dobashi H, Matsunaga T. Paraneoplastic syndromes associated with lung cancer. World J Clin Oncol. 2014 Aug 10;5(3):197-223.
4. Rizzoli R, Body JJ, Brandi ML, Cannata-Andia J, Chappard D, El Maghraoui A, et al.; International Osteoporosis Foundation Committee of Scientific Advisors Working Group on Cancer- Induced Bone Disease. Cancer-associated bone disease. Osteoporos Int. 2013 Dec;24(12):2929-53.
5. Qu Q1, Wang S, Chen S, Zhou L, Rui JA. Prognostic role and significance of paraneoplastic syndromes in hepatocellular carcinoma. Am Surg. 2014 Feb;80(2):191-6.
6. Ralston SH, Gallacher SJ, Patel U, Campbell J, Boyle IT. Cancer- associated hypercalcemia: morbidity and mortality. Clinical experience in 126 treated patients. Ann Intern Med. 1990 Apr 1;112(7):499-504.
7.VAlsirafy SA, Sroor MY, Al-Shahri MZ. Predictive impact of electrolyte abnormalities on the admission outcome and survival of
신은경 외. 말기암환자에서의 고칼슘혈증과 예후와의 연관성 Korean Journal of Family Practice
KJFP
palliative care cancer referrals. J Palliat Med. 2009 Feb;12(2):177-80.
8. Zhang SJ, Hu Y, Cao J, Qian HL, Jiao SC, Liu ZF, et al. Analysis on survival and prognostic factors for cancer patients with malignancy-associated hypercalcemia. Asian Pac J Cancer Prev.2014;14(11):6715-9.
9. Stewart AF. Clinical practice. Hypercalcemia associated with cancer.
N Engl J Med. 2005 Jan 27;352(4):373-9.
10. Roodman GD. Mechanisms of bone metastasis. N Engl J Med. 2004 Apr 15;350(16):1655-64.
11. Clines GA. Mechanisms and treatment of hypercalcemia of malignancy. Curr Opin Endocrinol Diabetes Obes. 2011 Dec;18(6):339-46.
12. Rordorf T, Hassan AA, Azim H, Alexandru E, Er O, Gokmen E, et al. Bone health in breast cancer patients: a comprehensive statement by CECOG/SAKK Intergroup. Breast. 2014 Oct;23(5):511-25.
13. Coleman R, Body JJ, Aapro M, Hadji P, Herrstedt J; ESMO Guidelines Working Group. Bone health in cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2014 Sep;25 Suppl 3:iii124-37.
14. Yasuda H. RANKL, a necessary chance for clinical application to osteoporosis and cancer-related bone diseases. World J Orthop.
2013 Oct 18;4(4):207-17.
15. Deans C, Wigmore S, Paterson-Brown S, Black J, Ross J, Fearon KC. Serum parathyroid hormone-related peptide is associated with systemic inflammation and adverse prognosis in gastroesophageal carcinoma. Cancer. 2005 May 1;103(9):1810-8.
16. Grzywacz A, Dziuk M, Niemczyk S. Refractory hypercalcemia
in patient with lung cancer. Pol Merkur Lekarski. 2014 Apr;36(214):261-4.
17. Skrabanek P, McPartlin J, Powell D. Tumor hypercalcemia and "ectopic hyperparathyroidism". Medicine (Baltimore). 1980 Jul;59(4):262-82.
18. Radványi I, Csikós A, Balogh S. The significance of early diagnosis of cancer-related hypercalcaemia. Orv Hetil. 2013 Sep 1;154(35):1367-73.
19. Major P, Lortholary A, Hon J, Abdi E, Mills G, Menssen HD, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol. 2001 Jan 15;19(2):558-67.
20. Binstock ML, Mundy GR. Effect of calcitonin and glutocorticoids in combination on the hypercalcemia of malignancy. Ann Intern Med.
1980 Aug;93(2):269-72.
21. Freeman A1, El-Amm J, Aragon-Ching JB. Use of denosumab for renal cell carcinoma-associated malignant hypercalcemia: a case report and review of the literature.Clin Genitourin Cancer. 2013 Dec;11(4):e24-6.
22. Hu MI, Glezerman I, Leboulleux S, Insogna K, Gucalp R, Misiorowski W, et al. Denosumab for patients with persistent or relapsed hypercalcemia of malignancy despite recent bisphosphonate treatment. J Natl Cancer Inst. 2013 Sep 18;105(18):1417-20.
23. Alsirafy SA, Sroor MY, Al-Shahri MZ. Hypercalcemia in advanced head and neck squamous cell carcinoma: prevalence and potential impact on palliative care. J Support Oncol. 2009 Sep- Oct;7(5):154-7.