동정맥루 수술에서 초음파를 이용한 상완신경총 차단과 동 , 정맥 평가
대구가톨릭대학교 의과대학 외과학교실, 1의학통계학교실
이재훈, 박기혁, 곽상규1
Brachial Plexus Block and Vascular Evaluation Used Ultrasound in Arteriovenous Access Surgery
Jae Hoon Lee, Ki Hyuk Park, Sang Gyu Kwak
1Departments of Surgery,
1Medical Statistics, College of Medicine, Daegu Catholic University, Daegu, Korea
Received August 8, 2016 Revised August 18, 2016 Accepted August 30, 2016
Purpose: Brachial plexus block (BPB) promotes vasodilation of the upper extremities be-
cause of a sympathectomy-like effect. We investigated changes in the arteries and veins of the upper extremities after BPB, the factors affecting the vascular change of vessels and the relations with the patency of vascular access.Methods: From September 2015 to February 2016, 49 patients evaluable by ultra-
sonography were included this study. The arteries and veins were examined prospectively before and after BPB at the wrist, cubital fossa and axilla fossa. A two sample t-test and paired t-test were used for statistical analyses.Results: The mean age of the patients was 63.08 ± 14.23 years and the percentage of males
was 67.3%. Artificial grafts were used in 23 patients (46.9%), supraclavicular BPB in 37 pa- tients and axillary BPB in 12 patients. All vessels except axillary arteries increased sig- nificantly after BPB. In diabetic patients, changes in brachial arteries, brachial veins and axil- lary veins less increased (P = 0.04, 0.015 and 0.011). The level of anesthesia is most com- mon to C7 dermatome after BPB (65%). The mean last follow-up period was 66.78 ± 52.50 days. Vascular access was occluded in four patients. The vascular access patency was not re- lated to the sizes and changes in vessels. No other complications associated with BPB proce- dures were not noted except for phrenic nerve palsy in one patient.Conclusion: BPB employing ultrasound was found to be an effective and safe procedure that
could improve venous dilation and absence of arterial spasm in vascular access surgery.However, caution may be necessary in selecting veins for vascular access in diabetic patients having less venous dilatation.
Keywords: Brachial plexus anesthesia, Arteriovenous fistula, Ultrasound
Correspondence to:Ki Hyuk Park
Division of Vascular and Endovascular Surgery, Department of Surgery, College of Medicine, Daegu Catholic University, 33, Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea
Tel: +82-53-650-4053 Fax: +82-53-624-7185 E-mail: [email protected]
서 론
의료 발전으로 인한 인구의 고령화와 더불어 당뇨와 고 혈압과 같은 성인병의 증가로 말미암아 우리나라 말기신
부전 환자는 꾸준히 증가하고 있다. 말기신부전 환자의 신 대체요법인 투석요법은 신장기능을 대신하여 수십 년 이 상 유지할 수 있는 보편화된 치료법이다. 이중 복막투석환 자 수는 큰 변화가 없는 반면, 혈액투석환자 수는 매년 약
ORIGINAL ARTICLE
J Surg Ultrasound 2016;3:35-39
JSU Journal of Surgical Ultrasound
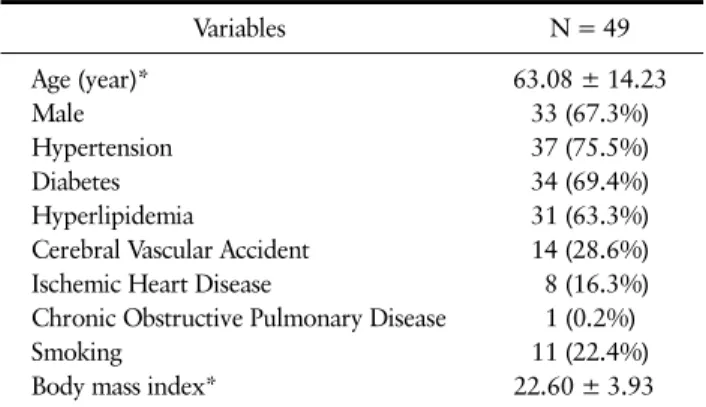
Table 1. Patients’ Clinical Characteristics
Variables N = 49
Age (year)* 63.08 ± 14.23
Male 33 (67.3%)
Hypertension 37 (75.5%)
Diabetes 34 (69.4%)
Hyperlipidemia 31 (63.3%)
Cerebral Vascular Accident 14 (28.6%)
Ischemic Heart Disease 8 (16.3%)
Chronic Obstructive Pulmonary Disease 1 (0.2%)
Smoking 11 (22.4%)
Body mass index* 22.60 ± 3.93
Values are presented as number (%).
*Expressed as mean ± SD.
Table 2. Details of Anesthesia and Operation
Variables N = 49
Brachial plexus block
Resident/Professor 25/24
Supraclavicular/Axillary 37/12
Mepivacaine dose (mg)* 430.71 ± 88.74
Level (C6/C7/C8/T1) 6/32/10/1
Operation
Left / Right 42/7
Autologous vein/ Artificial graft 26/23 Values are presented as number (%).
*Expressed as mean ± SD.
5-8% 증가하여 2011년 말 기준 전체 투석환자의 84.7%를 차지하고 있다.(1) 장기적인 혈액투석을 위해서는 동정맥 루(arteriovenous fistula) 수술이 필수적이다. 동정맥루 수술시 마취방법은 국내에서 일반적으로 이용되는 국소 마취(local anesthesia), 미국에서 85.2% (2) 차지하며 주 로 이용되는 전신마취(general anesthesia), 본 연구에서 말하고자 하는 상완신경총 차단(brachial plexus block) 을 통한 부분마취(regional anesthesia)로 구분된다.
이중 상완신경총 차단은 교감신경절제술(sympathec- tomy) 같은 효과로 정맥의 크기를 증가시키고,(3,4) 요골 동맥(radial artery)과 동정맥루 혈류를 증가시켜(5) 동정 맥루의 자가혈관 사용비율을 향상 시킨다고 알려져 있 다.(6) 이 연구에서는 본원에서 동정맥루 수술시 주로 이 용되는 초음파를 통한 상완신경총 차단후 동, 정맥의 크기 변화를 조사하고 변화에 영향을 미치는 인자, 나아가 동정 맥루 폐쇄와 연관성을 알고자 한다.
방 법
2015년 9월부터 2016년 2월까지 본원에서 동정맥루 수 술시 초음파를 통해 평가가능했던 49명의 환자를 대상으 로 하였다. 초음파를 통해 상완신경총 차단 전, 후로 동, 정맥의 크기를 손목, 팔오금(cubital fossa), 겨드랑이 세 부분으로 나누어 각각 측정해 차이를 비교 하였다.
상완신경총 차단방법은 초음파와 신경 자극기(stimuplex Dig RC Nerve Stimulator, B. Braun Malaysia, Costa Mesa, California, United States)를 같이 이용한 듀얼
모니터링(dual monitioring) 방법을 이용해 시행하였다.
마취제로는 메피바카인(mepivacaine)을 이용하였고 마 취부위는 쇄골위(supraclavicular) 또는 겨드랑이(axillary) 상완신경총을 차단하였다. 동, 정맥 크기 측정과 상완신 경총 차단시 이용된 초음파는 ProSound Alpha 7 (Hitachi, Tokyo, Japan), 3.6-12.3 MHz 프로브(UST-5412, lin- ear, 36 mm Width)를 사용하였다.
통계학적 분석은 SPSS 18.0 (SPSS, Chicago, IL, USA)를 사용하였으며, 통계학적 검증은 two sample t-test, paired t-test를 이용하였고 P-value < 0.05인 경우 통 계학적으로 의의가 있는 것으로 하였다.
결 과
1. 환자의 임상적 특징(Table 1)
환자의 평균 나이는 63.08 ± 14.23세였고 남자가 67.3%
를 차지하였다. 동반질환으로는 고혈압(75.5%), 당뇨 (69.4%), 고지혈증(63.3%) 순으로 높게 나타났고 흡연력 (22.4%), 신체질량지수(body mass index)는 22.60 ± 3.93로 나타났다.
2. 마취와 수술의 세부사항(Table 2)
마취자가 교수, 전공의 경우가 각각 25례, 24례로 비슷 한 비율로 나타났고 쇄골위 상완신경총 차단이 37례로 겨 드랑이 차단(12례)에 비해 3배정도 많이 시술되었다. 사 용된 메피바카인의 평균용량은 430.71 ± 88.74 mg로 조 사되었고 마취 후 감각마비에 따른 피부분절(dermatome) 은 제7목신경(cervical nerve 7)까지 마비된 경우가 32례 로 다수를 차지하였다.
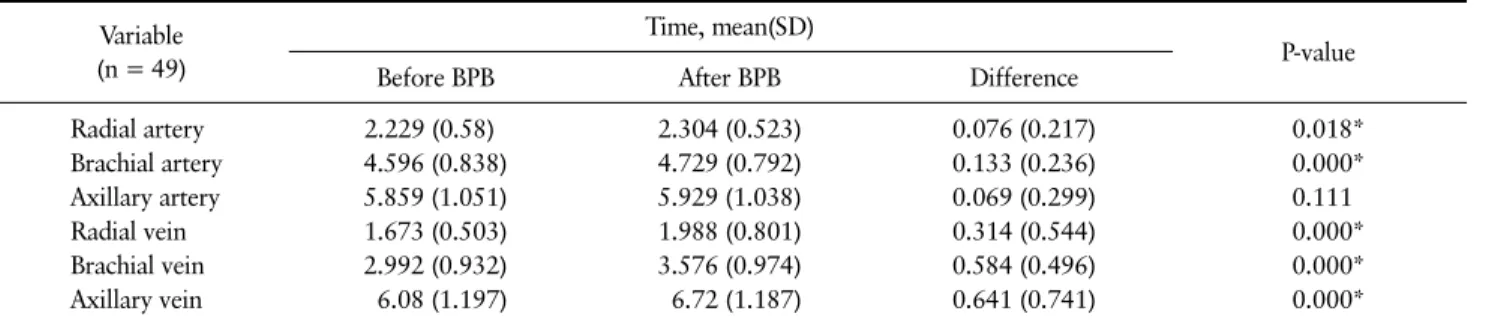
Table 3. Changes of Arteries and Veins Before/After Brachial Plexus Block (BPB) Variable
(n = 49)
Time, mean(SD)
P-value
Before BPB After BPB Difference
Radial artery 2.229 (0.58) 2.304 (0.523) 0.076 (0.217) 0.018*
Brachial artery 4.596 (0.838) 4.729 (0.792) 0.133 (0.236) 0.000*
Axillary artery 5.859 (1.051) 5.929 (1.038) 0.069 (0.299) 0.111
Radial vein 1.673 (0.503) 1.988 (0.801) 0.314 (0.544) 0.000*
Brachial vein 2.992 (0.932) 3.576 (0.974) 0.584 (0.496) 0.000*
Axillary vein 6.08 (1.197) 6.72 (1.187) 0.641 (0.741) 0.000*
*Statistically significant with P < 0.05.
Table 4. Changes of Vessels With/Without Diabetes Mellitus (DM) Variable
(n = 49) Factor Time, mean (SD)
P-value
Before BPB After BPB Difference
Radial artery DM - 2.26 (0.445) 2.32 (0.404) 0.06 (0.196) 0.743
+ 2.215 (0.636) 2.297 (0.573) 0.082 (0.228)
Brachial artery DM - 4.413 (1.151) 4.687 (1.095) 0.273 (0.162) 0.004*
+ 4.676 (0.661) 4.747 (0.634) 0.071 (0.238)
Axillary artery DM - 5.76 (1.002) 5.787 (0.972) 0.027 (0.42) 0.512
+ 5.903 (1.083) 5.991 (1.075) 0.088 (0.232)
Radial vein DM - 1.78 (0.632) 2.1 (0.84) 0.32 (0.393) 0.962
+ 1.626 (0.437) 1.938 (0.792) 0.312 (0.604)
Brachial vein DM - 3.02 (1.005) 3.86 (0.929) 0.84 (0.59) 0.015*
+ 2.979 (0.913) 3.45 (0.98) 0.471 (0.408)
Axillary vein DM - 5.487 (1.055) 6.527 (1.222) 1.04 (0.782) 0.011*
+ 6.341 (1.175) 6.806 (1.179) 0.465 (0.66)
*Statistically significant with P < 0.05.
3. 마취 전, 후의 동, 정맥 변화(Table 3)
액와동맥을 제외하고 측정된 요골동맥, 상완동맥, 요골 정맥, 상완정맥, 액와정맥은 마취후 의미있는 크기 변화 (P < 0.005)를 보였고 동맥보단 정맥에서 원위부보단 근 위부에서 더 큰 변화를 보였다.
4. 당뇨 유무에 따른 동, 정맥 변화(Table 4)
환자의 임상적 특징에 따른 동, 정맥 변화를 통계학적 으로 분석했을 때 당뇨환자에서 상완동맥, 상완정맥, 액 와정맥이 당뇨가 없는 환자에 비해 증가 폭이 의미있게 적 었다.5. 합병증, 동정맥루 폐쇄 및 미성숙
환자의 평균 추적관찰 기간은 66.78 ± 52.50일였고,
술기와 관련된 합병증으로는 1례에서 횡경신경 마비가 관 찰되었다. 호흡곤란과 산증이 관찰되었으나 대증적 치료 후 증상없이 회복되었다. 이외 합병증은 없었다.
추적기간 동안 2례에서 동정맥루 폐쇄가 있었고, 2례에 서 동정맥루 미성숙으로 인한 투석이 불가능 하였다. 2례 의 동정맥루 폐쇄는 모두 인조혈관을 이용한 상완동맥- 액와정맥 동정맥루였다. 동정맥루 폐쇄시 정맥의 크기가 가장 중요한 인자이므로 인조혈관을 이용한 상완동맥-액 와정맥 동정맥루 시행한 18례중 폐쇄가 된 2례와 원활한 흐름을 가지는 16례의 액와정맥의 크기를 비교하였다 (Table 5). 폐쇄된 경우가 액와정맥의 크기도 작고 크기 변 화도 작았으나 의미 있는 변화를 보이지 않았다(P = 0.508).
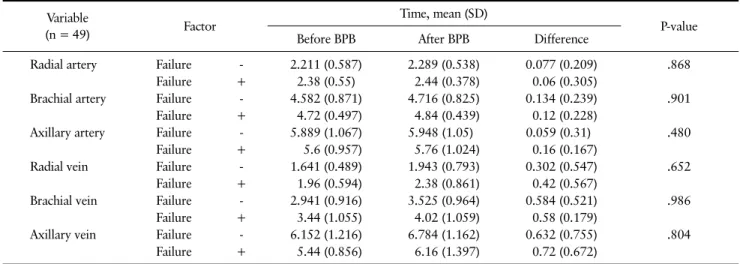
폐쇄와 미성숙되어 정상적인 기능을 하지 못하는 동정 맥루 4례와 정상적인 기능을 가지는 동정맥루 45례의 동, 정맥 크기변화를 비교했을 때 의미 있는 차이는 없었다
Table 6. Changes of Vessels Vein With/Without Graft Failure Variable
(n = 49) Factor Time, mean (SD)
P-value
Before BPB After BPB Difference
Radial artery Failure - 2.211 (0.587) 2.289 (0.538) 0.077 (0.209) .868
Failure + 2.38 (0.55) 2.44 (0.378) 0.06 (0.305)
Brachial artery Failure - 4.582 (0.871) 4.716 (0.825) 0.134 (0.239) .901
Failure + 4.72 (0.497) 4.84 (0.439) 0.12 (0.228)
Axillary artery Failure - 5.889 (1.067) 5.948 (1.05) 0.059 (0.31) .480
Failure + 5.6 (0.957) 5.76 (1.024) 0.16 (0.167)
Radial vein Failure - 1.641 (0.489) 1.943 (0.793) 0.302 (0.547) .652
Failure + 1.96 (0.594) 2.38 (0.861) 0.42 (0.567)
Brachial vein Failure - 2.941 (0.916) 3.525 (0.964) 0.584 (0.521) .986
Failure + 3.44 (1.055) 4.02 (1.059) 0.58 (0.179)
Axillary vein Failure - 6.152 (1.216) 6.784 (1.162) 0.632 (0.755) .804
Failure + 5.44 (0.856) 6.16 (1.397) 0.72 (0.672)
*Statistically significant with P < 0.05.
Table 5. Changes of Axillary Vein With/Without Graft Occlusion Variable
(n = 18) Factor Time, mean (SD)
P-value
Before BPB After BPB Difference
Axillary vein Occlusion - 6.237 (1.258) 6.800 (1.354) 0.562 (0.735) 0.508
+ 4.750 (0.354) 4.950 (0.212) 0.200 (0.141)
*Statistically significant with P < 0.05.
(Table 6).
고 찰
국소 마취는 조직 부종을 일으켜 전기 소작기의 효과를 감소시키고 감염의 가능성을 증가시킨다. 반복적인 국소 마취시 혈관경련을 일으키고 몸무게에 따른 사용량의 한 계가 있다.(6) 전신 마취는 만성신부전 환자의 경우 심각 한 질환을 동반한 경우가 많아(7) 전신 마취과 관련된 합 병증의 위험성이 높다.(8-10) 반면 상완신경총 차단의 경 우 전신 마취의 위험성을 감소시키고 국소마취의 단점을 극복할 뿐만 아니라 혈관경련을 감소시키고 감각신경의 차단과 더불어 운동신경도 차단되어 보다 용이하게 수술 을 진행할 수 있다. 상완신경총 차단시 기흉, 혈종, 혈관내 마취제 주입, 신경 손상, 횡경막 신경마비, 호너 증후군 (Horner’s syndrome)과 같은 시술과 관련된 합병증을 일 으킬 수 있다. 최근 여러 무작위 대조 시험(randomized controlled trial)과 메타 분석(meta-analysis)에서 초음 파를 통한 상완신경총 차단이 신경자극기를 이용한 상완
신경총 차단에 비해 마취가 빨리 되고 오래 지속되며 성공 률이 높아 합병증 없이 유용하게 이용된다고 알려져 있 다.(11-13) 본 연구에서는 상완신경총 차단시 초음파 뿐 만 아니라 신경 자극기를 이용하여 마취와 관련된 합병증 없이 보다 안전하게 성공률을 높여 유용한 마취방법으로 이용될 수 있을 것이다.
본 연구에서는 앞선 여러 연구와 마찬가지로 상완신경 총 차단후 동맥의 혈관경련을 막고 정맥의 크기를 의미 있 게 증가시켰다.(3,6,14) 혈관의 증가는 박동 지수를 감소 시키고(4), 요골동맥과 동정맥루의 혈류 흐름을 증가시킨 다.(5) 이런 효과는 말기신부전 환자의 수술원칙인 원위 부, 자가혈관을 사용하는 혈액투석 임상 진료 지침 (hemodialysis clinical practice guidelines)에 부합한 다.(15,16) 자가혈관이 인조혈관이 비해 장기간 개존율이 좋고 합병증이 적은 것으로 보고된다.(17,18) 상완신경총 차단후 혈관의 증가는 수술부위를 원위부 또는 자가혈관 으로 수술의 변화가 17%-44%까지 나타났다.(3,6,19,20) 후향적 리뷰 논문은 수술전 정맥의 크기가 동정맥루의 성숙의 가장 의미 있는 인자라고 소개한다.(21) 본 연구에
서 당뇨환자에서 상완 정맥, 액와 정맥에서 크기증가가 의 미있게 적게 나타났고 이 결과는 당뇨환자가 동정맥루 실 패의 주요인자라는 최근 논문(22,23)과 관련성이 있다.
당뇨환자는 정맥의 크기변화가 적고 이것이 동정맥루의 실패의 원인이 될 수 있음을 나타낸다.
결 론
초음파를 통한 상완총 차단은 동정맥루 수술시 안전하 고 효과적인 마취방법이다. 상완총 차단은 동맥의 혈관경 련과 정맥의 확장을 시켜 수술시 보다 원위부에, 자가혈관 으로 수술할 수 있는 기회를 제공하는 장점을 가진다. 당 뇨환자의 경우 정맥확장이 적기 때문에 충분한 평가 후 수 술하는 것이 동정맥루 실패를 막을 수 있을 것이다.
REFERENCES
1. Jin DC. Current status of dialysis therapy in Korea.
Korean J Intern Med 2011;26:123-31.
2. Siracuse JJ, Gill HL, Parrack I, Huang ZS, Schneider DB, Connolly PH, et al. Variability in anesthetic con- siderations for arteriovenous fistula creation. J Vasc Access 2014;15:364-9.
3. Laskowski IA, Muhs B, Rockman CR, Adelman MA, Ranson M, Cayne NS, et al. Regional nerve block al- lows for optimization of planning in the creation of arteriovenous access for hemodialysis by improving superficial venous dilatation. Ann Vasc Surg 2007;
21:730-3.
4. Lo Monte AI, Damiano G, Mularo A, Palumbo VD, Alessi R, Gioviale MC, et al. Comparison between lo- cal and regional anesthesia in arteriovenous fistula creation. J Vasc Access 2011;12:331-5.
5. Sahin L, Gul R, Mizrak A, Deniz H, Sahin M, Koruk S, et al. Ultrasound-guided infraclavicular brachial plexus block enhances postoperative blood flow in ar- teriovenous fistulas. J Vasc Surg 2011;54:749-53.
6. Reynolds TS, Kim KM, Dukkipati R, Nguyen TH, Julka I, Kakazu C, et al. Pre-operative regional block anesthesia enhances operative strategy for arterio- venous fistula creation. J Vasc Access 2011;12:336- 40.
7. Solomonson MD, Johnson ME, Ilstrup D. Risk factors in patients having surgery to create an arteriovenous fistula. Anesth Analg 1994;79:694-700.
8. Weissman C. The metabolic response to stress: an overview and update. Anesthesiology 1990;73:308-27.
9. Seltzer JL. Is regional anesthesia preferable to gen- eral anesthesia for outpatient surgical procedures on
an upper extremity? Mayo Clin Proc 1991;66:544-7.
10. Eldredge SJ, Sperry RJ, Johnson JO. Regional anes- thesia for arteriovenous fistula creation in the fore- arm: a new approach. Anesthesiology 1992;77:1230-1.
11. Qin Q, Yang D, Xie H, Zhang L, Wang C. Ultrasound guidance improves the success rate of axillary plexus block: a meta-analysis. Braz J Anesthesiol 2016;66:
115-9.
12. Liu GY, Chen ZQ, Jia HY, Dai ZG, Zhang XJ. The technique comparison of brachial plexus blocks by ul- trasound guided with blocks by nerve stimulator guided. Int J Clin Exp Med 2015;8:16699-703.
13. Singh S, Goyal R, Upadhyay KK, Sethi N, Sharma RM, Sharma A. An evaluation of brachial plexus block using a nerve stimulator versus ultrasound guidance:
a randomized controlled trial. J Anaesthesiol Clin Pharmacol 2015;31:370-4.
14. Shemesh D, Olsha O, Orkin D, Raveh D, Goldin I, Reichenstein Y, et al. Sympathectomy-like effects of brachial plexus block in arteriovenous access surgery.
Ultrasound Med Biol 2006;32:817-22.
15. Centers for Medicare and Medicaid Services, Kinney R. 2005 annual report: ESRD clinical performance measures project. Am J Kidney Dis 2006;48:S1-106.
16. Tordoir J, Canaud B, Haage P, Konner K, Basci A, Fouque D, et al. EBPG on vascular access. Nephrol Dial Transplant 2007;22 Suppl2:ii88-117.
17. Perera GB, Mueller MP, Kubaska SM, Wilson SE, Lawrence PF, Fujitani RM. Superiority of autogenous arteriovenous hemodialysis access: maintenance of function with fewer secondary interventions. Ann Vasc Surg 2004;18:66-73.
18. Huber TS, Carter JW, Carter RL, Seeger JM. Patency of autogenous and polytetrafluoroethylene upper ex- tremity arteriovenous hemodialysis accesses: a sys- tematic review. J Vasc Surg 2003;38:1005-11.
19. Schenk WG 3rd. Improving dialysis access: regional anesthesia improves arteriovenous fistula prevalence.
Am Surg 2010;76:938-42.
20. Renaud CJ, Leong CR, Bin HW, Wong JC. Effect of brachial plexus block-driven vascular access planning on primary distal arteriovenous fistula recruitment and outcomes. J Vasc Surg 2015;62:1266-72.
21. Lauvao LS, Ihnat DM, Goshima KR, Chavez L, Grues- sner AC, Mills JL Sr. Vein diameter is the major pre- dictor of fistula maturation. J Vasc Surg 2009;49:
1499-504.
22. Eslami MH, Zhu CK, Rybin D, Doros G, Siracuse JJ, Farber A. Simple predictive model of early failure among patients undergoing first time arteriovenous fistula creation. Ann Vasc Surg 2016;35:46-52.
23. Kim SM, Han Y, Kwon H, Hong HS, Choi JY, Park H, et al. Impact of a preoperative evaluation on the out- comes of an arteriovenous fistula. Ann Surg Treat Res. 2016;90:224-30.