- 133 -
J Rhinol 17(2), 2010 www.ksrhino.or.kr
INTRODUCTION
The posterior ethmoid sinuses are related to the poste- rior half of the orbit, particularly the optic nerve. There- fore, lesions in the posterior ethmoid cell are frequently associated with ocular symptoms, such as visual loss, vi- sual fields defects, proptosis, and extraocular palsies rath- er than nasal symptoms. In particular, Onodi cell is a large pneumatized posterior ethmoid cell that pneumatizes lat- erally and superiorly to the sphenoid sinus. Thus, optic nerve may be exposed along the superior lateral wall.1) Due to this close relationship between the Onodi cell and the optic nerve, the Onodi cell is considered one of the most important structures to be identified before surgery.
A mucocele is a chronic, expansive, and cystic lesion lim- ited by the mucosa of the paranasal sinus. Most muco- celes often occur in the frontal and anterior ethmoid sinus rather than the posterior ethmoid and sphenoid sinus.
We describe a patient with infected mucocele in the Onodi cell associated with acute visual loss and necessity
of imaging studies for the differential diagnosis.
CASE REPORT
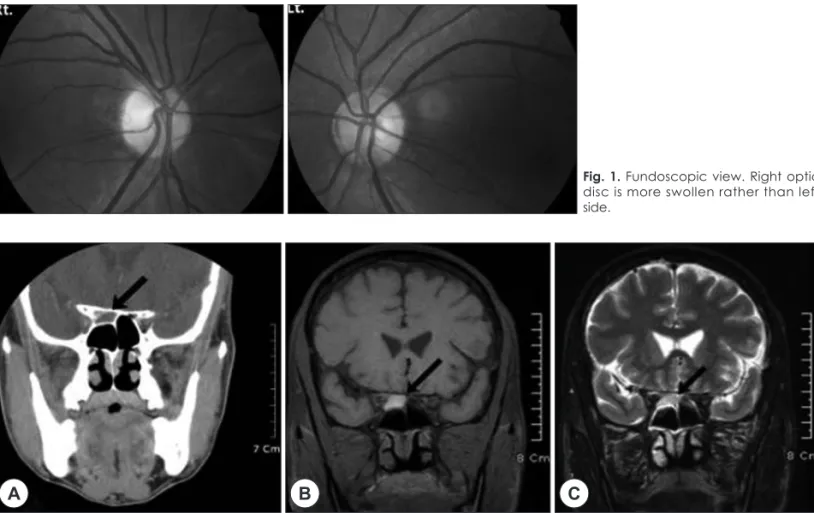
A 54-year old man was referred to our department with the blindness of right eye associated right-sided headache and retrobulbar pain. Five days ago, he visited at the de- partment of neurology with headache, ocular pain and blurred vision. Brain computed tomography (CT) was checked, but unremarkable. Thereafter, his visual acuity was gradually deteriorated, referred to the department of ophthalmology. On ophthalmological examination, visual acuity was 0.2 in right eye and 1.0 in left eye. Color vi- sion test of right eye was failed. Right optic disc papilla showed mild swelling on fundoscopic examination (Fig.
1). Visual field analysis revealed large central scotoma in right eye. Both intraocular pressure was normal. A right relative afferent pupillary defect (RAPD) was present.
Computed tomography (CT) and magnetic resonance im- age (MRI) of the orbit were performed and showed nor- mal brain, but demonstrated isodense, oval-shaped lesion in the posterior ethmoid sinus in the coronal-sectioned CT, isosignal intensity in T2W MRI, hypersignal intensi- ty in T1W MRI (Fig. 2). The optic nerve margin of right eye was high signal intensity in T2W MRI. Therefore he was referred to our department. On physical examina- tion, head and neck were unremarkable. Nasal endoscop-
Acute Visual Loss Caused by Onodi Cell Mucopyocele
Jinsu Choi, MD, Kisik Kim, MD and Bosung Kim, MD
Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Dongguk University, Gyeongju, Korea
ABSTRACT
Acute visual loss caused by an infected mucocele in an Onodi cell is extremely rare. The Onodi cell is a pneumatized pos- terior ethmoid cell located laterally and superiorly to the sphenoid sinus and closely related to the optic nerve. Therefore, a mucocele affecting the Onodi cell that has encroached on the adjacent sphenoid bone forming the optic canal can rarely present with visual loss. We describe a rare case of retrobulbar optic neuritis caused by an infected mucocele in the Onodi cell.
A 54-year-old male complained of headache and visual loss in his right eye. A computed tomography scan and magnetic reso- nance image demonstrated a mucocele occupying the Onodi cell on the right side. Surgical treatment with an endoscopic sinus approach was performed, resulting in improvement of visual acuity. A lesion in an Onodi cell may be associated with ocular symptoms even if the lesion is isolated or small. Imaging studies should be considered for the differential diagnosis because early diagnosis and prompt surgical treatment for mucocele are needed for recovery of visual function.
KEY WORDS:MucoceleㆍOnodi cellㆍOptic neuritis.
Address correspondences and reprint requests to Jinsu Choi, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Dongguk University, 1090-1 Seokjang- dong, Gyeongju 780-350, Korea
Tel:82-54-770-8572, Fax:82-54-770-8378 E-mail:[email protected]
Received for publication on January 28, 2010 Accepted for publication on March 24, 2010 online©MLComm
134 / J Rhinol 17(2), 2010
ic examination showed no inflammatory changes, such as edema, polyps, or purulent discharge. Clinical impres- sion was rhinogenic optic neuropathy caused by isolated Onodi cell mucocele. Endoscopic sinus approach was performed. After anterior and posterior ethmoidectomy, the mucocele was identified and marsupialized (Fig. 3).
Intraoperatively, inspissated purulent material was pre- sented in the Onodi cell mucocele which was evacuated and cultured. Bacteriologic study revealed mixed infec- tion of E. coli, Enterobacter aerogenes, coagulase nega- tive staphylococcus. Postoperatively, he was administrat- ed intravenous steroid (Methysol®) at a dosage of 250 mg/day for 1 day and intravenous antibiotics for 3 days.
His visual acuity was gradually improved. Postoperative 20 days later, visual acuity in right eye was 1.0, but mild- ly remained paracentral scotoma (Fig. 4). Color vision test was normalized.
DISCUSSION
The Onodi cell has been defined as a most posterior ethmoid cell that has pneumatized laterally and superior- ly to the sphenoid sinus.2) The prevalence of Onodi cells varies from 7% using CT to 60% by anatomic dissection in cadavers.3)4) It has been reported to be more prevalent in Asia compared to the West contries (60% vs. 39%).3) The incidence of Onodi cell rages from 8%5) to 13%6) on the basis of CT and radiologic findings, and its clinical im- portance lies in its close proximity to the optic nerve and
Fig. 1. Fundoscopic view. Right optic disc is more swollen rather than left side.
Fig. 2. Coronal computed tomography reveals a sightly soft tissue density (arrow) in Onodi cell of right posterior ethmoid sinus (A). High signal intensity is showed in the same lesion in Coronal T1 weighted magnetic resonance image (B), intermediate signal intensity showed in Coronal T2 weighted magnetic resonance image (C).
A B C
Fig. 3. Intraoperative endoscopic view. Onodi cell is well marsu- pialized.
Choi et al:Visual Loss by Onodi Cell Mucopyocele / 135
internal carotid artery which often run within its cavity.
This explains the devastating loss of vision in our case with a infected mucocele of the Onodi cell.
Mucoceles are epithelium-lined mucus-containing sacs completely filling a paranasal sinus as a result of obstruc- tion of the sinus ostium. They are capable of expansion, aided by the production of osteolytic factors, notably pros- taglandins and collagenases. They are characterized by slow enlargement over years unless infection causes a pyo- cele.7)
In the case of sinonasal mucocele, the paranasal sinus is filled with exudates, the paranasal sinus is enlarged, and there is displacement, destruction or resorption of the bony wall. As the cause of these changes, narrowing or block- age of the paranasal sinus ostium, inflammation, and oth- er conditions have been proposed.8) The mechanism of bone resorption had been thought to involve internal pressure due to retained fluid, but more recently interleu- kin-1 (IL-1) and other bone-resorption-promoting cyto- kines that are produced by the mucocele epithelium have been suggested to be involved.9) Approximately 90% of primary mucoceles are thought to be formed in the bound- ary area between the frontal sinus and the anterior ethmoid
sinus.9) The ostia of posterior ethmoid sinus and sphenoid sinus are wide, resulting in a low incidence of mucocele formation. In particular, formation of a primary mucocele in an Onodi cell is extremely rare.
Two causative mechanisms for the visual disturbances have been proposed.10) According to one theory, cleavage of the optic canal wall or bone resorption occurs, the op- tic nerve is directly compressed by the mucocele, and ischemia of the nerve and venous congestion develop. It is thought that because the inside of the optic canal is not lined with fat or other soft tissues, pressure that is applied externally is readily transferred directly to the nerve. The second theory postulates that inflammation occurs due to an infection in the mucocele and spreads to the nerve via a cleavage in the optic canal wall or via a bone resorption site. In our patient, gross observation during the operation did not reveal the optic nerve to be exposed, and for this reason it can be surmised that inflammation had spread via a cleavage in the optic canal wall or small site of bone resorption caused by the mucocele. Also, inflammatory products spread through the vascular or lymphatic vessles could be a cause for optic neuritis.
In general, the prognosis is poor when the preoperative degree of visual impairment is high or when its onset is very sudden. It has also been reported that even when the degree of visual impairment is high, recovery of visual acuity is achieved when surgery is performed within 2 days after the decrease in visual acuity occurs and within 24 hours of the loss of light sense.11) In cases with a mild to moderate degree of visual impairment and gradual progression, the prognosis depends on the time from on- set until surgery is performed.10) Thus, it is desirable for sur- gery to be perfomed quickly.
Ogata et al. discussed two problems associated with lesions of an Onodi cell.12) One is that it is easy for an Onodi cell to escape detection when only a horizontal- section CT scan is performed. The posterior ethmoid cells are 8 to 20 mm in size, and there is a possibility that an Onodi cell itself would not be detected when using a slice width of 10 mm or more. In addition, Onodi cells are generally flat and are positioned laterally and superi- orly to the sphenoid sinus. Thus, Ogata et al. pointed out that a coronal-section CT scan and MR are useful for the diagnosis and evaluation of the Onodi cells. The second problem is that we lack anatomical knowledge regarding Onodi cells. In our patient, a coronal- section CT scan and MR were useful for the diagnosis. The horizontal-section CT alone was unable to reveal the lesion in the paranasal sinus, and there is a possibility that it would have escaped
Fig. 4. Visual field analysis (VFA). Preoperative VFS shows com- plete visual field defect of right eye (top). Postoperative 4 days later, VFS shows slightly improved in central lesion (middle). Post- operative 20 days later, VFS shows nearly complete improve- ment in central lesion, but remained paracentral visual field de- fect (bottom).
136 / J Rhinol 17(2), 2010
detection in the absence of anatomical knowledge re- garding the existence of Onodi cells and knowledge that a mucocele limited to that area could develop and if a coronal-section CT scan had not been performed.
The MR imaging signal characteristics typical of a mu- cocele reflect the protein content of the mucoid material.
On T1-weighted sequences, signal intensity is initially decreased, due to its high water content. However, as wa- ter is resorbed in the course of time, the protein content and viscosity are increased, resulting in signal intensity that is initially isointense and then hyperintense, relative to the brain on T1-weighted images. On T2-weighted images, the signal intensity usually remains high, but may be decreased as the contents become inspissated.13)
In our case, Onodi cell lesion showed partially erosion of inferior border in CT, moderately signal intensity in T1-weighted MRI, partially rim enhancement in enhanced T1-weighted MRI. Purulent Mucinous secretion was drained during marsupialization. We concluded infected muco- cele of Onodi cell rather than sinusitis.
Although paranasal mucoceles are usually deemed be- nign and treated on an elective basis, management should be prompt, especially if clinical evidence of inflamma- tion or infection is already present, as pyoceles in any loca- tion can lead to devastating loss of vision.14)
As in our patient, Visual impairment can occur even when the mucocele lesion is small and restricted to an Onodi cell. Accordingly, we suggest that MR and coronal-sec- tion CT scan are necessary for the evaluation of retrobul- bar optic neuritis.
저자역할(Author Contributions)
최진수, 김기식, 김보성은 본 연구에서 모든 자료에 접근할 수 있 으며 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습니 다. 연구 기획:최진수. 자료 해석 및 분석:최진수, 김기식, 김 보성. 논문초안:최진수. 논문수정:최진수. 연구 총괄:최진수.
REFERENCES
1) Yanagisawa E, Weaver EM, Ashikawa R. The Onodi (Sphenoeth- moid) cell. Ear Nose Throat J 1998;77(8):578-80.
2) Stammberger HR, Kennedy DW. Paranasal sinuses: Anatomic ter- minology and nomenclature. Ann Otol Rhinol Laryngol (Suppl) 1995;
167:7-16.
3) Thanaviratananich S, Chaisiwamongkol K, Kraitrakul S, Tang- sawad W. The prevalence of an Onodi cell in adult Thai cadavers.
Ear Nose Throat J 2003;82(3):200-4.
4) Unal B, Bademci G, Bilgili YK, Batay F, Avci E. Risky anatomic variations of sphenoid sinus for surgery. Surg Radiol Anat 2006;
28(2):195-201.
5) Jones NS, Strobl A, Holland I. A study of the CT findings in 100 patients with rhinosinusitis and 100 controls. Clin Otolaryngol Al- lied Sci 1997;22(1):47-51.
6) Meloni F, Mini R, Rovasio S, Stomeo F, Teatini GP. Anatomic vari- ations of surgical importance in ethmoid labyrinth and sphenoid sinus. A study of radiological anatomy. Surg Radiol Anat 1992;14 (1):65-70.
7) Lund VJ, Harvey W, Mehji S, Harris M. Prostaglandin Synthesis in the pathogenesis of fronto-ethmoial mucoceles. Acta Otolaryngol 1998;106(1-2):145-51.
8) Lund VJ, Henderson B, Song Y. Involvement of cytokines and vascular adhesion receptors in the pathology of fronto-ethmoidal mucoceles. Acta Otolaryngol 1993 ;113(4):540-6.
9) Ohnishi T, Ashikawa R, Shirahata Y, Asano Y. Fronto-ethmoidal mucocele-observation of its mode of enlargement. Rhinology 1982;
20(4):213-21.
10) Moriyama H, Hesaka H, Tachihashi T, Honda Y. Mucoceles of ethmoid and sphenoid sinus with visual disturbance. Arch Otolar- yngol Head Neck Surg 1992 ;118(2):142-6.
11) Yumoto E, Hyodo M, Kawakita S, Aibara R. Effect of sinus sur- gery on visual disturbance caused by spheno-ethmoid mucoceles.
Am J Rhinol 1997;11(5):337-43.
12) Ogata Y, Okinaka Y, Takahashi M. Optic neuropathy caused by an isolated mucocele in an Onodi cell. ORL J Otorhinolaryngol Relat Spec 1998;60(6):349-52.
13) Lim CC, Dillon WP, McDermott MW. Mucocele involving the an- terior clinoid process: MR and CT finding. Am J Neuroradiol 1999;20(2):287-90.
14) Loo JL, Looi AL, Seah LL. Visual outcomes in patients with pa- ranasal mucoceles. Ophthal Plast Reconstr Surg 2009;25(2):126-9.