JSUJournal of Surgical Ultrasound
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치

관련 문서
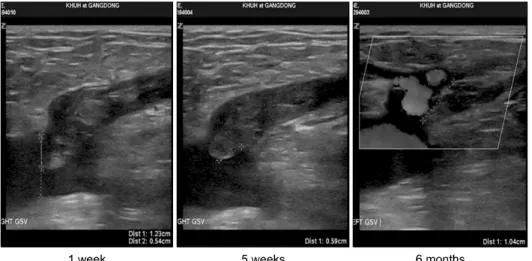
When the glue was injected across a joint, an inflammatory reaction developed in the vein wall as well as the surrounding tissue.. It may be assumed that cyanoacrylate glue
A total of 200 limbs in 148 patients underwent RFA. All saphenous veins with reflux ≥0.5 second were ablated.. Occlusion rate of saphenous vein. Kaplan-Meier analysis showed
