INTRODUCTION
The frontal recess is an anatomically complex area with many variations. A thorough knowledge of the recess is essential for safe and successful endoscopic surgical man- agement of frontal sinus disease.1) This narrow space could be pneumatized by various frontoethmoidal cells (FECs), including the agger nasi cells (ANCs), frontal cells (FCs) type 1 to 4, suprabullar cells (SBCs), frontal bullar cells (FBCs), supraorbital ethmoid cells (SOECs) and interfron- tal sinus septal cells (ISSCs).2) 3) To differentiate FECs and understand the anatomy of the frontal recess, simultane- ous analysis with the axial/coronal computed tomographic
(CT) images and sagittal reconstruction is essential.4) 5) The reported incidences of FECs vary widely in the literature.6-12) The variation could be explained by dif- ferences in enrolled patients and/or interrater differences when examining CT scans.12) Moreover, the CT scans used in previous studies had different cutting thicknesses or resolutions. The primary purpose of this study is to deter- mine the prevalence of various FECs in patients with and without the frontal sinus/recess mucosal thickening sepa- rately through a detailed study of triplanar CT images.
Various FECs can narrow the frontal recess causing a partial obstruction of drainage and aeration of the frontal sinus.12) To date, only few reports regarding the associa- tion between FECs and frontal sinus/recess disease exist, which is still unclear. Although there was a significant association of frontal sinus mucosal thickening with the presence of type 1, 2 and 3 FCs12) or type 3 and 4 FCs,14) 15) other authors were not able to find such association.6) 13) In another report, rather than the FECs anterior to the frontal recess (ANCs and FCs), the FECs posterior and postero- - 31 -
Frontoethmoidal Cells on Computed Tomographic Analysis:
The Prevalence and Relationship to Frontal Sinus/Recess Mucosal Thickening
Seung Ju Lee, MD1, Hyun Woo Kang, MD1, Kwang Kyu Yu1, MD and Hyun-Sook Kim, MD2
1Department of Otorhinolaryngology-Head and Neck Surgery;
2Department of Radiology, Eulji Hospital, Eulji Hospital, Eulji University College of Medicine, Seoul, South Korea
ABSTRACT
Objectives : To determine the prevalence of frontoethmoidal cells (FECs) in patients with and without frontal sinus/recess mucosal thickening and to establish the relationship between the FECs and the frontal sinus/recess mucosal thickening. Materials and Methods : We retrospectively reviewed 245 consecutive ostiomeatal CT scans (490 sides). The normal and frontal sinus/recess mucosal thickening groups were categorized based on these images. The latter group was sub-categorized into the frontal sinus mucosal thickening group (FS group) and the frontal recess mucosal thickening group (FR group). Results : Types 1, 2, 3 and 4 frontal cells were found in 17.5, 6.7, 8.3 and 0%of 326 normal sides, respectively. The prevalence of agger nasi, suprabullar, frontal bul- lar, supraorbital ethmoid and interfrontal sinus septal cells was 85.6, 43.3, 4.9, 4.3 and 17.2% of the same 326 normal sides, respectively. Type 3 frontal cells, frontal bullar cells and suprabullar cells were more prevalent in the FS and FR groups than in the normal group. All types of cells were more prevalent in the FS group, but only the suprabullar cells were more prevalent in the FR group than in the normal group. Conclusion : These findings suggest that type 3 frontal cells, frontal bullar cells and suprabullar cells may have a significant association with frontal sinus/recess mucosal thickening.
KEY WORDS : Frontoethmoidal Cells·Frontal Sinusitis·Computed Tomography.
Address correspondence and reprint requests to Seung Ju Lee, MD, Department of Otorhinolaryngology-Head and Neck Surgery, Eulji Hospital, Eulji University College of Medicine, 280-1 Hagye-dong, Nowon-gu, Seoul 139-711, South Korea.
Tel : +82-2-970-8276 · Fax : +82-2-970-8275 E-mail : [email protected]
Received for publication on October 30, 2013 Accepted for publicatoin on December 21, 2013
lateral to the frontal recess (SBCs, FBCs and SOECs) were associated with the development of frontal sinusitis.6) The secondary purpose of this study is to clarify the specific correlation of FECs to frontal sinus/recess mucosal thick- ening by comparing the frequency of these cells between groups of patients with and without frontal sinus/recess mucosal thickening.
MATERIALS AND METHODS
We retrospectively reviewed 269 consecutive os- tiomeatal triplanar CT scans of Korean adult patients per- formed from March 2012 to February 2013. Each patient’s information such as age, sex and the purpose of the scan has been collected. These patients underwent CT scan- ning for the assessment of nasal symptoms such as nasal obstruction, rhinorrhea, posterior nasal dripping, anosmia, facial pain, headache, etc. Out of 269 patients, 24 patients were discarded: 4 was younger than 18 years, 12 had pre- vious surgical changes, 8 had poor frontal sinus develop- ment, leaving 245 patients.
CT scans of the nasal cavities and paranasal sinuses were performed with contiguous axial cuts of 2mm thick- ness (120 kVp, 210mAs, FOV 180 ×180 mm) on GE Discovery 750HD CT scanners (GE Medical Systems, Milwaukee, WI, USA). The CT data were then recon- structed into coronal and sagittal images by GE worksta- tion Adw 4.5 software (GE, USA). Each CT scan was studied jointly by one ENT surgeon (Lee SJ) and one radiologist (Kim HS). We evaluated coronal, sagittal and axial images for the presence of FCs type 1 to 4, ANCs, SBCs, FBCs, SOECs and ISSCs by the definitions and criteria for FECs by Lee et al.2) Triplanar scrolling at a computer workstation facilitated identification of FECs.
Appropriate magnification and window setting improved bony detail, which was particularly useful in significant- ly diseased sinuses.
All CT images were evaluated for the presence of fron- tal sinus/recess mucosal thickening greater than 3 mm as in previous studies.6) 12-14) One hundred forty-two CT scans (284 sides) were normal or nearly-normal without any sinus disease, regardless of the purpose of the scans.
Forty two CT scans showed unilateral frontal sinus/recess lesions. Consequently, no radiographic evidence of frontal sinus/recess mucosal thickening was found in 326 sides.
Sixty one CT scans (122 sides) showed bilateral fron- tal sinus/recess lesions. From all CT images, two major groups were categorized; the normal group and the frontal sinus/recess mucosal thickening group (164 sides). Then, the later group was sub-categorized into two groups; the frontal sinus mucosal thickening group (FS group) and the frontal recess mucosal thickening group (FR group). The FS group had mucosal thickening involving the frontal sinus with or without the frontal recess (110 sides), and the FR group had mucosal thickening involving only the frontal recess (54 sides).
The prevalence of each type of FECs was presented as total numbers and percentages. Using Fisher’s exact test, we compared the frontal sinus/recess mucosal thickening group, FS group and FR group with the normal group, re- spectively. Univariate and multivariate logistic regression analyses between the normal group and the frontal sinus/
recess mucosal thickening group were also performed.
Then, odds ratio and 95% confidence interval were calcu- lated for each FEC. Data were evaluated statistically using the SPSS program for Windows version 12.0 (SPSS Inc, Chicago, IL, USA). P values < 0.05 were considered sta- tistically significant. The study protocol for a retrospective
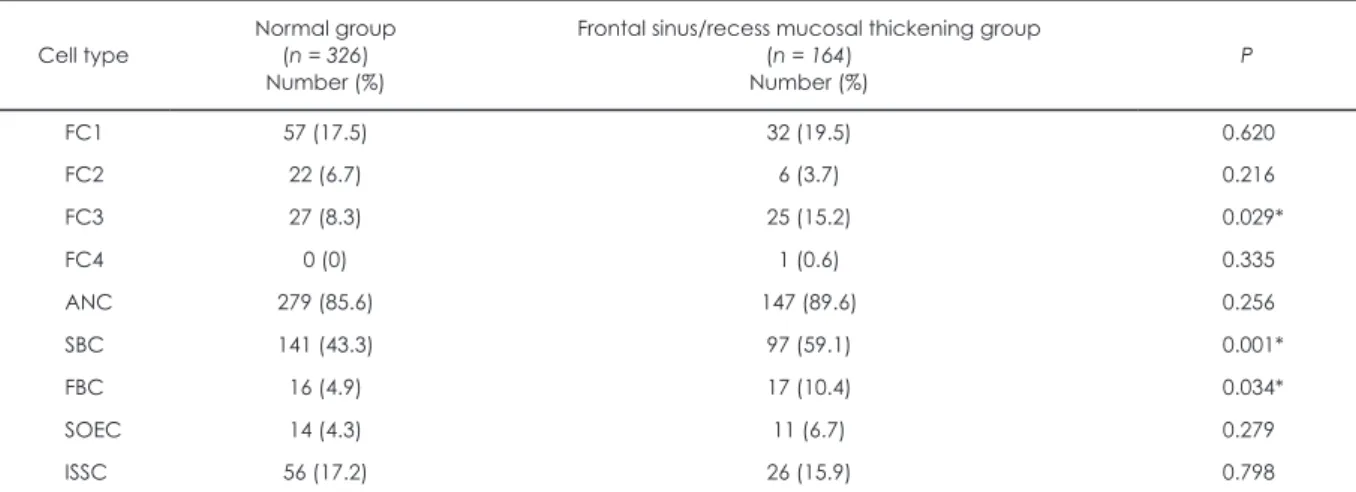
Table 1. The prevalence of frontoethmoidal cells and their relationship to frontal sinus/recess mucosal thickening.
Cell type
Normal group (n = 326) Number (%)
Frontal sinus/recess mucosal thickening group (n = 164)
Number (%) P
FC1 57 (17.5) 32 (19.5) 0.620
FC2 22 (6.7) 6 (3.7) 0.216
FC3 27 (8.3) 25 (15.2) 0.029*
FC4 0 (0) 1 (0.6) 0.335
ANC 279 (85.6) 147 (89.6) 0.256
SBC 141 (43.3) 97 (59.1) 0.001*
FBC 16 (4.9) 17 (10.4) 0.034*
SOEC 14 (4.3) 11 (6.7) 0.279
ISSC 56 (17.2) 26 (15.9) 0.798
* Statistically significant.
FC: frontal cell, ANC: agger nasi cell, SBC: suprabullar cell, FBC: frontal bullar cell, SOEC: supraorbital ethmoid cell, ISSC: interfrontal sinus septal cell.
chart and CT review for research purposes was approved by the Institutional Review Board.
RESULTS
A total of 490 sides from 245 patients were assessed and used for the final data analysis. There were 150 male (61.2%) and 95 female patients (38.8%). The mean age was 42.8 years (range, 18 to 85 years) . Table 1 shows the prevalence of FECs in sides with and without frontal sinus/recess mucosal thickening. Of the 326 normal sides (66.5%), type 1, 2, 3 and 4 FCs were found in 17.5% (57 sides), 6.7% (22 sides), 8.3% (27 sides) and 0%, respec- tively. The prevalence of ANCs, SBCs, FBCs, SOECs and ISSCs was 85.6% (279 sides), 43.3% (141 sides), 4.9%
(16 sides), 4.3% (14 sides) and 17.2% (56 sides), respec- tively.
Of the 164 sides with frontal sinus/recess mucosal thick- ening (33.5%), type 1, 2, 3, and 4 FCs were found in 19.5%
(32 sides), 3.7% (6 sides), 15.2% (25 sides) and 0.6%
(1 side), respectively. The prevalence of ANCs, SBCs, FBCs, SOECs and ISSCs was 89.6% (147 sides), 59.1%
(97 sides), 10.4% (17 sides), 6.7% (11 sides) and15.9%
(26 sides), respectively. Type 3 FCs, SBCs and FBCs were more prevalent in the frontal sinus/recess mucosal thick- ening group than in the normal group (p = 0.029, 0.001 and 0.034, respectively). From univariate and multivariate analysis, relatively higher presence of frontal sinus/recess mucosal thickening was observed in type 3 FCs, SBCs and FBCs (Table 2).
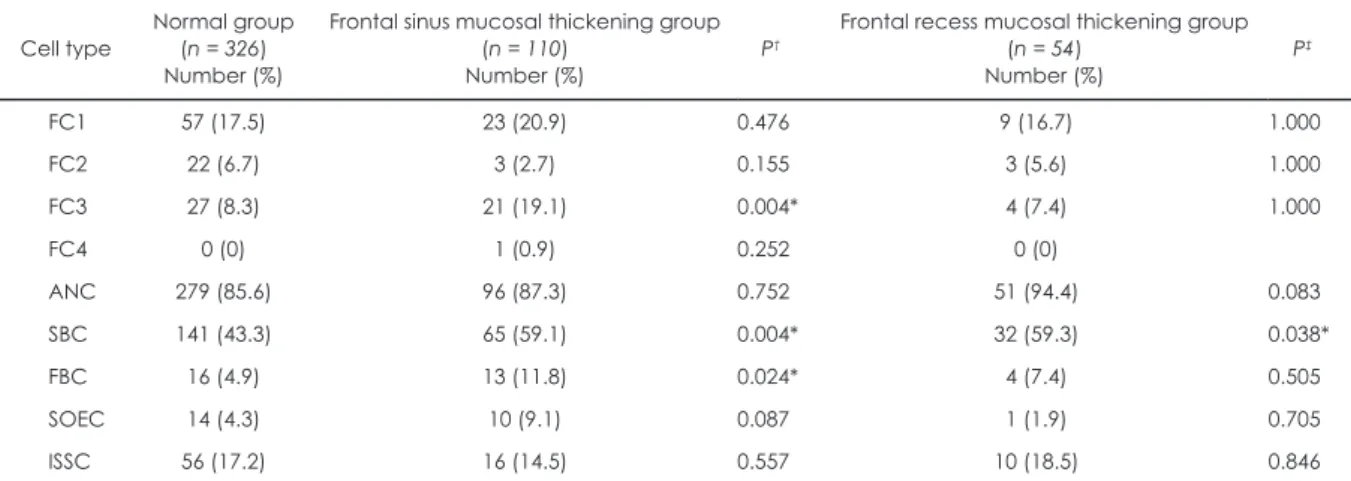
Table 3. The prevalence of frontoethmoidal cells in normal group, frontal sinus mucosal thickening group and frontal frontal recess mucosal thickening group.
Cell type
Normal group (n = 326) Number (%)
Frontal sinus mucosal thickening group (n = 110)
Number (%) P†
Frontal recess mucosal thickening group (n = 54)
Number (%) P‡
FC1 57 (17.5) 23 (20.9) 0.476 9 (16.7) 1.000
FC2 22 (6.7) 3 (2.7) 0.155 3 (5.6) 1.000
FC3 27 (8.3) 21 (19.1) 0.004* 4 (7.4) 1.000
FC4 0 (0) 1 (0.9) 0.252 0 (0)
ANC 279 (85.6) 96 (87.3) 0.752 51 (94.4) 0.083
SBC 141 (43.3) 65 (59.1) 0.004* 32 (59.3) 0.038*
FBC 16 (4.9) 13 (11.8) 0.024* 4 (7.4) 0.505
SOEC 14 (4.3) 10 (9.1) 0.087 1 (1.9) 0.705
ISSC 56 (17.2) 16 (14.5) 0.557 10 (18.5) 0.846
* Statistically significant.
† Fisher’s exact test was performed between normal group and frontal sinus group.
‡ Fisher’s exact test was performed between normal group and frontal recess group.
FC: frontal cell, ANC: agger nasi cell, SBC: suprabullar cell, FBC: frontal bullar cell, SOEC: supraorbital ethmoid cell, ISSC: interfrontal sinus septal cell.
Table 2. Results of logistic regression analysis for normal group and frontal sinus/recess mucosal thickening group.
Cell type Univariate analysis Multivariate analysis
OR 95% CI P OR 95% CI P
FC1 1.14 0.71-1.85 0.583 1.25 0.74-2.10 0.411
FC2 0.53 0.21-1.32 0.171 0.72 0.27-1.89 0.504
FC3 1.99 1.12-3.56 0.020* 2.33 1.25-4.37 0.008*
ANC 1.46 0.81-2.63 0.211 1.22 0.64-2.30 0.546
SBC 1.90 1.30-2.78 0.001* 2.52 1.65-3.85 0.000*
FBC 2.24 1.10-4.56 0.026* 3.89 1.80-8.40 0.001*
SOEC 1.73 0.76-3.95 0.193 2.09 0.89-4.95 0.093
ISSC 0.91 0.55-1.51 0.711 0.96 0.57-1.64 0.892
* Statistically significant.
OR: odds ratio, CI: confidence interval, FC: frontal cell, ANC: agger nasi cell, SBC: suprabullar cell, FBC: frontal bullar cell, SOEC:
supraorbital ethmoid cell, ISSC: interfrontal sinus septal cell.
Table 3 shows the prevalence of FECs of patients in FS group and FR group. In the FS group, type 3 FCs, SBCs and FBCs were more prevalent than in the normal group (19.1%, 59.1% and 11.8%, respectively) (p = 0.004, 0.004 and 0.024, respectively). In the FR group, only the preva- lence of SBCs was increased compared to the normal group (59.3%, p = 0.038).
DISCUSSION
The reported prevalence of FECs varies widely in the literature. The variation could be explained firstly by in- clusion of patients with frontal sinus/recess inflammation.
The presence of mucosal thickening or polyps within the frontal recess makes it more difficult to distinguish FECs from nearby structures on a CT scan. A number of pre- vious studies have not specifically divided the enrolled patients into those with and without frontal sinus/recess mucosal thickening. In this study, we have determined the prevalence of various FECs in normal group first. Then, the prevalence in the patients with frontal sinus/recess mucosal thickening was determined and compared. Re- cent studies of FECs in frontal recess by CT have focused on Asian adult population, therefore the ethnic difference must be considered.6-8) 16) Finally, a small number of en- rolled patients in the earlier studies may be a factor.2) 8-10)
In the previous studies, the prevalence of type 1 (20~20.4%), 2 (7~14%) and 3 (7~8.2%) FCs in normal Asian patients,6-8) increased a little to 28~37%, 17~20.7%
and 8~11% in normal Western patients.2) 8-10) The preva- lence in our study was more consistent with that in the Asian patients, predictably. Similar to most studies, we identified type 1 cells as the most common.2) 6-13) 17) How- ever, the second most common type of FCs was type 2,2)
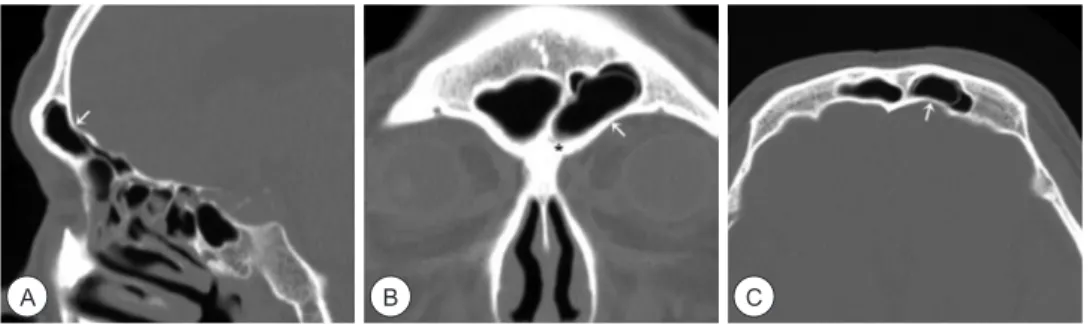
6) 8) 12) 17) or type 3.7) 9-11) 13) We found that type 3 FCs were more frequently found than type 2 FCs in normal group, and the prevalence of type 3 FCs increased markedly in those with frontal sinus/recess mucosal thickening. Type 4 FCs seemed to be quite rare and we found only one side in FS group with a type 4 FC and mucosal thickening involv- ing the dependent portion of the frontal sinus (Fig. 1). This episodic occurrence of type 4 FCs may make it difficult to decide any correlation of type 4 FCs to frontal sinus/
recess mucosal thickening. The prevalence of the ANCs in the earlier studies was 86~94.1%, without much dif- ference between the ethnic groups or between the groups with or without frontal sinus/recess mucosal thickening.
Our results are consistent with the above studies.
Anatomically, ANCs and FCs which are found above ANCs occur anteriorly in the frontal recess,2) and together they may narrow the frontal recess. Thus Langille et al re- ported that type 1, 2 and 3 FCs had association with fron-
Fig. 1. A type 4 frontal cell (white arrow) is seen in the left frontal sinus on the sagittal (A), coronal (B) and axial (C) CT images with the mucosal thickening involving the dependent portion of the sinus (asterisk).
A B C
Fig. 2. On left sagittal and axial CT images, the type 3 frontal cell (white arrow) attaches to the anterior wall of the frontal sinus whereas the frontal bullar cell (dashed arrow) to the posterior wall (A, C). This frontal bullar cell is seen above the type 3 frontal cell on the left side of coronal CT image (B). The frontal sinus shows total haziness (asterisk). On the right side of coronal CT image, a type 3 frontal cell (white arrow) above the agger nasi cell (black arrow) is also seen.
A B C
tal sinus mucosal thickening, but their conclusion lacked detailed data.12) In an analysis of 768 coronal CT scans which probably are not optimal for visualizing and char- acterizing all FECs, Meyer et al found a higher incidence of frontal mucosal thickening in patients with FCs type 3 and 4.14) But, DelGaudio et al and Lien et al reported that FCs and ANCs were not associated with frontal si- nusitis.6) 13) Despite above controversies, our data show clear and statistically significant association between type 3 FCs and the development of frontal sinusitis by the high prevalence of type 3 FCs in frontal sinus/recess mucosal thickening group and especially in FS group. We think that type 3 FCs are more likely to narrow the frontal recess because they do extend into frontal sinus (Fig. 2). For the ANCs and type 1 or 2 FCs, the size or spatial relationship with other FECs clearly weighs heavier than the presence per se in the occurrence of frontal sinus/recess mucosal thickening.
FBCs, SBCs and SOECs occur posteriorly in the frontal recess along the skull base.2) Contrary to the ANCs and FCs, the effect of these cells on frontal sinusitis has been dealt with in few reports.3) 12) Both the FBCs and SBCs might obstruct the frontal recess posteriorly.2) 6) SBCs have been more frequent in the normal Asian patients with the prevalence of 36~39.5%,6) 8) than in the normal West- ern patients with the prevalence of 11~20%.2) 8) 10) In our study, the prevalence of SBCs and FBCs in normal group, which was consistent with the previous studies increased significantly in the frontal sinus/recess mucosal thicken- ing group and in the subdivided FS group. We think that this increase in the current study may support the recent conclusions by Lien et al which suggested that both the FBCs and SBCs might have significant association with the development of frontal sinusitis.6)
Uniquely and for the first time, we assumed that the patients with minimal mucosal thickening involving only the frontal recess may have different characteristics in the prevalence of FECs compared with those with more extensive frontal sinus mucosal thickening. Interestingly,
in the FR group, the prevalence of FECs did not differ significantly compared with the normal group. Only the prevalence of SBCs noticeably increased to that in the FS group, suggesting that SBCs might have a role in the de- velopment of frontal recess mucosal thickening (Fig. 3).
SOECs which extend over the orbit from the frontal re- cess open into the lateral aspect of the frontal recess.6-12) On coronal CT images, SOECs are found lateral to the frontal sinus, whereas the FBCs are medial to it.16) SOECs were overwhelmingly more frequent in the Caucasian group (64.6%) than in the Korean group (2.6%).8) The presence of SOECs was reported to reveal significant association with the development of frontal sinusitis.6) Zhang et al re- ported 11 cases of chronic rhinosinusitis with 12 SOECs, which hints at a possible effect of SOEC on chronic rhi- nosinusitis.16) In our study, the prevalence of SOECs was consistent with the Asian studies,6-8) but did not differ be- tween those with and without frontal sinus/recess mucosal thickening, unpredictably.
The limitation of our study is that 2 mm cut CT images may not reveal all the cells, especially small type 1 or 2 FCs. However, small cells that are indistinguishable by the 2 mm cut CT slices may not have any effect on the frontal sinus/recess mucosal thickening. We believe that the suffi- cient number of patients have been enrolled for this study.
Also, the proportion of sides with frontal sinus/recess mu- cosal thickening was adequate (33.5%), compared to the previous study (14%).6) However, the number of sides in FR group was relatively small to confirm more confined results. Lastly, the etiologic factors of frontal sinusitis are anatomic variations, mucosal inflammation, polypo- sis, etc. Thus, it is not possible at this stage to designate the cause-and-effect relationship between the presence of FECs and frontal sinus/recess mucosal thickening.
Despite these limitations, our data are statistically sig- nificant with considerable consistency to indicate an as- sociation between the presence of type 3 FCs, FBCs and SBCs and frontal sinus/recess mucosal thickening. We believe that directly extending cells to the frontal sinus
Fig. 3. On sagittal and axial CT images, mucosal thickening of left frontal recess (asterisk) is seen between the type 3 frontal cell (white arrow) and the suprabullar cell (dashed arrow) (A, C). On coronal CT image, a type 3 frontal cell on the left (white arrow) and an interfrontal sinus septal cell (black arrow) on the right are seen (B).
A B C
and SBCs, along with the above etiologic factors will in- fluence the development of frontal sinus/recess mucosal thickening. For this reason, during endoscopic sinus sur- gery for frontal sinus, complete removal of these obstruct- ing cells is required in order to perform successful frontal sinus surgery.
CONCLUSIONS
In this study, the prevalence of FECs in patients without frontal sinus/recess mucosal thickening was consistent with that of the previous Asian studies. Type 3 FCs and FBCs that directly extend anteriorly and posteriorly to frontal sinus from the frontal recess and SBCs were more prevalent in the frontal sinus/recess mucosal thicken- ing group than in the normal group. They all were more prevalent in the FS group, but only the SBCs were more prevalent in the FR group than in the normal group. These findings suggest that type 3 FCs, FBCs and SBCs may have significant association with frontal sinus/recess mu- cosal thickening.
저자역할(Author Contributions)
이승주, 강현우, 유광규, 김현숙은 본 연구에서 모든 자료에 접근 할 수 있었으며 자료의 완전성과 자료 분석의 정확성에 책임을 지 고 있습니다. 연구 기획 : 이승주. 자료 수집 : 강현우, 유광규. 자 료의 해석 및 분석 : 이승주, 김현숙. 논문 초안 : 이승주, 강현우.
논문 수정 : 이승주, 유광규. 통계 분석 : 이승주, 강현우, 유광규.
연구 총괄 : 이승주.
REFERENCES
1) Huang BY, Lloyd KM, DelGaudio JM, Jablonowski E, Hudgins PA. Failed endoscopic sinus surgery: spectrum of CT findings in the frontal recess. Radiographics 2009;29:177-195.
2) Lee WT, Kuhn FA, Citardi MJ. 3D computed tomographic analy- sis of frontal recess anatomy in patients without frontal sinusitis.
Otolaryngol Head Neck Surg 2004;131:164-173.
3) Coates MH, Whyte AM, Earwaker JW. Frontal recess air cells:
spectrum of CT appearances. Australasian Radiol 2003;47:4-10.
4) Kanowitz SJ, Shatzkes DR, Pramanik BK, Babb JS, Jacobs JB,
Lebowitz RA. Utility of sagittal reformatted computerized tomo- graphic images in the evaluation of the frontal sinus outflow tract.
Am J Rhinol 2005;19:159-165.
5) Becker SS. Preoperative computed tomography evaluation in si- nus surgery: a template-driven approach. Otolaryngol Clin North Am 2010;43:731-751.
6) Lien CF, Weng HH, Chang YC, Lin YC, Wang WH. Computed to- mographic analysis of frontal recess anatomy and its effect on the development of frontal sinusitis. Laryngoscope 2010;120:2521- 2527.
7) Han D, Zhang L, Ge W, Tao J, Xian J, Zhou B. Multiplanar com- puted tomographic analysis of the frontal recess region in Chinese subjects without frontal sinus disease symptoms. ORL J Otorhi- nolaryngol Relat Spec 2008;70:104-112.
8) Cho JH, Citardi MJ, Lee WT, Sautter NB, Lee HM, Yoon JH, et al. Comparison of frontal pneumatization patterns between Kore- ans and Caucasians. Otolaryngol Head Neck Surg 2006;135:780- 9) Thomas L, Pallanch JF. Three-dimensional CT reconstruction and 786.
virtual endoscopic study of the ostial orientations of the frontal recess. Am J Rhinol Allergy 2010;24:378-384.
10) Dearking AC, Pallanch JF. Mapping the frontal sinus ostia using virtual endoscopy. Laryngoscope 2012;122:2143-2147.
11) Tuncyurek O, Songu M, Adibelli ZH, Onal K. Frontal in- fundibular cells: pathway to the frontal sinus. Ear Nose Throat J 2012;91:E29-32.
12) Langille M, Walters E, Dziegielewski PT, Kotylak T, Wright ED. Frontal sinus cells: identification, prevalence, and associa- tion with frontal sinus mucosal thickening. Am J Rhinol Allergy 2012;26:e107-110.
13) DelGaudio JM, Hudgins PA, Venkatraman G, Beningfield A. Mul- tiplanar computed tomographic analysis of frontal recess cells: ef- fect on frontal isthmus size and frontal sinusitis. Arch Otolaryngol Head Neck Surg 2005;131:230-235.
14) Meyer TK, Kocak M, Smith MM, Smith TL. Coronal computed tomography analysis of frontal cells. Am J Rhinol 2003;17:163- 15) Yildirim A. Is it more reasonable to categorize frontal cells on the 168.
basis of their location rather than on their type? Ear Nose Throat J 2010;89:E19-21.
16) Zhang L, Han D, Ge W, Tao J, Wang X, Li Y, Zhou B. Computed tomographic and endoscopic analysis of supraorbital ethmoid cells. Otolaryngol Head Neck Surg 2007;137:562-568.
17) Park SS, Yoon BN, Cho KS, Roh HJ. Pneumatization pattern of the frontal recess: Relationship of the anterior-to-posterior length of frontal isthmus and/or frontal recess with the volume of agger nasi cell. Clin Exp Otorhinolaryngol 2010;3:76-83.