Journal of Surgical Ultrasound is an Open Access Journal. All articles are distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright ⓒ 2014 by The Korean Surgical Ultrasound Society
ISSN 2288-9140
응급실에서의 초음파의 활용
가톨릭대학교 의과대학 응급의학교실 외상외과
김지훈, 김성집, 조항주
Ultrasound Applications in the Emergency Room
Ji Hoon Kim, Sung Jeep Kim, Hang Joo Cho
Division of Trauma Surgery, Department of Emergency Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
Received October 10, 2014 Revised October 30, 2014 Accepted November 3, 2014
Emergency sonography is focused, easy to learn, and relatively quick to perform. It can also have a direct impact on clinical decision making in an emergency operation. Therefore, if an emergency operation is performed in a timely fashion, it can have significant effect on the prognosis of patients. Performance of sonography by the general surgeon performing the operation can simplify the decision making process. In addition, the general surgeon’s un- derstanding of the patient’s history and knowledge of surgical anatomy can can have a sig- nificant impact on the outcome of patients. Major applications of emergency ultrasound in- clude trauma, abdominal aortic aneurysm, echocardiography, biliary system, deep vein thrombosis, soft tissue, and thorax. The coverage of the emergency ultrasound performed by the surgeon is expected to increase and have a more important role in the future.
Keywords: Emergency department, Ultrasonography, Point-of-care ultrasonography Correspondence to:
Hang Joo Cho
Division of Trauma Surgery, Department of Emergency Medicine, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu 480-717, Korea Tel: +82-31-820-5066 Fax: +82-31-847-2717
E-mail: [email protected]
서 론
1980년 초 우리나라에서 초음파 장비가 의료분야에서 사용되기 시작한 후, 처음에는 복부, 유방갑상선 등에서 활용되기 시작하였으나 현재는 전신에 초음파가 활용된 다고 해도 과언이 아니다.(1) 또한 처음에는 영상의학과에 의해서 초음파가 주로 시행되었지만, 현재는 각 임상과에 서 초음파를 직접 시행하고 있다. 특히, 외과의사들은 응 급 환자를 진단하고 치료하는 최일선에 있으므로 응급실 에서의 초음파(응급초음파)에 대해서 잘 알고 활용한다면 큰 도움이 될 것이다. 이에 저자들은 응급실에서 외과의사 가 초음파를 시행하였을 때의 장점 및 활용할 수 있는 초음 파의 종류 및 특징에 대하여 논하고자 하였다.
본 론
1. 응급초음파의 특징
응급초음파는 응급실에서 생명을 위협하는 급성 질환 의 즉각적인 진단을 가능하게 하고, 초음파 유도를 통하여 시술에 도움을 주며, 궁극적으로 환자의 예후를 향상시키 게 된다.(2-4) 응급 초음파의 특징은 다음과 같다.(3,4) 첫 번째는 집중성(focused)이다. 증상이 없지만 검사를 진행하거나, 아픈 원인이 무엇인지를 찾는 검사가 아닌, 하나 또는 두 개의 질문에 대답하는 형식의 초음파이다.
예를 들면 상복부 통증 환자가 응급실에 내원하였을 때
“상복부 통증의 원인이 무엇인가?”가 아니라, “담낭의 결 석이 있는가?”라는 질문에 대한 대답을 할 것이며, 복부
REVIEW ARTICLE
J Surg Ultrasound 2014;1:64-67
Journal of Surgical UltrasoundJSUJi Hoon Kim, et al: Ultrasound Applications in the Emergency Room
65
Table 2. Core Emergency Ultrasound Applications Trauma
Abdominal Aortic Aneurysm Echocardiography
biliary system Deep vein thrombosis Soft-tissue
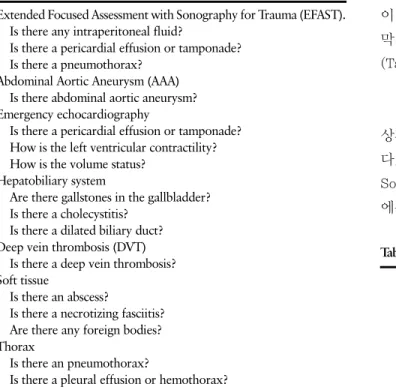
Thorax Table 1. Main Questions in the Field of Emergency Ultrasound
Extended Focused Assessment with Sonography for Trauma (EFAST).
Is there any intraperitoneal fluid?
Is there a pericardial effusion or tamponade?
Is there a pneumothorax?
Abdominal Aortic Aneurysm (AAA) Is there abdominal aortic aneurysm?
Emergency echocardiography
Is there a pericardial effusion or tamponade?
How is the left ventricular contractility?
How is the volume status?
Hepatobiliary system
Are there gallstones in the gallbladder?
Is there a cholecystitis?
Is there a dilated biliary duct?
Deep vein thrombosis (DVT) Is there a deep vein thrombosis?
Soft tissue
Is there an abscess?
Is there a necrotizing fasciitis?
Are there any foreign bodies?
Thorax
Is there an pneumothorax?
Is there a pleural effusion or hemothorax?
외상환자의 경우는 “어떤 복부 장기가 손상을 받았는가?”
라는 질문에 대한 대답이 아닌 “복강 내 저류액이 있는 가?”라는 단순한 질문에 “예, 아니오” 형태로 대답하는 초 음파의 형식을 하고 있다(Table 1). 두 번째는 초음파의 결 과가 임상적 결정에 직접적인 영향을 미치게 된다. 예를 들어, 초음파의 결과에 따라서 수술 여부가 결정되기도 한 다. 세 번째로 응급 질환을 진단하게 되므로 가능한 빨리 환자에게 시행하게 된다. 네 번째로 시간이 오래 걸리지 않는다. 우리가 원하고자 하는 답만 얻으므로 꼭 확인해야 할 영상의 숫자가 적다. 다섯 번째로 다른 초음파에 비해 서 배우기가 쉽다. 우리가 원하는 중요한 물음에만 답할 정도면 충분하다.
2. 외과의사에 의하여 행해지는 초음파(Surgeon performed ultrasound)
1993년부터 외과의사에 의한 초음파가 주목을 끌기 시 작하였다.(5) 외과의사가 초음파를 시행 한다면 많은 장점 이 있다. 첫 번째로는 본인 앞으로 입원한 환자를 보게 되 므로 직접적인 책임감과 동기를 부여 받게 된다. 두 번째로 환자에 대해서 누구보다 잘 알고 있다. 다른 사람이 초음파 를 할 경우에는 환자의 병력을 설명해야 하지만 그럴 필요
가 없다. 세 번째로 빠른 진단과 의사결정이 가능하다. 외 상에 의한 혈복강을 외과의사가 초음파로 진단했다면, 다 른 의사전달 과정 없이 바로 수술의 결정이 가능하다. 네 번째는 반복성이다. 입원환자에 대해서 시간만 허락된다 면 다른 과에 의뢰할 필요 없이 반복이 가능하고 이를 통해 서 초음파의 민감도를 올릴 수 있다.(6) Lindelius 등(7)은 응급실로 내원한 800명의 급성복증 환자를 대상으로 외 과의사가 응급실에서 직접 초음파를 시행한 군과 그렇지 않은 군으로 분류하였을 때, 외과의사가 응급실에서 초음 파를 시행하였을 때 영상의학과에 의한 추가 초음파의 시 행 건수가 적었고(8.7% vs 27.5%, P<0.001), 응급실에 서 수술 여부에 대한 의사결정 건수가 통계적으로 유의하 게 많았다고 하였다(34.5% vs 16%, P=0.013). Burford 등(8)은 급성 충수염의 진단에서 외과의사에 의한 초음파 의 정확도가 영상의학과의 정확도에 비해 통계적으로 차 이가 없지만, 이학적 검사와 초음파가 같은 의사에 의하여 실행되었을 경우 더 높은 정확도를 얻을 수 있었다고 하였 다. 이런 점에서 외과의사의 직접 초음파는 그 장점을 분 명히 가지고 있다고 하겠다.
3. 응급초음파의 종류
먼저 진단에서는 외상, 복부동맥류, 응급 심장초음파, 간담췌, 심부정맥혈전증, 연부조직, 흉부에 대하여 응급 초음파를 시행할 수 있다.(9) 초음파 유도 시술에도 응용 이 가능한데 중심정맥 삽관술, 심낭천자술, 복부천자, 흉 막천자, 이물제거술, 농양의 진단 및 배액술 등이 있다 (Table 2).(9)
1) 외상
응급초음파의 효시라고 볼 수 있으며, 1970년대부터 외
상환자에서 복강 내 저류액의 유무를 확인하기 시작하였
다. 1996년 Rozycki 등(10)은 Focused Abdominal
Sonogram for Trauma를 FAST로 기술하였으며, 1999년
에는 국제합의회의를 통하여 FAST를 Focused Assess-
J Surg Ultrasound Vol. 1, No. 2, 2014
66
ment with Sonography for Trauma의 약자로 표기하였 다.(11) FAST에 기흉의 검사를 더하여 EFAST (Extended FAST)로 표기하기도 한다.(12)
FAST에서는 네 군데, EFAST에서는 양측 흉부 두 군데 를 더하여 총 여섯 군데의 영상이 필요하다. 먼저 Subxi- phoid를 통하여 심낭압전의 유무를 관찰하며, 모리슨 궁, 좌측 횡격막 하부, 더글라스 와에서 액체의 저류 유무를 관찰한 후, 여기에 더해서 양측 흉부 늑간을 종스캔하여 기흉의 유무를 판단하게 된다. EFAST에는 약 5분 내외의 시간이 걸리게 된다. 민감도와 특이도는 둔상환자에서 각 각 90%, 99%이며, 관통상에서는 91%, 100% 정도이 다.(13)
2) 복부대동맥류
복부대동맥류는 늦지 않게 진단하는 것이 상당히 중요 하다. 복부대동맥류가 의심되는 환자에서 이학적 검사는 진단율이 떨어지며, CT는 조영제를 사용하며 방사선 조 사가 필요하고 검사 시간이 길다.(3) 응급 초음파를 시행 하면 환자를 CT실로 이동하지 않고도 빠르고 정확하게 진 단이 가능하다. 응급 초음파의 복부대동맥류 진단에서 민 감도는 100%, 특이도는 98%, 양성예측도 98%, 음성예측 도 93%이다.(14)
3) 심장초음파
응급 심장초음파는 심낭 삼출 또는 심낭 압전을 진단하 며, 심장(특히 좌심실)의 기능 평가 및 하대정맥 관찰을 통 한 수화상태 또는 저혈량성 쇽의 진단을 할 수 있다. 심낭 삼출 또는 압전은 주로 subxiphoid view를 통해 관찰하게 된다. 좌심실의 기능은 주로 박출계수를 통해 알 수 있으며 부흉골 장축(parasternal long axis) 및 단축(short axis), 첨부 4방 영상(apical 4 chamber view)에서 모두 측정이 가능하다. 하대정맥은 흡기 시 최소 직경이, 호기 시 최대 직경이 된다. 이를 이용하여 하대정맥(IVC)의 collapsi- bility index (IVC직경
호기-IVC직경
흡기/IVC직경
호기)를 구 하여 이 수치가 0에 가까울수록 수화가 잘 되어 있으며 100 에 가까울수록 탈수가 되어 있다고 판정한다.(15)
4) 담도
담도 영역에서 응급초음파의 활용은 주로 담석의 유무, 담도의 폐색, 담낭염의 유무에 대해서 관찰하게 된다. 외 과의사가 응급초음파를 시행 시 담석의 진단율은 민감도 96%, 특이도 99%까지도 보고되었다.(16)
5) 심부정맥혈전증
압축 초음파(compression ultrasound)는 상당히 정확 한 심부정맥혈전증의 진단법이다. 완전한 하지 정맥에 대 한 검사는 많은 시간이 필요하므로 응급초음파는 이를 간 략화 하여 두 점(two point) 또는 세 점(three point) 초음 파를 시행하게 된다. 두 점 초음파는 총 대퇴 정맥과 슬와 정맥을, 세 점 초음파는 두 점 초음파에 더하여 proximal greater saphenous vein을 추가로 관찰하여 정맥의 압축 가능 여부를 측정하게 된다.(17,18) Crisp 등(17)은 두 점 초음파로도 민감도 100%, 특이도 98%를 보고하였다. 영 상은 한 정맥에서 압축 전후로 두 장씩 얻어 두 점 초음파 에서는 총 4장, 세 점 초음파에서는 총 6장의 영상을 얻어 심부정맥혈전증의 여부를 진단하게 된다.
6) 연부조직
연부조직에서는 봉와직염 또는 농양, 괴사성 근막염, 이물에 대한 진단을 하게 된다. Squire 등(19)은 봉와직염 과 농양이 의심되는 환자를 대상으로 30분의 교육을 마친 의사에게 농양의 여부에 대한 초음파를 시행하게 하였을 때, 민감도 98%, 특이도 88를 보고하여 초음파에 의한 농 양의 진단이 배우기 쉽고 정확하다고 하였다. 농양의 경우 외과의사가 초음파를 시행한다면 진단과 동시에 배농술 또한 가능할 것이다. 괴사성 근막염의 경우에도 초기 진단 이 어려운 경우가 많은데 초음파를 통하여 진단이 가능하 며, 이물에 대한 진단, 위치 확인, 제거 또한 초음파를 이 용한다면 수월하게 시행이 가능하다.(20,21)
7) 흉부
흉부에서 응급초음파는 기흉과 흉수의 여부에 대해서
판단하게 된다. 물론 폐부종이나 성인호흡곤란증후군
(ARDS)에 대해서도 초음파를 하는 경우도 있지만, 응급
초음파에서 특히 기흉과 흉수에 대한 초음파는 쉬우면서
도 유용하고, 단순 흉부 X선 검사에 비해서 민감도도 더욱
우수하다.(22,23) 둔상에 의한 외상성 기흉 환자에서 초
음파의 민감도는 86-98%인 반면 앙와위 단순 흉부 X선
검사의 민감도는 28-75%로 초음파에서 더 우수한 민감도
를 보여주었다.(22) Eibenberger 등(23)은 51명의 환자를
대상으로 흉수의 양을 얼마나 정확하게 측정할 수 있는 가
를 초음파와 측와위 단순 영상검사 비교하였을 때, 초음파
에 의한 오차평균은 224 ml로 측와위 단순 영상의 오차평
균 465 ml에 비하여 통계적으로 유의하게 적다고 하여,
초음파가 측와위 단순 영상검사보다 흉수의 양을 정확히
Ji Hoon Kim, et al: Ultrasound Applications in the Emergency Room