서 론
미국의학연구원(Institute of Medicine, 이하 IOM)이 1999 년 발간한 보고서 ‘To Err is Human’에서 환자안전(patient safety)에 대한 의약품 사용오류(medication error)의 심각 성, 예방을 위한 체계적인 시스템 구축 및 활성화를 강조한 이후로,
1)의약품 사용오류에 대한 관심이 크게 증가하였으 며, 우리나라에서도 2007년 보건복지부의 ‘의약품 사용 과오 (medication error) 예방을 위한 가이드라인’을 발간하고, 2012 년 한국의약품안전관리원(Korea Institute of Drug Safety &
Risk Management)을 설립하고 의약품이상사례보고시스템 을 통해 의약품 관련 유해사례 등의 체계적인 관리 시스템을 구축해 왔으며, 의약품 안전사고에 대한 사회적 인식과 관련 연구의 필요성이 증가하고 있다.
2)식품의약품안전처의 보고서에 따르면, 의약품 사용오류는
“보건의료인, 환자, 또는 소비자의 관리하에 일어나는 의약
품과 관련된 예방이 가능한 모든 부적절한 사용으로, 환자에 게 위해(harm)를 발생시킬 수 있는 경우와 아닌 경우를 모두 포함한다”로 정의된다.
3)국내외 의약품 사용오류에 대한 정 의를 제시한 환자 안전 관련 기관 기관들이 사용하고 있는 의 약품 사용오류의 분류유형은 크게 심각도(severity), 절차(pro- cess), 행위(activity) 및 주체(responsible person)에 따른 분 류로 구분할 수 있으며, 보건복지부에서는 심각도 및 행위에 의한 분류기준을 제시하고 있다.
4,5)의약품 사용오류에 대한 체계적이고 효과적인 예방 및 문제해결을 위해서는 의약품 사용오류에 대한 현황 파악이 우선되어야 하며, 이를 위해서 는 표준화된 정의와 합리적인 분류체계 마련이 선행되어야 한 다. 이에 본 연구에서는 문헌고찰을 통해 국외의 선행연구들 이 의약품 사용오류에 대한 어떤 분류체계를 사용하고 있는 지를 분석 및 고찰하고, 전문가 임상자문을 통해 우리나라에 서 사용하기에 적합한 의약품 사용오류의 분류유형에 대해 검토하고 제안하고자 한다.
Types of Medication Error to Be Used in Korea
Hyungtae Kim
1, Hye Duck Choi
2, Siin Kim
1, Sola Han
1, Iyn-Hyang Lee
2, and Hae Sun Suh
11College of Pharmacy, Pusan National University, Busan, Korea
2College of Pharmacy, Yeungnam University, Gyeongsan, Korea
의약품 사용 오류
부산대학교 약학대학1, 영남대학교 약학대학2
김형태
1·최혜덕
2·김시인
1·한솔아
1·이인향
2·서혜선
1Received May 11, 2017 Revised May 23, 2017 Accepted May 30, 2017 Address for Correspondence:
Hae Sun Suh College of Pharmacy, Pusan National University, 2 Busandaehak-ro 63beon-gil, Geumjeong-gu, Busan 46241, Korea Tel: +82-51-510-2528
Fax: +82-51-513-6754 E-mail: [email protected]
Objectives:
To explore prevalently used types of medication error and the types of medication er- ror which would be appropriate to be used in Korea.
Methods:In depth literature review was per- formed to explore the mostly used types of medication error in the United States, Canada, Europe, Australia, and Japan. We intended to examine experts’ view on the suitability of the types of medi- cation error to be used in Korea. The types of medicati0on error were classified by activity criteria, severity criteria, process criteria, and responsible person criteria based on literature reviews.
Re- sults:According to the result of literature review, activity criteria was the most commonly used type of medication error. Ten experts in the area of patient-safety and medication error responded and the top two types of medication error which were appropriate and suitable to be used in Korea were severity criteria and activity criteria.
Conclusion:Severity criteria and activity criteria could be recommended to be used as the standard types of medication error in Korea although there are oth- er types of criteria such as process criteria and responsible person criteria.
Key Words
Medication errors · Patient safety.
J Health Tech Assess 2017;5(1):31-41 ISSN 2288-58111 Copyright © 2017 The Korean Association for Health Technology Assessment Review Article
JoHTA
방 법
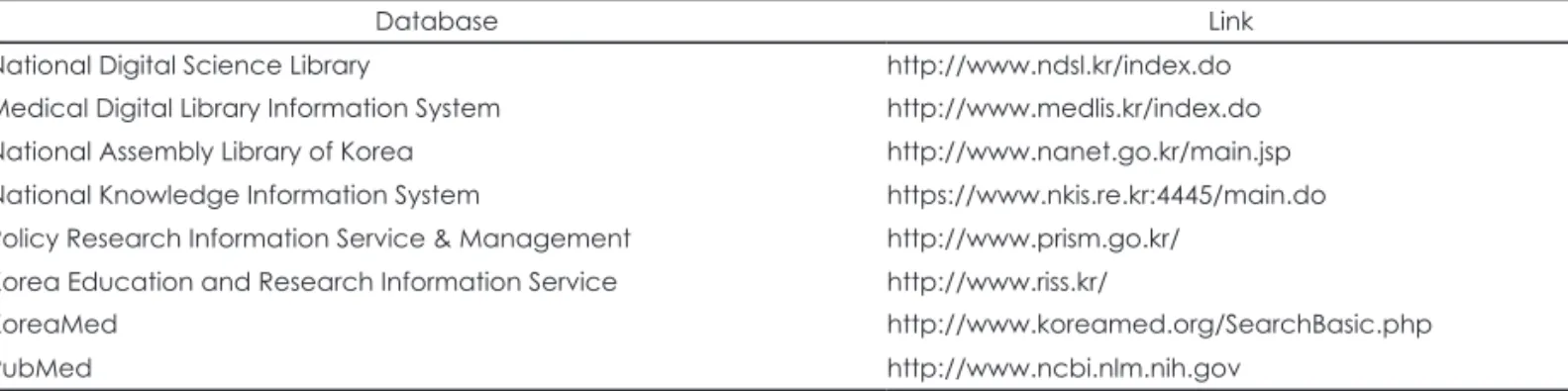
의약품 사용오류에 대한 국외의 선행연구들이 어떤 분류를 사용하고 있는지 분석 및 고찰하기 위해 문헌 검색을 수행 하였다. 검색에 사용된 자료원은 표 1과 같으며, 영문 검색어
“patient safety”, “medication error”, “Incidence”, “preva - lence”를 검색어로 사용하였다. 국외 현황 검토에 대한 문헌 의 포함기준은 1) 1990년 이후에 출판되었고, 2) 한글 또는 영 어로 작성되었으며, 3) 북미(미국, 캐나다), 유럽, 일본, 호주에 대한 현황에 대해 발표한 문헌들로 제한하였다. 각 검색원에 서 검색된 모든 문헌들의 제목과 초록을 바탕으로 1차적으 로 검토하여 중복된 논문과 연구 주제에 부합되지 않는 논 문을 배제한 후 최종적으로 선정된 문헌들을 고찰하였다. 최 종 선정된 문헌들을 미국/캐나다, 유럽, 일본/호주로 분류하 여 표 2의 형식에 맞게 정리하였다.
우리나라 및 미국, 유럽, 호주, 뉴질랜드를 포함한 국외 환 자안전 기관에서 사용되고 있는 의약품 사용오류에 대한 분 류유형 기준은 크게 심각도, 절차, 행위, 주체로 나뉘어진다.
심각도는 오류(error) 및 위해의 발생 여부 및 정도에 따라, 절
차는 의약품이 환자에게 도달하는 과정에 따라, 주체는 오류 를 일으키거나 적용되는 대상에 따라 구분되며, 행위의 경우 절차 기준과 일부 개념이 혼재되어 있다.
4)이러한 선행연구 결과를 바탕으로 의약품 사용오류의 분류유형을 정리한 후, 국내에서 사용하기에 적합한 유형을 알아보기 위해 환자 안 전 및 의약품 사용오류에 대한 임상 전문가 7명과 비임상 전 문가 3명에게 자문의견조사를 시행하였다. 자문의견조사는 2 주 동안 전자우편을 통해 이루어졌다.
결 과
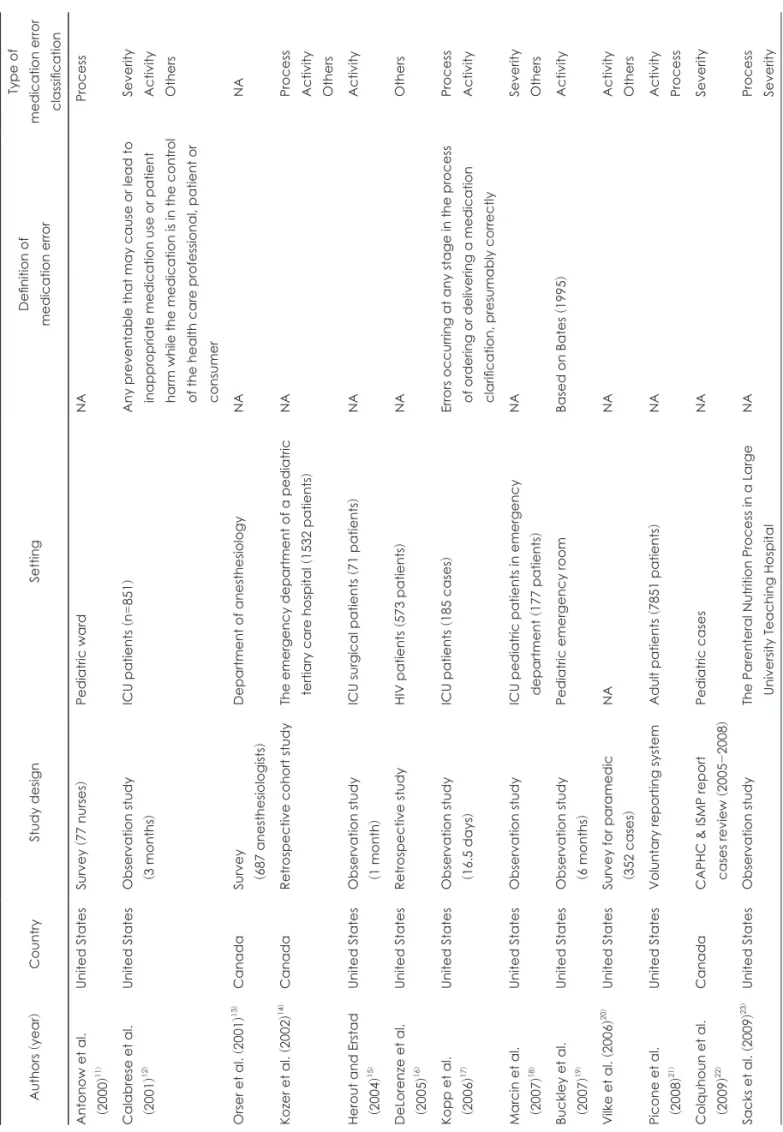
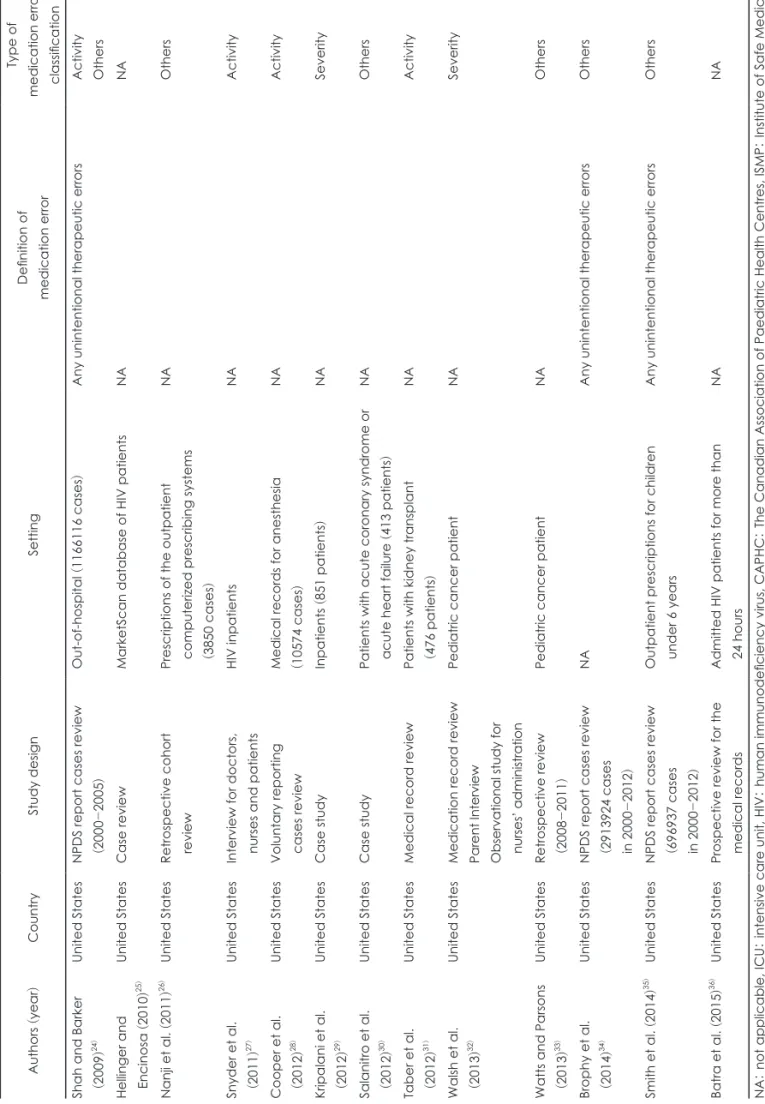
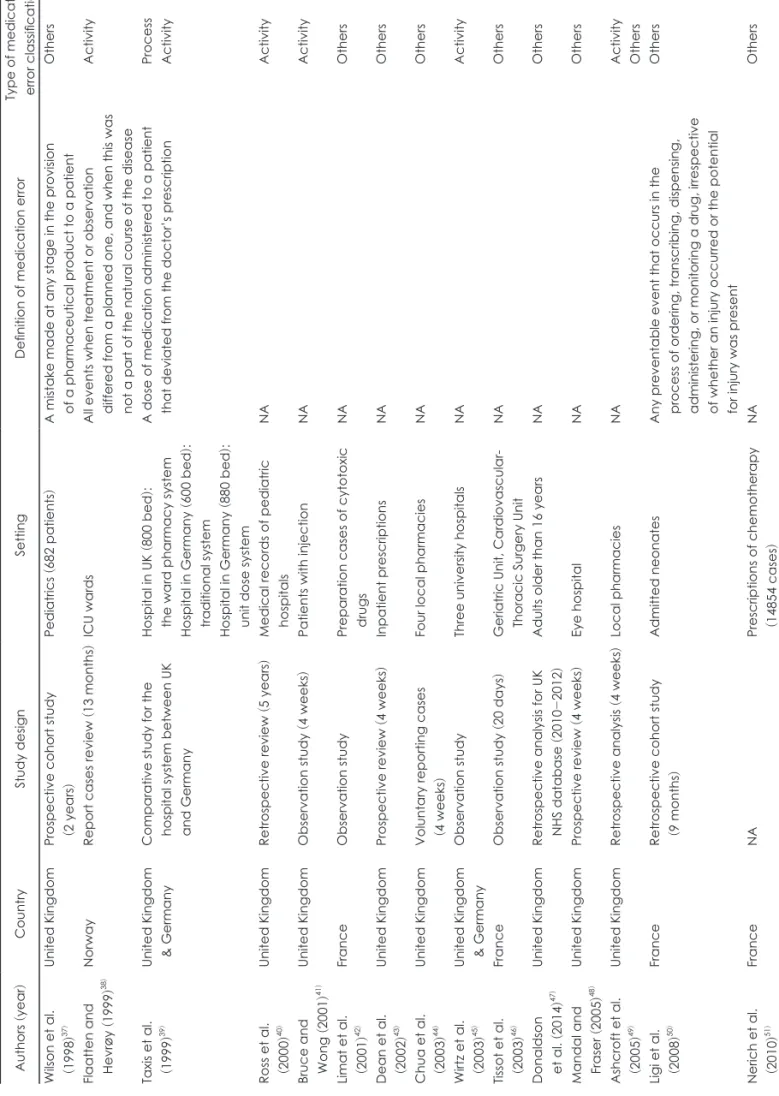
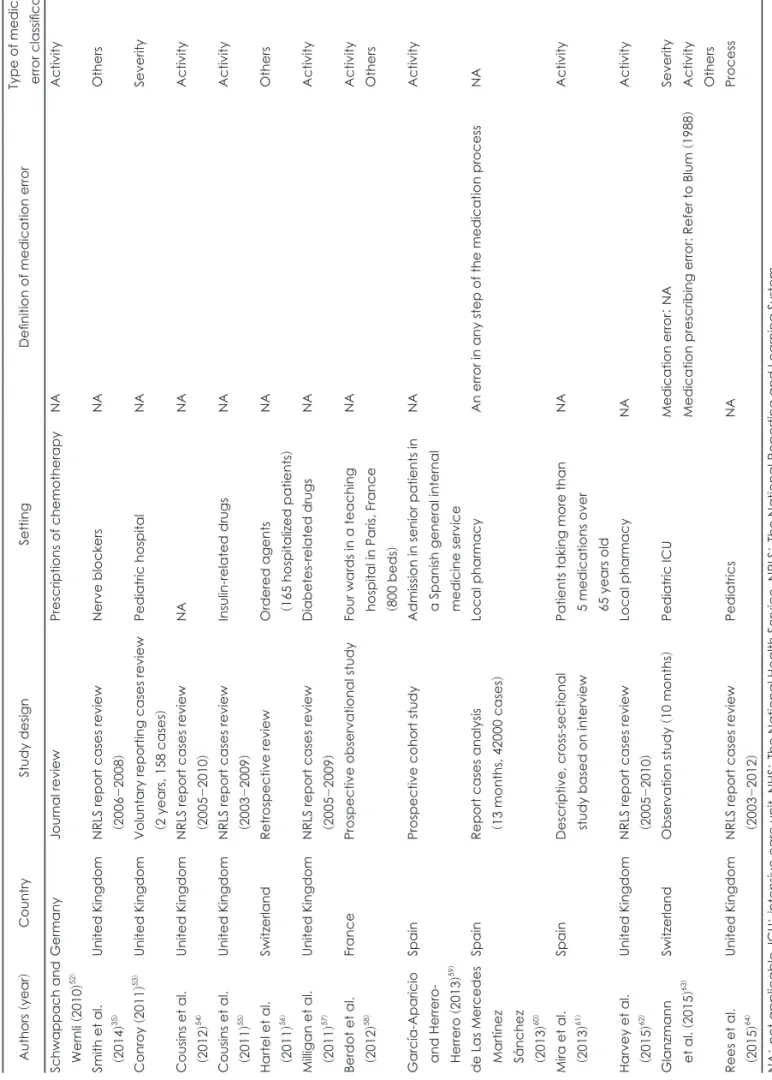
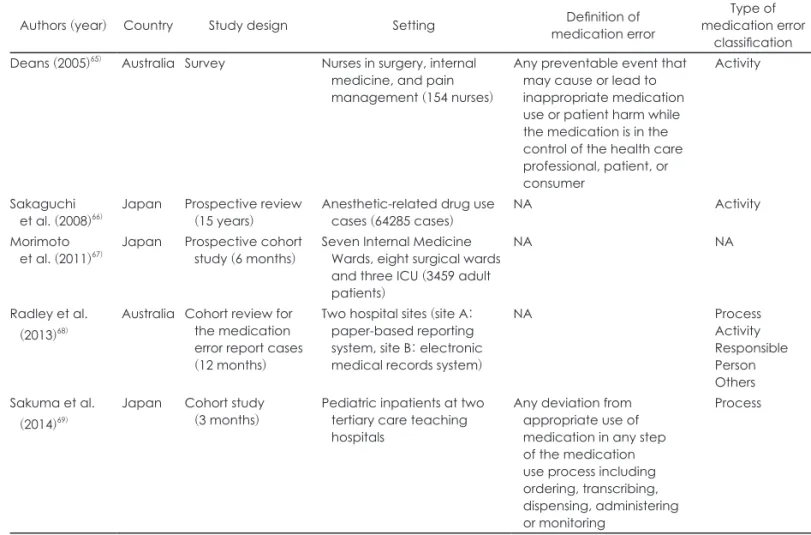
국외문헌에서의 의약품 사용오류 분류유형 이용현황을 검 토한 결과, 총 60건의 문헌이 포함되었다(표 3, 4, 5). 나라별 로는 미국 및 캐나다가 26건(표 3), 유럽은 29건(표 4), 일본 및 호주는 5건(표 5)으로 나타났다. 연구설계에서는 관찰연 구가 가장 많았으며, 다음으로 자발적 보고 또는 보고시스템 연구, 후향적 연구 순으로 나타났으며, 그 외 설문조사 등의 방법도 수행되었다. 검색된 문헌 전체 중 의약품 사용오류의 정의에 대해 서술한 논문은 일부(14건)였으며, 그 외 다수의
Table 1. Resources used in literature searchDatabase Link
National Digital Science Library http://www.ndsl.kr/index.do Medical Digital Library Information System http://www.medlis.kr/index.do National Assembly Library of Korea http://www.nanet.go.kr/main.jsp National Knowledge Information System https://www.nkis.re.kr:4445/main.do Policy Research Information Service & Management http://www.prism.go.kr/
Korea Education and Research Information Service http://www.riss.kr/
KoreaMed http://www.koreamed.org/SearchBasic.php
PubMed http://www.ncbi.nlm.nih.gov
Table 2. Categorization format-studies for the medication error
Category Description
Author Author’s first name, publish year
Country Countries where literature studies were conducted Study design Study design and year of study
Setting Target population
Definition of medication error The definition of medication error used in each study Type of medication error classification
Severity7) No Harm, Harm, Death, etc.
Activity8) Dose Omission, Improper Dose, Wrong Strength/Concentration, Wrong Drug, Wrong Dosage, Wrong Technique (includes inappropriate crushing of tablets), Wrong Route of Administration, Wrong Rate, Wrong Duration, Wrong Time, Wrong Patient, Monitoring Error (includes contraindicated drugs), Deteriorated Drug Error (Dispensing drug which has expired), etc.
Process6) Prescription, Transcription, Dispensing, Administration, Monitoring, etc.
Responsible Person9) Physicians, Pharmacists, Nurses, Patients, etc.
Others Type of medicinal efficacy, Type of system, etc.
Table 3. Definition and types of medication error in previous studies (United States & Canada) Authors (year
)CountryStudy designSettingDefinition of medication error
Type of medication error classification Antonow et al. (2000
)11)United StatesSurvey
(77 nurses
)Pediatric wardNAProcess Calabrese et al. (2001
)12)United StatesObservation study (3 months
)ICU patients
(n=)851Any preventable that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient or consumer
Severity Activity Others Orser et al.
(2001
)13) CanadaSurvey (687 anesthesiologists
)
Department of anesthesiologyNANA Kozer et al.
(2002
)14) CanadaRetrospective cohort studyThe emergency department of a pediatric tertiary care hospital
(1532 patients
)NAProcess Activity Others Herout and Erstad (2004
)15)United StatesObservation study (1 month
)ICU surgical patients
(71 patients
)NAActivity DeLorenze et al. (2005
)16)United StatesRetrospective studyHIV patients
(573 patients
)NAOthers Kopp et al. (2006
)17)United StatesObservation study (16.5 days
)ICU patients
(185 cases
)Errors occurring at any stage in the process of ordering or delivering a medication clarification, presumably correctly
Process Activity Marcin et al. (2007
)18)United StatesObservation studyICU pediatric patients in emergency department
(177 patients
)NASeverity Others Buckley et al. (2007
)19)United StatesObservation study (6 months
)Pediatric emergency roomBased on Bates
(1995
)Activity Vilke et al.
(2006
)20) United StatesSurvey for paramedic (352 cases
)NANAActivity Others Picone et al. (2008
)21)United StatesVoluntary reporting systemAdult patients
(7851 patients
)NAActivity Process Colquhoun et al. (2009
)22)CanadaCAPHC & ISMP report cases review
(2005
-2008)Pediatric casesNASeverity Sacks et al.
(2009
)23) United StatesObservation studyThe Parenteral Nutrition Process in a Large University Teaching HospitalNAProcess Severity
Table 3. Definition and types of medication error in previous studies (United States & Canada) (continued) Authors (year
)CountryStudy designSettingDefinition of medication error
Type of medication error classification Shah and Barker (2009
)24)United StatesNPDS report cases review (2000
-2005)Out-of-hospital
(1166116 cases
)Any unintentional therapeutic errorsActivity Others Hellinger and Encinosa
(2010
)25)United StatesCase reviewMarketScan database of HIV patientsNANA Nanji et al.
(2011
)26)United StatesRetrospective cohort reviewPrescriptions of the outpatient computerized prescribing systems (3850 cases
)
NAOthers Snyder et al. (2011
)27)United StatesInterview for doctors, nurses and patientsHIV inpatientsNAActivity Cooper et al. (2012
)28)United StatesVoluntary reporting cases reviewMedical records for anesthesia (10574 cases
)NAActivity Kripalani et al. (2012
)29)United StatesCase studyInpatients
(851 patients
)NASeverity Salanitro et al. (2012
)30)United StatesCase studyPatients with acute coronary syndrome or acute heart failure
(413 patients
)NAOthers Taber et al. (2012
)31)United StatesMedical record reviewPatients with kidney transplant (476 patients
)NAActivity Walsh et al. (2013
)32)United StatesMedication record review Parent Interview Observational study for nurses’ administration
Pediatric cancer patientNASeverity Watts and Parsons (2013
)33)United StatesRetrospective review (2008
-2011)Pediatric cancer patientNAOthers Brophy et al. (2014
)34)United StatesNPDS report cases review (2913924 cases in 2000-2012)
NAAny unintentional therapeutic errorsOthers Smith et al.
(2014
)35) United StatesNPDS report cases review (696937 cases in 2000-2012)
Outpatient prescriptions for children under 6 yearsAny unintentional therapeutic errorsOthers Batra et al.
(2015
)36) United StatesProspective review for the medical recordsAdmitted HIV patients for more than 24 hoursNANA NA: not applicable, ICU: intensive care unit, HIV: human immunodeficiency virus, CAPHC: The Canadian Association of Paediatric Health Centres, ISMP: Institute of Safe Medica- tion Practices, NPDS: National Poison Data System
Table 4. Definition and types of medication error in previous studies (Europe) Authors (year
)CountryStudy designSettingDefinition of medication errorType of medication error classification Wilson et al. (1998
)37)United KingdomProspective cohort study (2 years
)Pediatrics
(682 patients
)A mistake made at any stage in the provision of a pharmaceutical product to a patientOthers Flaatten and Hevrøy
(1999
)38)NorwayReport cases review
(13 months
)ICU wardsAll events when treatment or observation differed from a planned one, and when this was not a part of the natural course of the disease
Activity Taxis et al. (1999
)39)United Kingdom & GermanyComparative study for the hospital system between UK and Germany
Hospital in UK
(800 bed ):
the ward pharmacy system Hospital in Germany
(600 bed ):
traditional system Hospital in Germany
(880 bed ):
unit dose system
A dose of medication administered to a patient that deviated from the doctor’s prescriptionProcess Activity Ross et al. (2000
)40)United KingdomRetrospective review
(5 years
)Medical records of pediatric hospitalsNAActivity Bruce and Wong
(2001
)41)United KingdomObservation study
(4 weeks
)Patients with injectionNAActivity Limat et al. (2001
)42)FranceObservation studyPreparation cases of cytotoxic drugsNAOthers Dean et al. (2002
)43)United KingdomProspective review
(4 weeks
)Inpatient prescriptionsNAOthers Chua et al. (2003
)44)United KingdomVoluntary reporting cases (4 weeks
)Four local pharmaciesNAOthers Wirtz et al. (2003
)45)United Kingdom & GermanyObservation studyThree university hospitalsNAActivity Tissot et al. (2003
)46)FranceObservation study
(20 days
)Geriatric Unit, Cardiovascular- Thoracic Surgery UnitNAOthers Donaldson et al.
(2014
)47)United KingdomRetrospective analysis for UK NHS database
(2010
-2012)Adults older than 16 yearsNAOthers Mandal and Fraser
(2005
)48)United KingdomProspective review
(4 weeks
)Eye hospitalNAOthers Ashcroft et al. (2005
)49)United KingdomRetrospective analysis
(4 weeks
)Local pharmaciesNAActivity Others Ligi et al. (2008
)50)FranceRetrospective cohort study (9 months
)Admitted neonatesAny preventable event that occurs in the process of ordering, transcribing, dispensing, administering, or monitoring a drug, irrespective of whether an injury occurred or the potential for injury was present
Others Nerich et al. (2010
)51)FranceNAPrescriptions of chemotherapy (14854 cases
)NAOthers
Table 4. Definition and types of medication error in previous studies (Europe) (continued) Authors (year
)CountryStudy designSettingDefinition of medication errorType of medication error classification Schwappach and Wernli
(2010
)52)GermanyJournal reviewPrescriptions of chemotherapyNAActivity Smith et al. (2014
)35)United KingdomNRLS report cases review (2006
-2008)Nerve blockersNAOthers Conroy
(2011
)53) United KingdomVoluntary reporting cases review (2 years, 158 cases
)Pediatric hospitalNASeverity Cousins et al. (2012
)54)United KingdomNRLS report cases review (2005
-2010)NANAActivity Cousins et al. (2011
)55)United KingdomNRLS report cases review (2003
-2009)Insulin-related drugsNAActivity Hartel et al. (2011
)56)SwitzerlandRetrospective reviewOrdered agents (165 hospitalized patients
)NAOthers Milligan et al. (2011
)57)United KingdomNRLS report cases review (2005
-2009)Diabetes-related drugsNAActivity Berdot et al. (2012
)58)FranceProspective observational studyFour wards in a teaching hospital in Paris, France (800 beds
)
NAActivity Others García-Aparicio and Herrero- Herrero
(2013
)59)
SpainProspective cohort studyAdmission in senior patients in a Spanish general internal medicine service
NAActivity de Las Mercedes Martínez Sánchez (2013
)60)
SpainReport cases analysis (13 months, 42000 cases
)Local pharmacyAn error in any step of the medication processNA Mira et al. (2013
)61)SpainDescriptive, cross-sectional study based on interviewPatients taking more than 5 medications over 65 years old
NAActivity Harvey et al. (2015
)62)United KingdomNRLS report cases review (2005
-2010)Local pharmacyNAActivity Glanzmann et al.
(2015
)63)SwitzerlandObservation study
(10 months
)Pediatric ICUMedication error
: NA
Medication prescribing error: Refer to Blum
(1988
)Severity Activity Others Rees et al. (2015
)64)United KingdomNRLS report cases review (2003
-2012)PediatricsNAProcess NA: not applicable, ICU: intensive care unit, NHS: The National Health Service, NRLS: The National Reporting and Learning System
문헌들은 의약품 사용오류의 정의가 언급되지 않거나, 의약품 사용오류의 하부 개념[예: 근접오류(near-miss), 의약품 처 방오류(prescribing medication error)] 등에 대해서만 서술 하였다.
사용된 분류기준 유형은 행위(29건), 기타(25건), 심각도(9 건), 절차(7건), 주체(1건) 순으로 나타났으며, 하나의 연구에 두 가지 이상의 분류유형이 함께 사용된 연구들도 13건으로 나타났다. 이 중 행위 분류유형을 사용한 연구에서 가장 많
Table 5. Definition and types of medication error in previous studies (Australia & Japan)Authors (year) Country Study design Setting Definition of medication error
Type of medication error
classification Deans (2005)65) Australia Survey Nurses in surgery, internal
medicine, and pain management (154 nurses)
Any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer
Activity
Sakaguchi
et al. (2008)66) Japan Prospective review
(15 years) Anesthetic-related drug use
cases (64285 cases) NA Activity
Morimoto
et al. (2011)67) Japan Prospective cohort
study (6 months) Seven Internal Medicine Wards, eight surgical wards and three ICU (3459 adult patients)
NA NA
Radley et al.
(2013)68)
Australia Cohort review for the medication error report cases (12 months)
Two hospital sites (site A:
paper-based reporting system, site B: electronic medical records system)
NA Process
Activity Responsible Person Others Sakuma et al.
(2014)69)
Japan Cohort study
(3 months) Pediatric inpatients at two tertiary care teaching hospitals
Any deviation from appropriate use of medication in any step of the medication use process including ordering, transcribing, dispensing, administering or monitoring
Process
NA: not applicable, ICU: intensive care unit
Table 6. Experts’ opinion on the types of medication error
Questions Category Number of respondents
Which of the following methods are considered appropriate for classification of medication error in Korea? (possible for overlapping response)
Severity 7
Activity 7
Process 5
Responsible Person 4
None 0
Questions Category Very
appropriate Appropriate Neutral Inappropriate Very inappropriate Do you think the following
method is appropriate for classifying medication error in Korea?
Severity 3 4 3 0 0
Activity 4 4 2 0 0
Process 1 5 3 1 0
Responsible person 2 4 3 1 0
Questions Category Very high High Moderate Low Very low
Do you think the following categories are likely to be used in Korea?
Severity 4 3 2 1 0
Activity 4 5 1 0 0
Process 3 3 3 1 0
Responsible person 3 4 2 1 0
이 나타난 의약품 사용오류는 용량 오류였으며, 그 외 분류유 형에서는 연구설계 및 설정에 따라 상이한 결과를 나타냈다.
선행연구에 따라 현재 사용되고 있는 의약품 사용오류의 분류유형을 정리한 결과, 심각도 기준에서는 National Coor- dinating Council for Medication Error Reporting and Pre- vention(이하 NCC MERP)에서 정의한 유형이 국외 사례 및 문헌에서 가장 널리 사용되고 있었고,
6)절차 기준 중에서 는 의약품이 사용되는 다양한 환경과 주체를 함께 고려한 IOM 보고서의 의약품 사용 절차(medication-use process)가 있었으며,
7)행위 기준 중에서는 비교적 순수하게 행위에 초 점을 맞춘 NCC MERP 유형이,
8)주체 기준에서는 주요한 주체를 모두 포괄하면서도 최대한 간단한 기준을 보여주고 있는 Morimoto 등
9)의 연구 유형이 의약품 사용오류 분류유 형으로 사용되고 있었다. 이를 바탕으로 의약품 사용오류 분 류유형의 종류로 심각도, 행위, 절차, 주체를 제시하고 이들
유형을 국내에서 사용하는 것에 대한 적절성과 사용가능성 에 대하여 자문지를 작성하였다(Appendix). 작성된 설문지 를 총 10명의 전문가들에게 보냈고, 전원 자문에 응하였다.
먼저 어떤 의약품 사용오류 분류유형이 우리나라에서 사용 하기 적절한지를 묻는 질문(중복응답 허용)에서는 심각도 및 행위 분류기준이 가장 많았으며(7명), 다음으로 절차(5 명), 주체(4명) 분류기준 순서로 선택되었다. 다음으로 모든 분류유형들에 대해 Likert 5점 척도(매우 적절하다, 적절하 다, 보통이다, 부적절하다, 매우 부적절하다)를 사용하여 적 절성 및 우리나라에서의 사용가능성을 평가하도록 한 결과, 적절성에서는 행위 분류기준이 가장 높은 점수를 받았으며, 다음으로 심각도, 주체, 절차 분류기준 순서로 나타났고, 우 리나라에서의 사용가능성의 순서는 행위-심각도-주체-절 차 분류 순으로 높게 나타났다(표 6). 또한 적절성 및 사용가 능성에 대한 응답이유 및 자문의견을 서술하도록 하였으며,
Table 7. Experts’ opinion for the appropriateness and suitability of the types of medication errorType Description
심각도 ‘생명유지를 위한 중재가 필요한 경우’는 약물유해반응에서 serious ADR, 중대한 유해반응을 생명의 위협을 초래하거나, 유해반응으로 인한 입원, 입원이 연장되는 경우, 영구적인 장해로 표현하고 있어, ‘치명적인 또는 생명의 위협을 초래하는 경우’ 등으로 수정하면 좋을 것 같음
9단계 분류는 너무 전문적이고 복잡함
현재 대다수의 병원은 ASHP의 분류방식10)을 사용 중임
적신호사건, 위해사건, 근접오류에 대한 내용과 같이 검토되어져야 하고, 특히 근접오류의 경우 기관이나 평가자마다 기준이 달라 혼선이 있는 경우가 많음
사용오류의 경중이 오류의 분류에 영향을 미치기보다는 사용오류의 유무가 더 중요하게 여겨진다고 생각함 행위 ‘처방 오류’를 추가하는 것이 좋을 듯함
처방, 조제, 감사, 투약, 모니터링, 복약이행, 기타 등의 단계가 명확하지 않음 주체와 행위가 함께 분류되어 있으면 사용하기 편리할 것으로 생각됨
‘잘못된’이라는 용어보다 ‘오류’가 적절함(예: ‘잘못된 약물’보다 ‘약물 오류’가 적절한 표현)
‘중복 행위(예: 동일 약품을 중복으로 처방/조제/투여)’에 해당하는 항목이 없음 주체별 행위, 절차 등이 함께 분류되어 있으면 사용이 편리할 것으로 예상됨 절차 전사(transcribing)의 개념이 잘 와닿지 않음
‘투여’ 대신 ‘투약’이라는 표현이 적절함
대부분의 병원이 EMR 또는 OCS 전산시스템을 운영하고 있으므로 ‘transcribing(전사)’이라는 절차에 대한 재검토가 필요함 약품의 사용 단계에는 ‘선정’, ‘구매(공급)’도 있으므로 이 부분도 절차에 포함시킬 필요가 있음
‘transcribing’은 ‘prescribing’ 또는 ‘dispensing’에 포함시킬 수 있으므로 따로 절차로 생각하지 않는 것이 좋을 듯함
‘투여’ 단계는 의사나 간호사가 투여하는 경우와 환자가 복용하는 경우로 나누어야 할 것으로 보임 주체 ‘환자’보다는 ‘환자나 보호자’가 우리나라 현실에 더 적합함
‘기타’는 ‘기타(제약회사, 의약품 허가기관 등)’로 명시하는 것이 좋을 듯함
‘기타’에는 보조직원(pharmacy assistant)이 해당될 수 있음
만성질환자가 증가하면서 투약에 있어서 보호자 또는 간병인의 역할이 증가하고 있으므로 ‘보호자, 간병인’을 주체에 추가해야 함 절차와 겹치는 부분이 많아, 절차분류의 ‘투여’ 단계만 주체로 구분한다면 별도로 주체분류는 필요하지 않음
현실적으로 쉽게 체크 가능하여야 하는데 업무상 구분이 힘들 것으로 예상되며, 현재 대다수의 병원은 ASHP의 분류방식10)을 사용 중임 분류가 너무 세분화되어 있어서 대형병원, 상급종합병원, 대학병원 급에서는 사용할 수 있겠지만, 그 외의 소규모 기관에서의
사용가능성은 미지수임
이 기준을 적용하여 판단하려면 의사와의 논의가 필요하기 때문에 활용도가 떨어질 수 있음
ADR: adverse drug reaction, ASHP: American Society of Health-System Pharmacists, EMR: electronic medical record, OCS: order communication system
그 결과는 표 7과 같았다.
고 찰
선행연구 결과를 참고하여 의약품 사용오류의 유형을 크 게 심각도 기준, 절차 기준, 행위 기준, 주체 기준으로 나누어 전문가 자문을 수행하였을 때, 심각도 기준과 행위 기준이 적합성과 사용가능성이 높음을 알 수 있었다. 심각도 기준인 NCC MERP 방법은 9단계 분류로 이루어져 있어 다소 복잡 할 수 있으나, 국내외를 포괄하였을 때 가장 많이 사용되고 있 는 방법이고 오류의 발생여부와 위해의 발생여부 및 정도를 함께 판단할 수 있는 장점이 있다. 행위 기준에서는 단계의 모호성, 일부 오류 유형의 누락(예: 처방오류, 중복오류) 등의 한계가 발견되었으며, 주체 기준과 함께 사용해야 한다는 의 견이 있었다. 또한, 현재 많은 병원에서는 NCC MERP의 분류 방식보다 간단한 American Society of Health-System Phar - macists(ASHP)의 분류방식
10)을 사용하고 있음을 알 수 있었다.
국외 문헌의 검토를 통해, 비교적 행위 기준이 빈번히 사용 되고는 있었으나, 한 가지 기준만을 사용하여 의약품 사용오 류를 서술하기보다, 필요에 따라 다양한 분류기준을 사용하 여 연구를 수행하는 경향이 나타났다. 또한 여러 분류기준들 이 복합되어 있으면서 어느 하나의 기준으로 결정하기 모호 한 분류기준이 사용된 경우는 기타로 분류하였는데, 이 기준 에 해당되는 분류유형이 행위 기준 다음으로 많이 나타났다.
따라서 의약품 사용오류를 분류할 경우, 전문가 자문 결과 적합성과 사용가능성이 높았으며 문헌고찰 결과 사용빈도 가 높았던 행위 기준을 우선 고려하고, NCC MERP의 행위 기준으로 서술하기에 모호한 경우 필요한 구성요소를 간명한 정의와 함께 추가할 수도 있을 것이다. 또한 행위의 주체를 구분할 수 있는 주체 기준이나 사용오류의 단계별 발생 현황 을 파악할 수 있는 절차 기준을 함께 사용하여 의약품 사용 오류 분류의 명확성과 유용성을 높일 수 있다. 다만, 주체나 절차 기준을 함께 적용할 경우, 여러 연구들 간의 비교, 종합 이 용이할 수 있도록 가능한 한 상세한 서술이 동반되어야 할 것이다. 다음으로 의약품 사용오류의 심각도에 대한 평가가 필요할 경우, 본 연구에서 제시한 NCC MERP의 심각도 기준 을 활용할 수 있고, 이를 통해 심각도뿐만 아니라 오류 및 위 해의 유무를 함께 판단할 수 있다.
본 연구의 한계는 다음과 같다. 첫째, 전문가 자문 수행 시 논 의된 4가지 분류 기준들에 대한 다양한 방법들이 모두 논의 되지는 못하였다. 그러나 가장 널리 사용되고 있거나, 논의를 통해 여러 방식을 포괄할 수 있는 방법들을 각 기준별로 선정 하여 자문지를 작성하였고, 전문가들의 다양한 의견들을 적
극적으로 수렴하여 자문지에 반영되지 못한 방법들에 대해 서도 함께 논의하였다. 둘째, 문헌 검토 시 고려된 연구들에 서는 국내 문헌들이 제외되었다. 추가 연구를 통해 국내의 의약품 사용오류 현황에 대한 연구들을 고려하여 국내 상황 에 대한 면밀한 검토가 이루어져야 한다.
결 론
향후 의약품 사용오류의 국내 현황에 대한 연구 진행 시, 체 계적인 연구를 위해서는 의약품 사용오류에 대한 정의를 명 확히 서술할 필요가 있으며, 의약품 사용오류 분류 기준으로 심각도와 행위 기준을 사용할 수 있고, 연구 설계 및 대상, 의 약품 사용오류의 정의 등에 따라 주체 및 절차 기준도 함께 고려될 수 있다.
Acknowledgments
본 연구는 2015년도 식품의약품안전처의 연구개발비(15172의약안 118)로 수행되었으며 이에 감사드립니다.
REFERENCES
1) Institute of Medicine; Committee on Quality of Health Care in Amer- ica; Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academies Press;
2000.
2) Koo BK. Patient safety management in the medication use process:
prevention and management of medication error. J Korean Med As- soc 2012;55:835-842.
3) Ministry of Food and Drug Safety. Development of education mate- rials to ensure medication safety and prevent medication error. Cheon- gju: Ministry of Food and Drug Safety;2015.
4) Kim S, Han S, Suh HS. The analysis of definition and types for medi- cation error used in foreign countries. J Health Tech Assess 2016;4:
35-43.
5) Ministry of Health and Welfare. Guidelines for preventing medica- tion error. Gwacheon: Ministry of Health and Welfare;2008.
6) National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). NCC MERP index for categorizing medi- cation errors [cited 2015 Aug 21]. Available from: http://www.ncc- merp.org/sites/default/files/indexColor2001-06-12.pdf.
7) Committee on Identifying and Preventing Medication Errors, Aspden P, Wolcott J, Bootman JL, Cronenwett LR. Preventing medication errors: quality chasm series. Washington, DC: The National Acade- mies Press;2007. p.463.
8) National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). Recommendations to enhance accuracy of administration of medications [cited 2015 Aug 21]. Available from: http://www.nccmerp.org/recommendations-enhance-accuracy- administration-medications.
9) Morimoto T, Gandhi TK, Seger AC, Hsieh TC, Bates DW. Adverse drug events and medication errors: detection and classification meth- ods. Qual Saf Health Care 2004;13:306-314.
10) ASHP guidelines on preventing medication errors in hospitals. Am J Hosp Pharm 1993;50:305-314.
11) Antonow JA, Smith AB, Silver MP. Medication error reporting: a sur- vey of nursing staff. J Nurs Care Qual 2000;15:42-48.
12) Calabrese AD, Erstad BL, Brandl K, Barletta JF, Kane SL, Sherman
DS. Medication administration errors in adult patients in the ICU. In- tensive Care Med 2001;27:1592-1598.
13) Orser BA, Chen RJ, Yee DA. Medication errors in anesthetic practice:
a survey of 687 practitioners. Can J Anaesth 2001;48:139-146.
14) Kozer E, Scolnik D, Macpherson A, Keays T, Shi K, Luk T, et al. Vari- ables associated with medication errors in pediatric emergency medi- cine. Pediatrics 2002;110:737-742.
15) Herout PM, Erstad BL. Medication errors involving continuously in- fused medications in a surgical intensive care unit. Crit Care Med 2004;
32:428-432.
16) DeLorenze GN, Follansbee SF, Nguyen DP, Klein DB, Horberg M, Quesenberry CP Jr, et al. Medication error in the care of HIV/AIDS patients: electronic surveillance, confirmation, and adverse events.
Med Care 2005;43(9 Suppl):III63-III68.
17) Kopp BJ, Erstad BL, Allen ME, Theodorou AA, Priestley G. Medica- tion errors and adverse drug events in an intensive care unit: direct ob- servation approach for detection. Crit Care Med 2006;34:415-425.
18) Marcin JP, Dharmar M, Cho M, Seifert LL, Cook JL, Cole SL, et al.
Medication errors among acutely ill and injured children treated in ru- ral emergency departments. Ann Emerg Med 2007;50:361-367.e1-e2.
19) Buckley MS, Erstad BL, Kopp BJ, Theodorou AA, Priestley G. Direct observation approach for detecting medication errors and adverse drug events in a pediatric intensive care unit. Pediatr Crit Care Med 2007;8:145-152.
20) Vilke GM, Tornabene SV, Stepanski B, Shipp HE, Ray LU, Metz MA, et al. Paramedic self-reported medication errors. Prehosp Emerg Care 2006;10:457-462.
21) Picone DM, Titler MG, Dochterman J, Shever L, Kim T, Abramowitz P, et al. Predictors of medication errors among elderly hospitalized patients. Am J Med Qual 2008;23:115-127.
22) Colquhoun M, Orrbine E, Sheppard I, Stromquist L, Koczmara C, Cheng R, et al. National collaborative: top five drugs reported as caus- ing harm through medication error in pediatrics. Dynamics 2009;20:
20-22.
23) Sacks GS, Rough S, Kudsk KA. Frequency and severity of harm of medication errors related to the parenteral nutrition process in a large university teaching hospital. Pharmacotherapy 2009;29:966-974.
24) Shah K, Barker KA. Out-of-hospital medication errors: a 6-year anal- ysis of the national poison data system. Pharmacoepidemiol Drug Saf 2009;18:1080-1085.
25) Hellinger FJ, Encinosa WE. The cost and incidence of prescribing er- rors among privately insured HIV patients. Pharmacoeconomics 2010;
28:23-34.
26) Nanji KC, Rothschild JM, Salzberg C, Keohane CA, Zigmont K, Devita J, et al. Errors associated with outpatient computerized pre- scribing systems. J Am Med Inform Assoc 2011;18:767-773.
27) Snyder AM, Klinker K, Orrick JJ, Janelle J, Winterstein AG. An in- depth analysis of medication errors in hospitalized patients with HIV.
Ann Pharmacother 2011;45:459-468.
28) Cooper L, DiGiovanni N, Schultz L, Taylor AM, Nossaman B. Influ- ences observed on incidence and reporting of medication errors in anesthesia. Can J Anaesth 2012;59:562-570.
29) Kripalani S, Roumie CL, Dalal AK, Cawthon C, Businger A, Eden SK, et al. Effect of a pharmacist intervention on clinically important medi- cation errors after hospital discharge: a randomized trial. Ann Intern Med 2012;157:1-10.
30) Salanitro AH, Osborn CY, Schnipper JL, Roumie CL, Labonville S, Johnson DC, et al. Effect of patient- and medication-related factors on inpatient medication reconciliation errors. J Gen Intern Med 2012;27:
924-932.
31) Taber DJ, Pilch NA, Bratton CF, McGillicuddy JW, Chavin KD, Baliga PK. Medication errors and adverse drug events in kidney transplant recipients: incidence, risk factors, and clinical outcomes. Pharmaco- therapy 2012;32:1053-1060.
32) Walsh KE, Roblin DW, Weingart SN, Houlahan KE, Degar B, Billett
A, et al. Medication errors in the home: a multisite study of children with cancer. Pediatrics 2013;131:e1405-e1414.
33) Watts RG, Parsons K. Chemotherapy medication errors in a pediatric cancer treatment center: prospective characterization of error types and frequency and development of a quality improvement initiative to lower the error rate. Pediatr Blood Cancer 2013;60:1320-1324.
34) Brophy TJ, Spiller HA, Casavant MJ, Chounthirath T, Smith MD, Xiang H. Medication errors reported to U.S. Poison Control Centers, 2000-2012. Clin Toxicol (Phila) 2014;52:880-888.
35) Smith MD, Spiller HA, Casavant MJ, Chounthirath T, Brophy TJ, Xiang H. Out-of-hospital medication errors among young children in the United States, 2002-2012. Pediatrics 2014;134:867-876.
36) Batra R, Wolbach-Lowes J, Swindells S, Scarsi KK, Podany AT, Say- les H, et al. Impact of an electronic medical record on the incidence of antiretroviral prescription errors and HIV pharmacist reconcilia- tion on error correction among hospitalized HIV-infected patients.
Antivir Ther 2015;20:555-559.
37) Wilson DG, McArtney RG, Newcombe RG, McArtney RJ, Gracie J, Kirk CR, et al. Medication errors in paediatric practice: insights from a continuous quality improvement approach. Eur J Pediatr 1998;157:
769-774.
38) Flaatten H, Hevrøy O. Errors in the intensive care unit (ICU). Experi- ences with an anonymous registration. Acta Anaesthesiol Scand 1999;
43:614-617.
39) Taxis K, Dean B, Barber N. Hospital drug distribution systems in the UK and Germany--a study of medication errors. Pharm World Sci 1999;21:25-31.
40) Ross LM, Wallace J, Paton JY. Medication errors in a paediatric teach- ing hospital in the UK: five years operational experience. Arch Dis Child 2000;83:492-497.
41) Bruce J, Wong I. Parenteral drug administration errors by nursing staff on an acute medical admissions ward during day duty. Drug Saf 2001;
24:855-862.
42) Limat S, Drouhin JP, Demesmay K, Tissot E, Jacquet M, Woronoff- Lemsi MC. Incidence and risk factors of preparation errors in a cen- tralized cytotoxic preparation unit. Pharm World Sci 2001;23:102-106.
43) Dean B, Schachter M, Vincent C, Barber N. Prescribing errors in hos- pital inpatients: their incidence and clinical significance. Qual Saf Health Care 2002;11:340-344.
44) Chua SS, Wong IC, Edmondson H, Allen C, Chow J, Peacham J, et al.
A feasibility study for recording of dispensing errors and near misses’
in four UK primary care pharmacies. Drug Saf 2003;26:803-813.
45) Wirtz V, Taxis K, Barber ND. An observational study of intravenous medication errors in the United Kingdom and in Germany. Pharm World Sci 2003;25:104-111.
46) Tissot E, Cornette C, Limat S, Mourand JL, Becker M, Etievent JP, et al. Observational study of potential risk factors of medication ad- ministration errors. Pharm World Sci 2003;25:264-268.
47) Donaldson LJ, Panesar SS, Darzi A. Patient-safety-related hospital deaths in England: thematic analysis of incidents reported to a nation- al database, 2010-2012. PLoS Med 2014;11:e1001667.
48) Mandal K, Fraser SG. The incidence of prescribing errors in an eye hospital. BMC Ophthalmol 2005;5:4.
49) Ashcroft DM, Quinlan P, Blenkinsopp A. Prospective study of the in- cidence, nature and causes of dispensing errors in community pharma- cies. Pharmacoepidemiol Drug Saf 2005;14:327-332.
50) Ligi I, Arnaud F, Jouve E, Tardieu S, Sambuc R, Simeoni U. Iatrogenic events in admitted neonates: a prospective cohort study. Lancet 2008;
371:404-410.
51) Nerich V, Limat S, Demarchi M, Borg C, Rohrlich PS, Deconinck E, et al. Computerized physician order entry of injectable antineoplastic drugs: an epidemiologic study of prescribing medication errors. Int J Med Inform 2010;79:699-706.
52) Schwappach DL, Wernli M. Medication errors in chemotherapy: inci- dence, types and involvement of patients in prevention. A review of
the literature. Eur J Cancer Care (Engl) 2010;19:285-292.
53) Conroy S. Association between licence status and medication errors.
Arch Dis Child 2011;96:305-306.
54) Cousins DH, Gerrett D, Warner B. A review of medication incidents reported to the National Reporting and Learning System in England and Wales over 6 years (2005-2010). Br J Clin Pharmacol 2012;74:597- 55) Cousins D, Rosario C, Scarpello J. Insulin, hospitals and harm: a re-604.
view of patient safety incidents reported to the National Patient Safety Agency. Clin Med (Lond) 2011;11:28-30.
56) Hartel MJ, Staub LP, Röder C, Eggli S. High incidence of medication documentation errors in a Swiss university hospital due to the hand- written prescription process. BMC Health Serv Res 2011;11:199.
57) Milligan FJ, Krentz AJ, Sinclair AJ. Diabetes medication patient safe- ty incident reports to the National Reporting and Learning Service: the care home setting. Diabet Med 2011;28:1537-1540.
58) Berdot S, Sabatier B, Gillaizeau F, Caruba T, Prognon P, Durieux P.
Evaluation of drug administration errors in a teaching hospital. BMC Health Serv Res 2012;12:60.
59) García-Aparicio J, Herrero-Herrero JI. Medication errors detected in elderly patients admitted to an internal medicine service. Int J Clin Pract 2013;67:282-289.
60) de Las Mercedes Martínez Sánchez A. Medication errors in a Spanish community pharmacy: nature, frequency and potential causes. Int J Clin Pharm 2013;35:185-189.
61) Mira JJ, Orozco-Beltrán D, Pérez-Jover V, Martínez-Jimeno L, Gil- Guillén VF, Carratala-Munuera C, et al. Physician patient communi-
cation failure facilitates medication errors in older polymedicated pa- tients with multiple comorbidities. Fam Pract 2013;30:56-63.
62) Harvey J, Avery AJ, Ashcroft D, Boyd M, Phipps DL, Barber N. Ex- ploring safety systems for dispensing in community pharmacies: fo- cusing on how staff relate to organizational components. Res Social Adm Pharm 2015;11:216-227.
63) Glanzmann C, Frey B, Meier CR, Vonbach P. Analysis of medication prescribing errors in critically ill children. Eur J Pediatr 2015;174:1347- 1355.
64) Rees P, Edwards A, Powell C, Evans HP, Carter B, Hibbert P, et al. Pe- diatric immunization-related safety incidents in primary care: a mixed methods analysis of a national database. Vaccine 2015;33:3873-3880.
65) Deans C. Medication errors and professional practice of registered nurses. Collegian 2005;12:29-33.
66) Sakaguchi Y, Tokuda K, Yamaguchi K, Irita K. Incidence of anesthe- sia-related medication errors over a 15-year period in a university hos- pital. Fukuoka Igaku Zasshi 2008;99:58-66.
67) Morimoto T, Sakuma M, Matsui K, Kuramoto N, Toshiro J, Murakami J, et al. Incidence of adverse drug events and medication errors in Ja- pan: the JADE study. J Gen Intern Med 2011;26:148-153.
68) Radley DC, Wasserman MR, Olsho LE, Shoemaker SJ, Spranca MD, Bradshaw B. Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. J Am Med In- form Assoc 2013;20:470-476.
69) Sakuma M, Ida H, Nakamura T, Ohta Y, Yamamoto K, Seki S, et al.
Adverse drug events and medication errors in Japanese paediatric in- patients: a retrospective cohort study. BMJ Qual Saf 2014;23:830-837.
Expert questionnaire for the types of medication error
B-4. 의약품 사용오류의 분류
본 연구에서는 의약품 사용오류에 대한 정의와 판단 기준뿐만 아니라, 분류 방법도 함께 제안하고자 합니다. 문헌 고찰 등 을 통하여 자료를 수집 및 선정한 결과, 다양한 분류 기준들(심각도, 행위, 절차, 주체 등)이 존재하였습니다. 본 연구진은 이 들 중 하나 이상을 우리나라 의약품 사용오류의 분류 방법으로 제안하고자 합니다.
분류기분 참고로 한 지침 또는 문헌 참조 페이지
심각도 NCC MERP Index for Categorizing Medication Errors
a)13 행 위 NCC MERP Taxonomy of Medication Errors-TYPE
b)14 절 차 Institute of Medicine (IOM) Medication-use process
c)15
주 체 Morimoto 등
d)의 연구 15
원문과 국문은 참조 페이지에 제시되어 있습니다. 각각의 분류 방법을 보시고 아래 질문에 따라 의견을 주시기 바랍니다.
B-4-a. 다음 중 우리나라 의약품 사용오류 분류에 사용하기 적절하다고 생각되는 분류 방법은 무엇입니까? (중복 응답 가능) 1) 심각도: NCC MERP Index for Categorizing Medication Errors
2) 행위: NCC MERP Taxonomy of Medication Errors-TYPE
3) 절차: IOM Medication-use process
4) 주체: Morimoto 등의 연구
5) 없다 (이유: )
(다른 분류 방법 추천: )
a)
National Coordinating Council for Medication Error Reporting and Prevention. “Index” [cited 2015 Jul 8]. Available at:
http://www.nccmerp.org/sites/default/files/indexColor2001-06-12.pdf.
b)
National Coordinating Council for Medication Error Reporting and Prevention. “Taxonomy” [cited 2015 Jul 8]. Available at: http://www.nccmerp.org/sites/default/files/taxonomy2001-07-31.pdf.
c)
Aspden P, Wolcott J, Bootman JL, Cronenwett LR. Preventing medication errors. Washing, DC: National Academies Press;2007.
d)
Morimoto T, Gandhi TK, Seger AC, Hsieh TC, Bates DW. Adverse drug events and medication errors: detection and
classification methods. Qual Saf Health Care 2004;13:306-314.
오. 만일 ③~⑤라고 생각하신다면 그 이유에 대해서도 기술해 주십시오.
의약품 사용오류 분류 방법
① 매우
적절하다 ② 적절하다 ③ 보통이다 ④ 부적절하다 ⑤ 매우
부적절하다
심각도
<③~⑤로 응답한 경우에 대한 이유>
행 위
<③~⑤로 응답한 경우에 대한 이유>
절 차
<③~⑤로 응답한 경우에 대한 이유>
주 체
<③~⑤로 응답한 경우에 대한 이유>
⑤라고 생각하신다면 그 이유에 대해서도 기술해 주십시오.
의약품 사용오류
분류 방법 ① 매우 높다 ② 높다 ③ 보통이다 ④ 낮다 ⑤ 매우 낮다
심각도
<③~⑤로 응답한 경우에 대한 이유>
행 위
<③~⑤로 응답한 경우에 대한 이유>
절 차
<③~⑤로 응답한 경우에 대한 이유>
주 체
<③~⑤로 응답한 경우에 대한 이유>
● 국문
오류 없음
오류 있음, 위해 없음
오류 있음, 위해 있음
오류 있음, 사망
정의 위해
신체적, 감정적, 정신적 기능 또는 신체 구조의 손상, 그리고/또는 그로 인한 통증 모니터링
관련된 생리적 또는 정신적 징후를 관찰 또는 기록하는 것 중재
치료의 변경 또는 적극적인 의학적/수술적 치료를 포함할 수 있음 생명 유지를 위한 중재 심혈관과 호흡 유지 장치를 포함
(예를 들어 심폐소생술, 제세동, 삽관법 등)
Category A:
오류를 일으킬 잠재력이 있는 환경이나 사건
Category B:
오류가 발생하였으나 환자에게 도달하지 않은 경우(‘투여 누락 오류’는 환자에게 도달함)
Category C:
오류가 발생하여 환자에게 도달하였으나 환자에게
위해를 일으키지 않은 경우 Category D:
오류가 발생하여 환자에게 도달하였고 이로
인해 다음 행위 중 하나 이상이 필요한 경우:
① 환자에게 위해를 일으키지 않는다는 것을 확인하기 위한 모니터링,
② 위해를 방지하기 위한 중재 Category E:
오류가 발생하여 환자에게 일시적인 위해를 일으켰거나 일으키는 데 기여했을
가능성이 있고, 이로 인해 중재를 필요로 하는 경우 Category F:
오류가 발생하여 환자에게 일시적인 위해를 일으켰거나 일으키는 데 기여했을
가능성이 있고, 이로 인해 입원 또는
입원 기간의 연장을 필요로
하는 경우 Category G:
오류가 발생하여 환자에게 영구적인 위해를 일으켰거나 일으키는 데
기여했을 가능성이 있는 경우
Category H:
오류가 발생하여 생명 유지를 위한 중재를 필요로
하는 경우
Category I:
오류가 발생하여 환자의 사망을 초래했거나 초래하는 데 기여했을
가능성이 있는 경우
● 원문
No Error Error, No Harm Error, Harm Error, Death
© 2001 National Coordinating Council for Medication Error Reporting and Prevention. All Rights Reserved.
*Permission is hereby granted to reproduce information contained herein provided that such reproduction shall not modify the text and shall include the copyright notice appearing on the pages from which it was copied.
Definitions Harm
Impairment of the physical, emotional, or psychological function or structure of the body and/or pain resulting therefrom.
Monitoring To observe or record relevant physiological or psychological signs.
Intervention May include change in therapy or active medical/
surgical treatment.
Intervention Necessary to Sustain Life
Includes cardiovascular and respiratory support (e.g., CPR, defibrillation, intubation, etc.) NCC MERP Index for Categorizing Medication Errors
Category A:
Circumstances or events that have the capacity
to cause error Category B:
An error occurred but the error did not reach the patient (An “error of omission” does reach the
patient)
Category C:
An error occurred that reached the patient but did not cause patient
harm
Category D:
An error occurred that reached the patient and
required monitoring to confirm that it resulted in
no harm to the patient and/or required
intervention to preclude harm Category E:
An error occurred that may have contributed to
or resulted in temporary harm to the patient and required intervention Category F:
An error occurred that may have
contributed to or resulted in temporary harm to
the patient and required initial or prolonged hospitalization Category G:
An error occurred that may have contributed to or resulted in permanent
patient harm Category H:
An error occurred that required intervention necessary to sustain life
Category I:
An error occurred that may have contributed to or resulted in the
patient’s death