Department of Oral & Maxillofacial Surgery, College of Dentistry, Chosun University
Abstract
Alveolar bone absorption after missing of tooth leads to problems when placing posterior maxillary implants. Because of sinus lifting, an unfavorable architecture of the maxillary sinus no longer contraindicates when implant placement.
Many investigators have examined the ways to improve bone quality and quantity and the success rates differ for different bone grafting materials. This study evaluated the success rate of implant after sinus grafting with allografts and xenografts. From 2000 to 2005, 120 endosseous implants were placed in 50 patients at Chosun University Dental Hospital using sinus lifting techniques. The survival rate for the 120 implants was 89.2% (107/120).
Clinical evaluation of graft materials in sinus grafting
Su-Gwan Kim, Seok-Jin Yang, Sun-young Oh, Seng-Byung Park, Chae-Su Lim, Kyeung-Ho Yun, Hak-Kyun Kim, Seong -Yong Moon, So-Young Kim
Clinical evaluation of graft materials in sinus grafting
김수관, 양석진, 오선영, 박승병, 임채수, 윤경호, 김학균, 문성용, 김소영 조선대학교 치과대학 구강악안면외과학교실
※“이 논문은 2007년도 재단법인 조선대학교 치과대학교육문화재단 특수목적기금의 지원을 받아 연구되었음”
I n implant placement, the lack of adequate bone height causes numerous problems. In the posterior maxilla, the bone loss on the buccolingual side and apical region that follows the loss of a tooth and pneumatization of the maxillary sinus floor make implantation difficult1-
3). In the past, the maxillary sinus floor was considered merely an unnecessary anatomical space that was of no help in bone proliferation.
However, this attitude has been overcome by various surgical techniques4). The methods used to regenerate an atrophied ridge include guided bone regeneration (GBR) followed by onlay or veneer bone transplant, Le Fort I osteotomy and bone transplantation, and maxillary sinus floor elevation and bone grafting. The last appears to be an excellent method promoting the long-term retention of implants5,6). There have been numerous reports about maxillary sinus floor elevation in terms of the anatomy, technical factors, clinical and histological results based on the clinical approach, and implant materials5). A maxillary sinus floor elevation technique for placing an implant in a recessed maxillary molar area was first introduced7), and reported in 19808). Wallace et al.9) reported that maxillary sinus floor elevation is one of the most general methods for increasing the vertical bone height for implantation in the maxillary molar area.
treatment, one- or two-stage implant placement, the contact surface between the grafted and autologous bone, the blood supply to the elevated flap, and the time since surgery10,11). This study evaluated maxillary floor elevation using various bone substitutes to determine the criteria for successful implant placement in the maxillary molar area.
Patients and methods
This study included 50 patients who underwent maxillary sinus floor elevation during implant placement in the maxillary molar area from 2000 to 2005. The patients were followed up for at least 2 years after completion of the prosthesis. There were 29 males and 21 females, with an overall mean age of 53.6 years. In total, 120 implants were placed.
A lateral approach was used for patients with more than 4 mm of residual alveolar bone. When the height of the residual alveolar bone was less than 4 mm, two-stage surgery was performed, while one-stage surgery was performed for the cases with 4-7 mm of residual alveolar bone.
Under local anesthesia, a full thickness flap was prepared to fit the window, and an oval window was created in the area 2~3 mm above the
Ⅱ
original article
maxillary sinus floor. The maxillary sinus membrane was dissected, and elevated. Graft material was placed in the subantral space on the mesial, inner, and lateral sides, the implants were placed, and any remaining space was filled.
Finally, the flap was sutured.
The used materials were as follows:
1. Xenograft (Bio-Oss�, BioCera�, or BBP�) 2. Allograft (Dembone�)
3. Xenograft plus Allograft
4. Allograft plus Xenograft (Cerasorb� + Bio- Oss�)
5. Xenograft mixed with autogenous bone from the chin in 1:1 ratio.
The implants used in accordance with the manufacturer included 30 fixtures of Frialit-2, 25 Xive, 25 Avana, 19 of Bicon, 14 of 3i, and 7 of others. The most frequently used diameters were 4.5 (57 implants) and 4.0 mm (46 implants), and the most frequently used lengths were 11 mm (27), 13 mm (56), and 15 mm (24).
Implant success rate was evaluated using the five criteria suggested by Albrektsson (22), and the success rate was evaluated according to implant type, the length and diameter of the implant, and the time of second surgery.
Results (Tables 1~4)
Overall, 120 implants were placed in 50 patients with an 89.3% success rate. Xenograft (Bio-Oss�, BioCera�, BBP�) was successful in 75 of 86 cases (87.2%), while Xenograft + Allograft (Dembone�) was successful in 12 of 14 cases (85.7%) (Table 1).
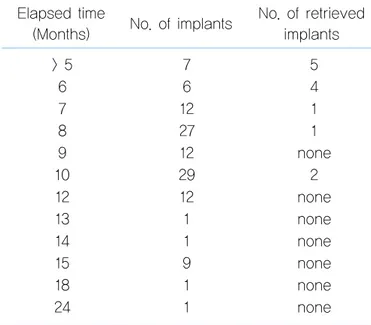
The implant failure rate was much higher when the second surgery was performed within 6 months.
Ⅲ
Table 1. Success rate of the various graft materials Materials No. of success implant / No.of total implant
(Success rate)
Xenograft 75 / 96 (87.2%)
Xenograft + Allograft 12 / 14(85.7%) Xenograft + Allograft 9 / 9 (100.0%)
Allograft 8 / 8 (100.0%)
Allograft + Xenograft 3 / 3 (100.0%)
Others 2 / 2 (100.0%)
Total 109 / 122 (89.3%)
Table 2. Success rate according to elapsed time.
> 5 7 5
6 6 4
7 12 1
8 27 1
9 12 none
10 29 2
12 12 none
13 1 none
14 1 none
15 9 none
18 1 none
24 1 none
Elapsed time
(Months) No. of implants No. of retrieved implants
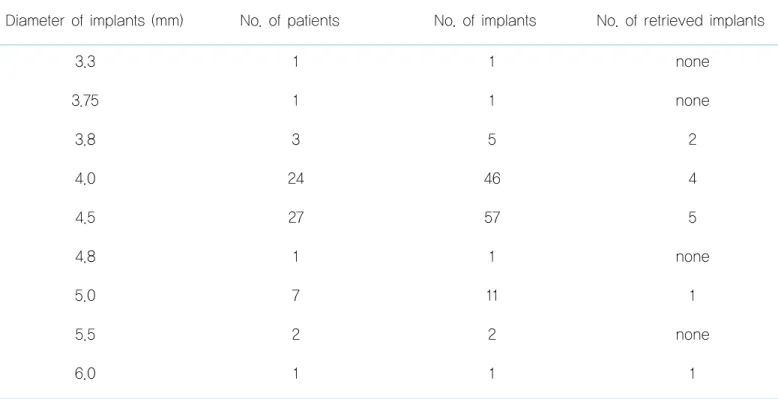
3.3 1 1 none
3.75 1 1 none
3.8 3 5 2
4.0 24 46 4
4.5 27 57 5
4.8 1 1 none
5.0 7 11 1
5.5 2 2 none
6.0 1 1 1
Table 4. Success rate according to implant length.
8 1 1 none
10 5 6 none
11 18 27 1
11.5 2 3 none
12 4 5 2
13 30 56 5
14 1 3 1
15 11 24 3
16 1 1 1
Length of implants (mm) No. of patients No. of implants No. of retrieved implants
original article
Summary and discussion
The maxillary sinus is connected to the nasal cavity through one or two inferior nasal meatus in the upper 1/3 of the internal wall of the maxillary sinus. If the maxillary sinus is elevated excessively, this area may be exposed, and care must be taken to avoid this. After birth, the maxillary sinus enlarges continuously and comes to occupy much of the maxilla. At adolescence, the maxillary sinus extends from the canine to the 3rd molar, and from the floor of the orbit superiorly to the root of the maxillary canine inferiorly. Consequently, the maxillary sinus interferes with implant placement near the maxillary canine. Therefore, implant placement requires elevation of the maxillary sinus mucosa. In addition, with loss of the maxillary canine, the alveolar bone is resorbed progressively from the buccal side, decreasing the height of the alveolar bone and shifting the crest of the alveolar bone toward the midline. Together with the pneumatization of the maxillary sinus, this makes implant placement difficult12).
In 1980, Boyne et al.8)first reported a significant increase in the thickness and height of alveolar bone in cases followed for 4 years after autogenous bone grafting in the maxillary sinus and they inserted a blade implant after a 6- month healing period. Misch et al.13) reported a
98% success rate for 170 implants with maxillary sinus grafts consisting of tricalcium phosphate mixed with demineralized bone and blood.
Autogenous bone can be used for sinus grafting.
Heterologous, allogenic, or synthetic bone used alone or in combination is effective implant material depending on the clinical situation14). The block pattern and particle shape were seen in 80.40 and 94.83% of grafts, respectively, and the particle pattern had a higher implant success rate15).
Autogenous bone is the gold standard for bone grafting in the oral cavity because of its osteoconduction and osteo-induction properties16). However, it has several shortcomings, including the additional hospital stay required for collecting extraoral bone, the need for a second surgery, and repneumatization of the maxillary sinus caused by resorption of the bone graft.
Consequently, the use of bone substitutes is increasing10).
Allografts include cortical or spongiose bone and are mainly obtained from cadavers or other donors. The bone is sterilized and stored in a bone bank. Technical problems are relatively frequent, and include the accuracy required to place the graft mass to the donor area, the need for firm fixation for successful fusion with the host bone, infection, non-union, and the possible fracture of the allograft. Allograft bone is not osteogenic, and when used in combination with autologous bone, osteogenesis is slower than when using autogenous bone alone.
Ⅳ
scaffolds to accelerate the repair and growth of bone tissues. Using allogenic bone or synthetic graft materials in combination with autologous bone for maxillary sinus grafts decreases the amount of autogenous bone needed, although osteogenesis may be insufficient or slow17).
The appropriate treatment method should be chosen after considering the advantages and shortcomings of autogenous and non- autogenous bone grafts. The advantages of non- autogenous bone are that no additionous surgery in another area is required, the postoperative infection rate is reduced, and the grafted bone is not resorbed during the healing period. Its shortcomings are that a longer bone regeneration period is required, and precise surgical techniques and appropriate selection of implant material are required to obtain the best result. The advantages of autogenous bone graft are that the period of bone regeneration is shorter than with a non-autogenous bone graft and the cost of non-autologous implant materials is avoided. The shortcomings are that additional surgery is required and slight bone loss occurs during the healing period18).
Recent studies have failed to detect significant associations between implant materials and the incidence of complications in maxillary floor elevation, and new bone developed within 6 months on average. In addition, no radiological
Conclusions
Maxillary mucosa elevation surgery was performed with xenogenic, allogenic, synthetic, and autogenous bone grafts, and 120 implants were placed. At the last follow-up, 107 implants remained attached to the upper prosthesis with no radiological or clinical signs of inflammation or mobility, and the patients could chew successfully, for an 89.2% success rate.
1. For xenografts alone, the success rate was 87.2% (75/86).
2. The most common implant diameters were 4.0 and 4.5 mm, and the success rate was 92.2% (94/102).
3. Implants of 13 mm in length were used most frequently, with a 91.1% (51/56) success rate.
References
1. Wheeler SL, Holmes RE, Calhoun CJ. Six-year clinical and histologic study of sinus-lift grafts. Int J Oral Maxillofac Implants 1996;11:26-34.
2. Butz SJ, Huys LW. Long-term success of sinus augmentation using a synthetic alloplast: a 20 patients, 7 years clinical report. Implant Dent 2005;14:36-42.
3. Krauser JT, Rohrer MD, Wallace SS. Human histologic and
Ⅴ
original article
histomorphometric analysis comparing OsteoGraf/N with PepGen P-15 in the maxillary sinus elevation procedure: a case report. Implant Dent 2000;9:298-302.
4. Tadjoedin ES, de Lange GL, Bronckers AL, Lyaruu DM, Burger EH.
Deproteinized cancellous bovine bone (Bio-Oss) as bone substitute for sinus floor elevation. A retrospective, histomorphometrical study of five cases. J Clin Periodontol 2003;30:261-270.
5. Wallace SS, Froum SJ, Cho SC, Elian N, Monteiro D, Kim BS, Tarnow DP. Sinus augmentation utilizing anorganic bovine bone (Bio- Oss) with absorbable and nonabsorbable membranes placed over the lateral window: histomorphometric and clinical analyses. Int J Periodontics Restorative Dent 2005;25:551-559.
6. Hurzeler MB, Kirsch A, Ackermann KL, Quinones CR.
Reconstruction of the severely resorbed maxilla with dental implants in the augmented maxillary sinus: a 5-year clinical investigation. Int J Oral Maxillofac Implants 1996;11:466-475.
7. Tatum OH Jr, Lebowitz MS, Tatum CA, Borgner RA. Sinus augmentation. Rationale, development, long-term results. N Y State Dent J 1993;59:43-48.
8. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg 1980;38:613-616.
9. Wallace SS, Froum SJ, Tarnow DP. Histologic evaluation of a sinus elevation procedure: a clinical report. Int J Periodontics Restorative Dent 1996;16:46-51.
10. Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 2004;24:565-577.
11. Kahnberg KE, Nystrom E, Bartholdsson L. Combined use of bone grafts and Branemark fixtures in the treatment of severely resorbed maxillae. Int J Oral Maxillofac Implants 1989;4:297-304.
12. Kim SG. Sinus Bone Graft, Narae Publishing Inc, 2004.
13. Misch CE. Maxillary sinus augmentation for endosteal implants:
organized alternative treatment plans. Int J Oral Implantol 1987;4:49- 58.
14. Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. Int J Oral Maxillofac Implants 1998;13:11-45.
15. Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol 2003;8:328-343.
16. Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J. Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J Oral Maxillofac Implants 2003;18:53-58.
17. Garg AK. Bone Biology, Harvesting, and Grafting for Dental Implants.
1st edition, 2005.
18. Fugazzotto PA, Pikos MA. Guided bone regeneration and sinus augmentation in the absence of autogenous bone grafting. Implant Dent 2001;10:158-161.
19. Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. Int J Oral Maxillofac Implants 2006;21:81-85.
트 식립시 상악동 거상술을 시행받고 보철물 장착 완료 후 사용기간이 2년 이상된 50명의 환자를 대상으로 시행하였다. 남자 는 29명, 여자는 21명으로 남자가 약간 더 많았으며, 평균 연령은 53.6세, 식립된 임프란트 개수는 120개 였다. 사용된 이식 재는 다양하였으며, 임프란트 성공 여부는 1986년 Albrektsson이 제시한 5가지 기준에 따라 평가하였으며, 이식재의 종류, 경과된 시간, 매식체의 직경 및 길이에 따라 각각의 성공률을 평가 하였다.
Xenograft 만 시행한 경우 75/86(87.2%)의 성공율을 보였다. 2nd surgery 시기는 7개월 이하시 60%로 현저히 성공율이 감소하였다. 4.0 ㎜ 및 4.5 ㎜ 직경이 가장 많이 식립되었으며, 94/102(92.2%)의 성공율을 보였다. 13 ㎜ 길이가 가장 많이 식립되었으며, 51/56(91.1%)의 성공율을 보였다. 향후 이식재와 사용된 임프란트의 표면처리 방식, 직경, 길이, 위치에 대한 보다 많은 자료에 대한 통계학적 연구가 필요할 것으로 사료된다.
교신저자 : 김학균 우편번호 : 501-825
주소 : 광주광역시 동구 서석동 421번지 조선대학교 치과병원 구강악안면외과 TEL: (062) 220-3816 E-Mail: [email protected] FAX: (062) 228-7316