초음파 및 컴퓨터 단층촬영 영상에서 내경정맥의 해부학적 변형의 비교
중앙대학교 의과대학 외과학교실
박병욱, 이한별, 김향경
Anatomical Variations in the Internal Jugular Vein on Ultrasound and Computed Tomography for Performing Vascular Cannulation
Byung Wook Park, Hanbyul Lee, Hyangkyoung Kim
Department of Surgery, Chung-Ang University College of Medicine, Seoul, Korea
Received May 15, 2017 Revised July 1, 2017 Accepted July 3, 2017
Purpose: The internal jugular vein (IJV) is known to have many anatomic variations and is
associated with various complications during puncture. We tried to confirm whether the preprocedural computed tomography (CT) image could be used as a reference by replacing the real-time ultrasound (US) guidance during catheterization.Methods: We retrospectively analyzed 250 patients who received central venous catheter
(CVC) insertion through the right IJV whose US and CT images were available from September 2013 to March 2016. The relative position of the IJV to the carotid artery was categorized into five groups by the vertical axis to the ground on US and CT (CTg) or by perpendicular axis to the skin on CT (CTs). The IJVs were divided into two groups accord- ing to the degree of safety for cannulation as groups of favorable anatomy (FA) and un- favorable anatomy (UA).Results: According to US, FA and UA, there were 91 (36.4%) and 159 (63.6%) patients, 181
(72.4%) and 69 (27.6%) patients in the CTg, 35 (14.0%) and 215 (86.0%) patients in the CTs. There was a statistically significant difference between CTg and CTs images (P<0.001), as well as between US and CT images (P<0.001).Conclusion: CT images could provide limited information about anatomic variations in the
IJV. However, when the neck is rotated, the degree of overlap of the IJV and carotid artery increases. Therefore, due to frequent anatomic variations of the two vessels, special regards to these variations are needed when attempting catheterization through the IJV.Keywords: Ultrasound, Internal jugular vein, Carotid artery, Central venous catheter,
Computed tomographyCorrespondence to:
Hyangkyoung Kim
Department of Surgery, Chung-Ang University Hospital, 102 Heukseok-ro, Dongjak-gu, Seoul 06973, Korea
Tel: +82-2-6299-1564 Fax: +82-2-6298-8351 E-mail: [email protected]
서 론
중심정맥관 삽입은 혈역학적감시, 고삼투압성 약물, 총 비경구영양, 수혈제재 등의 투여의 목적을 가지고 임상적 으로 널리 사용되는 술기 중의 하나이다. 우측 내경정맥은
접근이 용이하여 중심정맥관 삽입 시 첫 번째로 추천되는 곳이다.(1,2) 내경정맥은 많은 해부학적 변이가 있는 것으 로 알려져 있고,(3-6) 이로 인해 중심정맥관 삽입 시 다양 한 합병증이 발생할 수 있다.(4,7,8) 특히 동맥 천자에 의 해 발생한 혈종으로 인한 기도폐쇄의 가능성과 같은 치명
ORIGINAL ARTICLE
J Surg Ultrasound 2017;4:41-47
JSU Journal of Surgical Ultrasound
Fig. 1. Patient positioning for the examination. The head was rotated to the left at ultrasound examinations (A). CT scan was performed with supine position (B).
Fig. 2. Classification of the anato- mical relationship between the internal jugular vein and common carotid artery. The patients were divided into five groups with lateral (A), ante- rolateral (B), anterior, not complete (C), anterior, complete overlap (D) and anteromedial (E). The patients were divided into two groups accor- ding to the safety degree of internal jugular vein cannulation. We have classified group A, B as favorable anatomy for internal jugular vein puncture, and group C, D and E as unfavorable anatomy for puncture.
적 합병증을 고려하였을 때, 내경정맥과 경동맥의 해부학 적 위치관계를 파악하는 것은 안전하고 성공적인 중심정 맥관 삽입에 있어서 중요한 비중을 차지한다고 할 수 있 다.
이러한 이유로, 중심정맥관 삽입 시 내경정맥 천자와 관련된 합병증 예방을 위해서 초음파 유도 천자가 추천된 다.(2,9-13) 초음파 유도 천자에는 두 가지 방법이 있
다.(10) 실시간 초음파 영상을 보면서 바늘을 삽입하는 방 법과 미리 초음파로 천자할 위치를 파악한 후 바늘을 삽입 하는 정적 초음파 유도 천자 방법이 그것이다. 이 중 정적 초음파 유도 천자 방법은 동맥과 정맥의 해부학적 변이 및 위치를 초음파로 확인한 후 실제 바늘의 삽입은 초음파 유 도 없이 이루어진다.
본 연구에서는 초음파 영상과 컴퓨터 단층촬영 (Computed tomography; CT) 영상을 통하여 내경정맥과 경동맥 위치의해부학적 변이를 분석하였고, 실시간 초음 파 유도하 천자가 불가능한 상황에서, 경부 또는 흉부 CT 등의 내경정맥 주변 해부학적 구조를 반영한 영상검사가 있는 경우, 초음파 영상을 대체하여 천자에 사용할 수 있 는지 연구해 보고자 하였다.
방 법
본 연구는 중앙대학교병원 생명윤리위원회의 승인 (IRB No. 1705-010-16074)을 받아 중앙대학교병원에서 2013년 9월부터 2016년 3월까지 수술실에서 우측 내경정 맥을 통하여 피하 터널형 중심정맥도관 삽입술을 시행한 환자 326명에 대해 후향적 연구를 시행하였다. 연구 대상 환자들 중에서 도관 삽입 시 실시간으로 시행한 초음파 영
Fig. 3. Real-time ultrasound image. The central venous catheter insertion was performed while confirming the real-time ultrasound imaging. The ultrasound image was analyzed by hypothetical line passing through the middle of the internal jugular vein to the vertical axis.
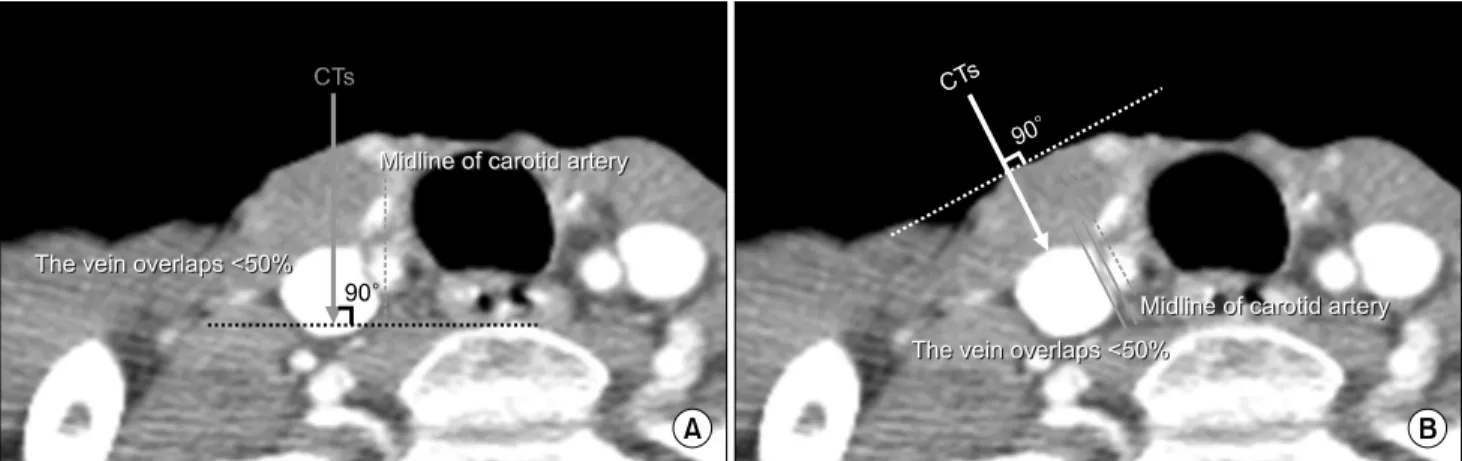
Fig. 4. CT images. The CT images were obtained by connecting a hypothetical line passing through the middle of the internal jugular vein to the vertical axis at ground (CTg, A) and the perpendicular axis to the skin (CTs, B), respectively.
상과 시술 전 경부 주위의 해부학적 구조를 파악할 수 있는 CT 영상이 있는 환자 250명을 선정하여 분석을 시행하였 다. 초음파 영상은 중심정맥 도관 삽입 중 천자에 편리하 게 목을 삽관 위치의 반대쪽으로 돌린 상태에서 천자 중 실시간으로 얻었고, CT 영상은 앙와위로 검사를 시행하 여 얻었다(Fig. 1).
초음파와 CT에서 관찰되는 내경정맥과 경동맥의 상대 적인 위치에 따라 환자들을 5개의 군으로 분류하였다 (Fig. 2).(14) 초음파 영상은 실제 바늘의 삽입 방향과 일 치하는 경로인 내경정맥의 정중앙면에서 수직인 축으로 분석하였다(Fig. 3). CT 영상은 천자 시 해부학적 지표로 이용되는 우측 흉쇄유돌근의 정점이 위치하는 영상면을
찾은 후 내경정맥의 정중앙을 지나는 가상의 선을 지면에 수직인 축으로 연결시킨 것(CTg, Fig. 4A)과 천자 시 피하 조직에 바늘이 지나가는 경로와 일치하는 피부에 수직인 축으로 연결시킨 것(CTs, Fig. 4B)으로 나누어 각각 분석 하였다. 내경정맥과 경동맥의 위치에 따라 총 다섯 개의 군으로 나누었다: A군/내경정맥이 경동맥의 외측에 위치 하는 경우(Fig. 2A); B군/내경정맥이 경동맥과 50% 미만 으로 겹치면서 경동맥의 외측에 위치하는 경우(Fig. 2B);
C군/내경정맥과 경동맥이 50% 이상으로 겹치지나 완전 히 포개지지는 않는 경우(Fig. 2C); D군/내경정맥이 경동 맥을 완전히 덮고 있는 경우(Fig. 2D); E군/내경정맥이 경동맥의 내측에 위치하는 경우(Fig. 2E). 이후 내경정맥 과 경동맥 사이의 상대적 위치관계를 파악하여 내경정맥 천자에 안전한 정도에 따라 두 개의 군으로 분류하였다 (Fig. 2). 내경정맥이 경동맥 옆에 위치하여 정맥 천자가 용이한 A군과 B군은 FA (favorable anatomy) (Fig. 2A, B)로 분류하였고, 경동맥에 내경정맥이 50% 이상 겹쳐져 있거나 일반적으로 알려진 해부학적 위치와 다르게 내경 정맥이 경동맥의 내측에 위치하여 바늘 천자 시에 따른 위 험성이 높은 C군, D군과 E군은 UA (unfavorable anat- omy) (Fig. 2C, D and E)으로 나누었다. 초음파와 각각의 CT 영상에서 FA, UA의 분포의 차이를 비교하였고, CTg 영상과 CTs 영상 사이의 유사성을 분석하였다. 초음파를 기준으로 하여 CT 영상의 타당도를 평가하였다.
통계학적 검증 방법은 명목변수에 대하여는 χ2 검증, 검사간의 차이분석에는 McNemar 검증을 이용하였고, P 값이 0.05 보다 작은 경우를 통계학적으로 의미가 있는 것
Table 1. Demographics of the Study Group
Characteristics Value (N = 250) Age, mean ± SD, years old 61.62 ± 13.44 Gender, n (%)
Female 127 (50.8%)
Male 123 (49.2%)
Underlying disease, n (%)
Colorectal cancer 49 (19.6%)
Breast cancer 38 (15.2%)
Lymphoma 26 (10.4%)
Lung cancer 24 (9.6%)
Leukemia 22 (8.8%)
Stomach cancer 19 (7.6%)
Chronic kidney disease 19 (7.6%)
Etc.* 53 (21.2%)
*Acute renal failure, cervical cancer, cholangiocarcinoma, endometrium cancer, esophagus cancer, kidney cancer, liver cancer, major salivary gland cancer, melanoma, mesothelioma, nasopharyngeal cancer, ovary cancer, pancreas cancer, peritoneal cancer, prostate cancer, retroperitoneal cancer, sarcoma, supraglottis cancer, testis cancer, thymus cancer, ureter cancer, vaginal cancer.
Table 2. Anatomical Location of the Internal Jugular Vein in Relation to the Common Carotid Artery on US and CT Images
Anatomical type Number of patients (%)
US CTg CTs
FA (a) Lateral 16 (6.4%) 21 (8.4%) 2 (0.8%)
(b) Anterolateral 75 (30.0%) 160 (64%) 33 (13.2%)
Total 91 (36.4%) 181 (72.4%) 35 (14.0%)
UA (c) Anterior, not complete 59 (23.6%) 63 (25.2%) 94 (37.6%)
(d) Anterior, complete overlap 100 (40.0%) 6 (2.4%) 121 (48.4%)
(e) Anteromedial 0 (0%) 0 (0%) 0 (0%)
Total 159 (63.6%) 69 (27.6%) 215 (86.0%)
CTg = Vertical axis to the ground on CT; CTs = Perpendicular axis to the skin on CT; FA = Favorable anatomy; UA = Unfavorable anatomy.
으로 하였다. 통계학적 분석에는 IBM SPSS Statistics version 23 (IBM Corp., Chicago, IL, USA)을 사용하였다.
결 과
Table 1에 환자들의 기저특성을 나타내었다. 127명은 남성, 123명은 여성이었으며, 평균 나이는 61.6 ± 13.4년 (범위, 27-91세)이었다. 환자들의 기저 질환으로는 결장직 장암(19.6%), 유방암(15.2%), 림프종(10.4%) 등이 있었다.
Table 2는 초음파 영상과 CT 영상에서 내경정맥과 경동 맥의 해부학적 위치에 따른 환자들의 분포를 나타내었다.
초음파 영상에서 내경정맥이 경동맥의 외측에 위치하는 환자(A군)는 16명(6.4%), 내경정맥이 경동맥과 50% 미만 으로 겹치면서 경동맥의 외측에 위치하는 환자(B군)는 75 명(30.0%), 내경정맥과 경동맥이 50% 이상으로 겹쳐지나 완전히 포개지지 않는 환자(C군)는 59명(23.6%), 내경정 맥이 경동맥을 완전히 덮고 있는 환자(D군)는 100명 (40.0%)이었다. CTg에서는 A군은 21명(8.4%), B군은 160명(64%), C군은 63명(25.2%), D군은 6명(2.4%)이었 고, CTs에서는 각각 2명(0.8%), 33명(13.2%), 94명(37.6%), 121명(48.4%)으로 확인되었다. 천자의 안정성에 따라 분 류하였을 때, 초음파 영상에서 FA군은 91명(36.4%)이었 고, UA군은 159명(63.6%)이었다. CTg에서는 FA와 UA가 각각 181명(72.4%), 69명(27.6%)이었고, CTs에서는 각 각 35명(14.0%), 215명(86.0%)으로 확인되었다.
CTg 영상과 CTs 영상 사이의 유사성을 비교하였을 때, 두 검사 사이에는 통계학적으로 유의한 차이가 있었다(P < 0.001) (Table 3). 또한 초음파 영상과 두 가지의 CT 영상 간의 비교에서도 통계적으로 유의한 차이가 있었다(P < 0.001) (Table 4).
CTg 영상과 초음파 영상을 비교하였을 때, CTg 영상의 FA 중에서 58.6%가 초음파에서는 UA로 관찰되었고, CTg 영상의 UA 중에서 23.2%가 초음파에서는 FA로 관찰 되었다. CTs 영상과 초음파 영상을 비교하여 보면, CTs 영상의 FA 중에서 28.6%는 초음파에서 UA로 관찰되었 고, UA 중에서는 30.7%가 초음파에서 FA로 관찰되었다.
초음파 영상이 천자 시의 실제 해부학적 위치임을 감안 하여, 초음파와 CT 영상을 비교하여 CT의 타당도를 평가 하였을 때, CTg 영상에서는 82.4%의 민감도, 33.3%의 특 이도, 51.2%의 정확도, 41.4%의 양성예측도, 76.8%의 음
Table 4. The Comparison of US and CT Images
On CTg image On CTs image
Total
FA UA FA UA
On US image FA 75 16 25 66 91 (36.4%)
UA 106 53 10 149 159 (63.6%)
Total 181 (72.4%) 69 (27.6%) 35 (14%) 215 (86.0%) 250 (100%)
CTg = Vertical axis to the ground on CT; CTs = Perpendicular axis to the skin on CT; FA = Favorable anatomy; UA = Unfavorable anatomy.
*McNemar test: P < 0.001.
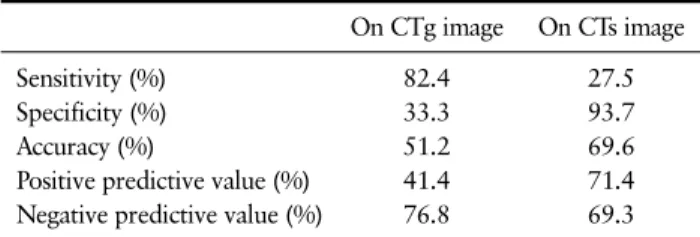
Table 5. The Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value of CT Images
On CTg image On CTs image
Sensitivity (%) 82.4 27.5
Specificity (%) 33.3 93.7
Accuracy (%) 51.2 69.6
Positive predictive value (%) 41.4 71.4 Negative predictive value (%) 76.8 69.3 CTg = Vertical axis to the ground on CT; CTs = Perpendicular axis to the skin on CT.
Table 3. Comparison between Groups on Vertical and Oblique CT Images
On CTs image
Total
FA UA
On CTg image FA 35 146 181
UA 0 69 100
Total 35 215 250
CTg = Vertical axis to the ground on CT; CTs = Perpendicular axis to the skin on CT; FA = Favorable anatomy; UA = Unfavorable anatomy.
*McNemar test: P < 0.001.
성예측도를 가졌으며, CTs 영상은 27.5%의 민감도, 93.7%의 특이도, 69.6%의 정확도, 71.4%의 양성예측도, 69.3%의 음성예측도를 가졌다(Table 5).
고 찰
경동맥에 대한 내경정맥의 상대적 위치는 Fig. 4의 CT 영상에서 제시된 형태와 같이 내경정맥이 경동맥 외측에 위치하는 형태가 가장 일반적으로 알려져 있다. 그러나 내 경정맥을 통한 중심정맥관 삽입 시에는 시술이 용이하게 하기 위해 목을 삽관 위치의 반대쪽으로 돌리게 되는데, 고개를 돌림으로써 내경정맥과 경동맥의 해부학적 위치 는 변하게 되며 두 혈관이 중첩되는 정도가 증가하게 된 다.(15,16) 본 연구에서도 동일한 결과를 얻을 수 있었는 데 Table 4에 나타난 바와 같이 CTg 영상에서 보다 초음파 영상에서 FA 환자의 비율이 적었다. 또한, CTg와 초음파 를 비교하였을 때 유의한 차이가 있었고 CTg 영상의 FA 중에서 58.6%가 초음파 상 UA에 해당되었다. CTg 영상 은 고개를 돌리지 않고 얻은 영상이므로 실제 중심정맥관 삽입시의 해부학적 구조라고 할 수 있는 초음파 영상과 큰 차이가 있어서 초음파 영상을 CTg 영상으로 대체하여 사
용하기에는 위험성이 크다고 할 수 있다.
Table 3에서 확인할 수 있듯이 CTs와 CTg 영상사이에 도 통계적으로 유의한 차이가 있었다. 앙와위에서 얻은 CTg 영상의 제한점을 극복하고자 고개를 돌린 상황과 유 사한 CTs방법으로 해부학적 변이를 분석하였으나 table 4 에서와 같이 CTs 영상은 초음파 영상과 통계학적으로 의 미 있는 차이가 있었다. 또한 CTs 영상의 FA 중에서 28.6%는 초음파에서 UA로 관찰되었고, CTs 영상의 UA 중에서는 30.7%가 초음파에서 FA로 관찰되었다. 따라서 CTs 영상이 실제로 고개를 돌림으로써 발생하는 내경정 맥과 경동맥의 위치 변화를 온전하게 반영하지 못한다고 볼 수 있다.
CTg와 CTs 영상의 민감도, 특이도와 정확도를 중심정 맥관 삽입 시 실시간 초음파 영상에서 확인된 구조와 비교 하여 계산하였다. CTs의 경우 비교적 높은 특이도를 가졌 지만, 이는 실제 UA를 가진 환자 중 검사를 통해 UA를 가 려낼 수 있지만 민감도가 너무 낮아서 실제 임상에서 사용 하기에는 제한점이 존재한다. 또한 CTg와 CTs 모두 높지 않은 정확도, 양성예측도와 음성예측도를 나타내므로 시 술 전 CT 영상 만으로 천자를 시도하는 것에는 위험성이 따를 수 있다. 따라서 내경정맥을 통하여 중심정맥관 삽입 을 시도할 경우에는 초음파 유도 하에 천자를 시행하는 것
이 보다 안전한 중심정맥관 삽관에 도움이 될 것이다.
본 연구의 제한점으로는 내경정맥의 해부학적 변이에 따른 중심정맥관 삽입과 관련된 합병증 발생률에 대한 분 석이 없었다는 것이다. 본 연구에 대상이 된 환자들은 모 두 실시간 초음파 유도 하에 천자를 시행하였기 때문에 경 동맥 천자와 같은 합병증은 발생하지 않았다. 두 번째 제 한점으로는, 본 연구에 대상이 되는 환자 대부분이 암환자 로 구성되어 있어 다른 장기로의 전이 여부를 판단하기 위 한 경부 주위 CT 영상이 확보되어 있었지만, 실제 내경정 맥 천자가 필요한 환자들은 중심정맥관 삽입 시술 전 CT 검사가 시행되지 않는 경우가 대부분이므로, 이런 면에 있 어서 실제로 임상에 적용하는 것에는 한계가 있을 수 있다 는 것이다. 세 번째 제한점으로는, 초음파 영상과 CT 영상 의 더 정확한 비교를 위해서는 실제 천자할 때처럼 고개를 돌린 상태에서 촬영한 CT 영상에 대한 분석이 필요하다는 것이다. 그러나 연구만을 위한 추가적인 CT 촬영을 진행 하는 데에는 현실적인 어려움이 있다.
그러나 본 연구는, 국내의 환자를 대상으로 처음 연구 가 시행되었다는 점에서 의의가 있고, 고개를 돌린 상태인 실제 천자 시 상태를 기준으로 내경정맥의 해부학적 변이 를 분석하였다. 더불어, 고개를 돌릴 때 해부학적인 위치 변화가 생긴다는 것을 영상의학적 검사간의 통계학적 분 석을 통해 다시 확인할 수 있었다.
결 론
경부 주위의 CT 영상은 내경정맥의 해부학적 변이에 대 한 정보를 제한적으로 얻을 수 있지만, 천자 시 고개를 돌 리게 되면 내경정맥과 경동맥의 해부학적인 위치변화가 생기면서 중첩이 심해지는 경우가 증가한다. 두 혈관의 상 호 위치에 해부학적 변이가 많이 관찰되므로 내경정맥을 통하여 중심정맥관 삽입을 시도할 경우에는 해부학적 변 이에 유의해야 할 필요가 있다.
REFERENCES
1. Sznajder JI, Zveibil FR, Bitterman H, Weiner P, Bursztein S. Central vein catheterization. Failure and complication rates by three percutaneous approaches.
Arch Intern Med 1986;146:259-61.
2. Dietrich CF, Horn R, Morf S, Chiorean L, Dong Y, Cui XW, et al. Ultrasound-guided central vascular inter-
ventions, comments on the European Federation of Societies for Ultrasound in Medicine and Biology guidelines on interventional ultrasound. J Thorac Dis 2016;8:E851-68.
3. Troianos CA, Jobes DR, Ellison N. Ultrasound-guided cannulation of the internal jugular vein. A pro- spective, randomized study. Anesth Analg 1991;72:
823-6.
4. Lin BS, Kong CW, Tarng DC, Huang TP, Tang GJ.
Anatomical variation of the internal jugular vein and its impact on temporary haemodialysis vascular ac- cess: an ultrasonographic survey in uraemic patients.
Nephrol Dial Transplant 1998;13:134-8.
5. Lichtenstein D, Saïfi R, Augarde R, Prin S, Schmitt JM, Page B, et al. The Internal jugular veins are asymmetric. Usefulness of ultrasound before cathe- terization. Intensive Care Med 2001;27:301-5.
6. Lim CL, Keshava SN, Lea M. Anatomical variations of the internal jugular veins and their relationship to the carotid arteries: a CT evaluation. Australas Radiol 2006;50:314-8.
7. McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med 2003;
348:1123-33.
8. Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical land- marks for internal jugular vein catheterization.
Cochrane Database Syst Rev 2015;1:CD006962.
9. American Society of Anesthesiologists Task Force on Central Venous Access, Rupp SM, Apfelbaum JL, Blitt C, Caplan RA, Connis RT, et al. Practice guidelines for central venous access: a report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology 2012;116:539-73.
10. Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD, et al. Guidelines for per- forming ultrasound guided vascular cannulation: rec- ommendations of the American Society of Echocardi- ography and the Society of Cardiovascular Anes- thesiologists. J Am Soc Echocardiogr 2011;24:1291- 318.
11. Wu SY, Ling Q, Cao LH, Wang J, Xu MX, Zeng WA.
Real-time two-dimensional ultrasound guidance for central venous cannulation: a meta-analysis. Anes- thesiology 2013;118:361-75.
12. Karakitsos D, Labropoulos N, De Groot E, Patrianakos AP, Kouraklis G, Poularas J, et al.
Real-time ultrasound-guided catheterisation of the internal jugular vein: a prospective comparison with the landmark technique in critical care patients. Crit Care 2006;10:R162.
13. Hind D, Calvert N, McWilliams R, Davidson A, Paisley S, Beverley C, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ 2003;327:361.
14. Umaña M, García A, Bustamante L, Castillo JL,
Sebastián Martínez J. Variations in the anatomical relationship between the common carotid artery and the internal jugular vein: an ultrasonographic study.
Colomb Med (Cali) 2015;46:54-9.
15. Kim WH, Gwak MS, Choi SJ, Song SH, Kim MH.
Optimal head rotation and puncture site for internal
jugular vein cannulation after laryngeal mask airway insertion. Singapore Med J 2015;56:472-8.
16. Sulek CA, Gravenstein N, Blackshear RH, Weiss L.
Head rotation during internal jugular vein cannula- tion and the risk of carotid artery puncture. Anesth Analg 1996;82:125-8.