J Rhinol 20(1), 2013
- 50 -
접형동에 발생한 악성 흑색종 1예
경희대학교 의과대학 이비인후-두경부 외과학 교실
박철언·이건희·김수진·신승엽
Malignant Melanoma of the Sphenoid Sinus
Cheol Eon Park, MD, Kun Hee Lee, MD, PhD, Su Jin Kim, MD and Seung Yup Shin, MD, PhD
Department of Otorhinolaryngology Head & Neck Surgery, Kyung Hee University, School of medicine
ABSTRACT
Sinonasal malignant melanoma comprises 0.5% ~ 1.5% of all malignant melanomas. Malignant melanoma in the nasal cavity is relatively more predominant than in the paranasal sinus. The maxillary sinus is the most common sinus cavity affected by malignant melanoma, and the sphenoid sinus is a very rare site regardless of a primary or secondary origin. We encountered a patient with frequent epistaxis who was found to have malignant melanoma at the nasal septum and sphenoid sinus. She was treated successfully with endoscopic sinus surgery, and we report this case, along with the associated literature.
KEY WORDS : Melanoma · Nasal Cavity · Sphenoid Sinus.
서 론
악성 흑색종은 신경 외배엽에서 유래하는 흑색아세포의 악성 변환에 의해 발생하며, 일반적으로 피부형과 점막형 으로 분류된다.1) 이 중 비강 및 부비동에 발생하는 점막형 악성 흑색종은 전체 악성 흑색종의 0.5%에서 1.5% 정도에 해당하며, 비강 및 부비동에 발생하는 전체 악성 종양의 약 3.5%에 해당하는 드문 질환으로, 적극적이고 광범위한 치 료에도 불구하고, 예후는 불량한 것으로 알려져 있다.2)
악성 흑색종은 부비동에 비해 비강에서 더 호발하며, 부비동에서는 상악동이 가장 호발부위이다.3) 4) 접형동에 발생한 악성 흑색종의 경우는 매우 드문 것으로 알려져 있다.
비강 및 접형동을 침범한 점막형 악성 흑색종을 치료, 경 험한 1예의 임상적 특성 및 치료 결과를 문헌고찰과 함께 보고하는 바이다.
증 례
80세 여자 환자가 수년간 지속된 우측 비출혈을 주소로 본원 이비인후과에 내원하였다. 환자는 비출혈 외에 두통 이나 복시, 안구통 등은 호소하지 않았다. 비내시경 검사에 서 우측 비중격에 3mm 정도 크기의 폴립 양상의 종물이 관 찰되었다(Fig. 1). 종물은 흑색이었고 표면은 매끄러웠으며 주변 조직과 유착되지 않은 양상이었다. 부비동 전산화 단 층촬영에서 조영증강되는 작은 비중격 종물과 우측 접형동 을 가득 채우는 연조직음영이 관찰되었다(Fig. 2). 우측 비 중격 및 접형동 주변의 골조직 파괴 등의 소견은 없었으며, 좌측 비강 및 부비동은 특이소견이 관찰되지 않았다. 전신 마취하에 조직검사를 겸해 비중격 종물 제거와 접형동종물 을 제거하였다. 접형동 자연공은 흑색종물과 점액 화농성 분비물로 가득차 있었으나 흑색종물은 크기가 작았으며 자 연공에 접해있어 자연공을 광범위하게 넓히고 종물이 접한 점막까지 절삭기와 sphenoid punch를 이용하여 제거하였 다(Fig. 3). 비중격 종물 역시 비중격 점막과 연골막을 포함 하여 광범위하게 절제를 시행하였다. 수술 후 시행한 조직 검사 결과 비중격 종물에서는 광학 현미경 소견에서 원형 논문접수일 : 2012년 1월 10일 / 심사완료일 : 2013년 5월 19일
교신저자 : 이건희, 서울특별시 강동구 상일동 149 강동경희대학교병원
전 화 : (02) 440-6180 · 전 송 : (02) 440-7336 E-mail : [email protected]
www.ksrhino.or.kr
박철언 등 : 비부비동 악성 흑생종 / 51
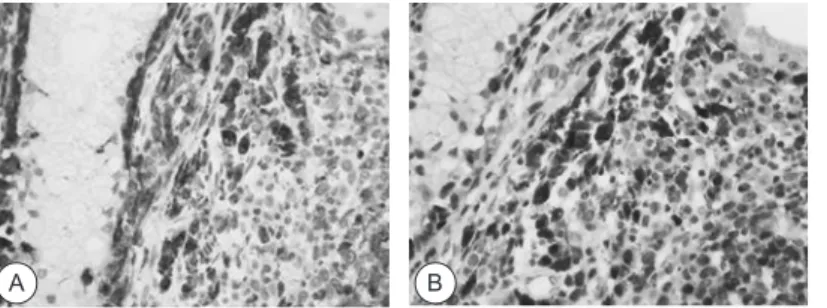
또는 난원형의 핵과 뚜렷한 핵소체를 가지고 있었고 핵 대 세포질의 비율이 높으며, 유사분열지수가 높은 악성의 조 직 소견을 보였으며, 접형동 종물에서는 광범위한 괴사를 동반한 악성종양의 소견을 보였다. 면역조직화학염색에서 종양 세포들은 leukocyte common antigen(LCA)에 음성 반응을 보이고, HMB-45, S-100 단백에 양성반응을 보여 악성 흑색종으로 진단되었다(Fig. 4).
조직 검사 결과가 악성 흑색종으로 진단되어 남아 있는 병변과 전신전이에 대한 평가를 위해 PET CT를 시행하였 으나, 잔류종양이나 임파선 전이, 전신 전이가 의심되는 부 위는 관찰되지 않았다. 방사선치료 권유하였으나 고령을 이유로 거절하였고 수술 후 1년 반 추적관찰에서 재발이나 전이의 소견은 관찰되지 않고 있다(Fig. 5).
고 찰
악성흑색종은 피부형과 점막형으로 나누는데 점막형이 피부형에 비해 진단이 늦고, 세포분열 빈도가 높고, 혈관이 나 림프계 침윤이 흔하여 예후가 좋지 않다. 또한 점막형은 증상이 비특이적이어서 조기발견이 어려우며, 침윤 정도를
정확히 결정하기 어려워 수술적 치료 시 병변 전체를 제거 하지 못할 가능성이 있다.5)
비강 및 부비동에서 점막형 악성흑색종의 호발 부위로는 비중격, 비강측벽, 중비갑개, 하비갑개, 상악동, 사골동 순 으로 알려져 있다.3) 4) Batsakis 등은 비강 및 부비동에서 발생한 악성흑색종 194례를 고찰하였으며, 이 중 접형동에 서 발생한 악성흑색종은 없었다고 보고하였다.2) Som 등은 악성흑색종은 절대 전두동과 접형동은 침범하지 않는다고 도 보고하였다.6)
그러나 2000년도에 Busaba 등은 처음으로 접형동 기원 의 악성흑색종 증례를 보여주며 접형동에서도 악성흑색종 이 발생할 수 있다고 보고하였다.7) 이 후에 지금까지 전세 계에서 6 례 정도의 접형동 기원의 악성 흑색종에 대한 보 고가 있으며, 아직 국내에서 보고된 바는 없다.7-12)
비강 및 부비동의 점막형 악성 흑색종은 대부분 50세 이 후에 발생하며, 남자에서 여자보다 약간 더 호발하는 것으 로 알려져있다.3) 13)
임상 증상은 비폐색 및 비출혈이 가장 흔하며 그 외에 비 루, 두통, 후비루 등의 비특이적인 증상을 보일 수 있는 것 으로 알려져 있다.5) 일반적으로 신체검사상 유두상 종괴로
Fig. 1. black pigmented mass on the right nasal septum was shown in endoscopic view.
Fig. 2. enhanced paranasal computerized tomographic scan showed soft tissue density in the right sphenoid sinus.
(A: coronal view, B: axial view)
Fig. 4. Histopathologic findings of malignant melanoma. A: Immunochemical stain for polygonal cells showing positive reaction for HMB-45 (X400). Melanin pigments are seen in the cytoplasm. B: S-100 positive cells (X400)
Fig. 5. Postoperative findings of malignant mel- anoma one year after surgery showed no evi- dence of recurrence. A: 0 degree endoscopic finding B: PET CT
Fig. 3. black-yellowish mass was found at the ostium of right sphe- noid sinus.
A
A A
B
B B
52 / J Rhinol 20(1), 2013
발견되며 단일성 혹은 다발성 병변으로 관찰될 수 있다. 하 지만 접형동에서 발생한 악성흑색종의 경우 종양은 해면정 맥동을 통해 두개내로 확장되거나, 시신경 주위로 성장하 게 된다. 따라서 접형동에서 발생한 악성흑생종이 진행하 게 되면, 환자는 비증상이 발생하기 전에 시력 감퇴, 복시, 두통 등을 호소하게 된다.
이전에 보고된 접형동에서 발생한 악성흑색종 6례에서 환자들은 공통적으로 두통을 호소하였다.7-12) 또한 6번 뇌 신경을 침범한 경우가 3례, 3번 뇌신경, 5번 뇌신경을 침 범한 경우가 3례, 4번 뇌신경을 침범한 경우가 1례였다. 이 러한 뇌신경 관련 증상은 수술 혹은 방사선 치료 후 회복 된 경우도 있었고, 남아있는 경우도 있었다. 하지만 본 증 례에서 환자는 비중격에서 발생한 악성흑색종에 의한 반복 적인 우측 비출혈을 호소하였을 뿐, 접형동에서 발생한 악 성흑색종과 관련하여 안과적 증상이나 두통 등은 호소하 지 않았다.
진단은 병리학적 특히 면역조직화학염색을 통해 가능하 며 leukocyte common antigen(LCA)에 음성반응을 보이 고, HMB-45, S-100 단백, tyrosinase, melan A, mi- crophthalmia transcription factor에 양성반응을 보인 다.14) 영상학적 진단 특히 MRI가 다른 질환과 감별진단에 도움이 되는데 T1-weighted image에서는 iso-hyper- intense, T2-weighted image에서는 hypointense하며 homogenous enhancement를 보여 meningioma, fungal sinusitis, lymphoma, mucocele 등과 감별할 수 있다.15)
치료에는 수술요법, 방사선요법, 항암 화학요법이 있으 나 근치적 수술 요법이 가장 우선적으로 고려된다. 원발병 소의 광범위한 절제가 다른 치료 요법들과 비교해 국소재 발, 국소 림프절 전이, 그리고 생존율에서 좋은 성적을 보 이기 때문이다.4) 그러나 비강 및 부비동의 악성 흑색종은 국소 림프절 전이 및 원격 전이의 빈도가 낮으므로, 림프 절 전이가 없으면 예방적 경부 곽청술은 실시하지 않는다.
방사선치료는 수술 후 종양이 남아있을 가능성이 있을 경 우, 국소절제가 불가능한 경우, 재발한 경우에 고식적인 요 법의 의미로 사용되고 있으나, 술후 보조 방사선요법이 국 소조절을 증가시키고 무병 생존율을 증가시킨다고 하여 충 분한 안전역 확보 유무와 관계없이 실시되어야 한다는 주 장도 있다.3) 16) 17) 한편 항암 화학요법은 원격전이가 있거 나 재발한 경우에 사용될 수 있으나 국소재발 및 국소 림 프절 전이, 생존율에 있어서 도움이 되지는 못하고 있다.
치료 실패의 주 원인은 경부 림프절 전이보다 국소 재발이 므로 병변의 조기 발견과 적절한 병기 평가 및 완전한 수 술적 절제가 생존과 치유에 가장 중요하다고 할 수 있다.14)
18) 본 증례에서는 주변 점막을 포함하여 안전역을 두고 광
범위 절제를 시행하였지만 악성 흑색종이 주위 혈관 및 림 프계의 침습 빈도가 높고 도약 병변이 존재하는 경우가 많 아 원발부위와 원발부위 인접의 재발 위험성이 높은 고위 험부위에 방사선 치료를 추가 시행을 계획하였으나 시행하 지 못하였다.
비강 및 부비동 악성흑색종 환자의 예후는 종양의 침범 정도 및 완전한 수술적 절제와 관련되어 있다. 점막형 악 성흑색종은 일반적으로 피부형 악성흑색종에 비해 증상이 늦게 나타나므로 예후가 나쁜것으로 알려져 있다. 따라서, 처음 내원시 국소 전이가 있는 경우가 많다. 5년 생존율이 11%, 20년 생존율이 0.5%, 평균 생존율이 2.3년 이라는 보 고가 있고,19) 또 다른 보고에서는 5년 생존율이 28%라는 보고도 있다.20) 21)
중심 단어:악성흑색종·비강·접형동.
저자역할(Author Contributions)
박철언, 이건희, 김수진, 신승엽 은 본 연구에서 모든 자료에 접근할 수 있으며, 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습 니다. 연구 기획 : 박철언, 이건희, 김수진, 신승엽. 자료 해석 및 분 석 : 박철언, 이건희, 김수진, 신승엽. 논문 초안 : 박철언, 이건희. 연 구 총괄 : 이건희
REFERENCES
1) Lee WJ, Oh KK, Shim YS, Lee YS. Malignant melanomas of the head and neck. Korean J Otolaryngol-Head Neck Surg 1994;37:1259-64.
2) Batsakis JG, Regezi JA, Solomon AR, et al. The pathology of head and neck tumors: mucosal melanomas, part 13. Head Neck Surg. 1982;4:404-18.
3) Lund VJ. Malignant melanoma of the nasal cavity and paranasal sinuses. Ear Nose Throat J 1993;72(4):285-90.
4) Stern SJ, Guillamondegui OM. Mucosal malignant melanoma of the head and neck. Head Neck 1991;13(1):22-7.
5) Snow GB, van der Esch EP, van Slooten EA. Mucosal melanomas of the head and neck. Head Neck Surg 1978;1(1):24-30.
6) Som PM, Brandwein M: Sinonasal cavities –Inflammatory dis- eases, tumors, fractures and postoperative findings, In: Head and Neck Imaging Vol 1 , Som PM, Curtin HD (eds), 3rd edition, Mosby, St.Louis 1996;126-318.
7) Busaba NY. Primary melanoma of the sphenoid sinus. Otolaryn- gol Head Neck Surg 2000;123:748–9.
8) Asano K, Sobata E, Yamazaki K, et al. Malignant melanoma aris- ing from the sphenoidal sinus: case report. Neurol Med Chir (To- kyo) 2000;40:329–34.
9) Pino Rivero V, Keituqwa Yanez T. Melanoma of sphenoid sinus:
case presentation and review of literature. Acta Otorrinolaringol Esp 2004;55:45–8.
10) Lynch SC, Lee AG, Graham SM, Kirby PA, et al. Primary mela- noma of the sphenoid sinus presenting with a third cranial nerve palsy. J Neuro-ophthalmol. 2005;25(4):289-92.
11) Carter TR. Pathologic quiz case 1. Malignant melanoma. Arch Otolaryngol Head Neck Surg 1986;112:450-3.
12) Shinbori T, Uyama E, Eto K, et al. An autopsy case of malig-
nant melanoma possibly originating in the sphenoid sinus. Rinsho Shinkeigaku 1988;28:636-42.
13) Freedman HM, DeSanto LW, Devien KD, Weiland LH, Roches- ter. Malignant melanoma of the nasal cavity and paranasal sinus.
Arch Otolaryngol 1973;97:322-5.
14) Thompson LD, Wieneke JA, Miettinen M. Sinonasal tract and nasoparyngeal melanomas: a clinicopathologic study of 115 cases with a proposed staging system. Am J Surg Pathol 2003;27(5);594- 15) Batra K, Chhabra A, Rampure J, Tang S, Koenigsberg R, Gonza-611 les C. CT and MRI appearances of primary sphenoid melanoma:
a rare case. Am J Neuroradiol 2005;26;2642-4.
16) Gilligan D, Slevin NJ. Radical radiotherapy for 28 cases of mucosal melanoma in the nasal cavity and sinuses. Br J Radiol 1991;64(768):1147-50.
17) Anderson LJ, Berthelson A, Hansen HS. Malignant melanoma of the upper respiratory tract and the oral cavity. J Otolaryngol 1992;21(3):180-5.
18) Dauer EH, Lewis JE, Rohlinger AL, Weaver AL, Olsen KD. Si- nonasal melanoma: a clinicopathologic review of 61 cases. Oto- laryngol Head Neck Surg 2008;138(3):347-52.
19) Holdcraft J, Gallagher JC. Malignant melanomas of the nasal and paranasal sinus mucosa. Ann Otol Laryngol Rhinol 1969;78:5- 20) Lund VJ, Howard DJ, Harding L, Wei WI. Management options 21.
and survival in malignant melanoma of the sinonasal mucosa.
Laryngoscope 1999;109(2pt1) :208-11.
21) Prasad ML, Busam KJ, Patel SG, Hoshaw-Woodard S, Shah JP, Huvos AG. Clinicopathologic differences in malignant melanoma arising in oral squamous and sinonasal respiratory mucosa of the upper aerodigestive tract. Arch Pathol Lad Med 2003;127(8):997- 1002.
박철언 등 : 비부비동 악성 흑생종 / 53