-
20
-전두와의 해부학적 변이와 전두동염:
부비동 전산화단층촬영을 이용한 분석
영남대학교 의과대학 이비인후-두경부외과학교실
우현재·예상백·배창훈·송시연·김용대
Anatomic Variations of the Frontal Recess and Frontal Sinusitis:
Computed Tomographic Analysis
Hyun-Jae Woo, MD, Sang Baik Ye, MD, Chang Hoon Bae, MD, Si-Youn Song, MD and Yong-Dae Kim, MD
Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Yeungnam University, Daegu, Korea
ABSTRACT
Background and Objectives:The frontal recess (FR) cells, including the frontal cell (FC), agger nasi cell (ANC), supra- orbital ethmoid cell (SOC) and inter-frontal sinus septal cell (IFSSC), can interfere with the drainage system of the frontal sinus.
We evaluated the relationship between the FR cells and the frontal sinusitis. Subjects and Methods:All paranasal sinus CT scans performed from July 2004 through June 2005 were reviewed. Of the 675 scans reviewed, 317 patients (634 sides) were selected for data collection. Exclusion criteria included a clinical history of neoplasms, bony deformities, and extensive disease responsible for obscuring the bony anatomy. Similarly, CT scans with severe artifacts were also excluded. Result:FCs were present in 21.9% of the patients. According to the Bent’s classification, the prevalence of each FC type was as follows;
type 1 FC (13.6%), type 2 FC (3.2%), type 3 FC (1.9%) and type 4 FC (3.1%). Of the four types of FR cells, type 4 had a significant association with frontal sinusitis. The incidence of hyperpneumatized frontal sinus, ANC, SOC, IFSSC were sig- nificantly higher among patients with the FC than those without the FC (p<0.05). Patients without the ANC or with type 1 uncinate process, according to Stammberger’s classification, displayed a higher frequency of frontal sinusitis (p<0.05). There was a statistically significant decrease in the frequency of frontal sinusitis among patients with hypopneumatized frontal sinus (p<0.05). Conclusion:In our series, the frontal sinusitis was influenced by each types of FC, attachment sites of uncinate pro- cess and the degree of frontal sinus pneumatization. Therefore, these anatomic variations in the frontal recess should be ap- propriately addressed during the surgical management of the frontal sinusitis.
KEY WORDS:Frontal recess cells·Frontal sinusitis·Computed tomography.
서 론
내시경의 발달로 인해 대부분의 만성 비·부비동염 환자 의 치료에 내시경을 이용한 부비동 수술이 시행되고 있다.
하지만 전두와(frontal recess)의 형태적 특성과 주변의 구 조물들로 인해 내시경을 이용하여 전두동의 병소로 접근하 는 것은 많은 제약이 있으며 두개기저부와 안와지판이 인접 해 있어 조작이 힘들고 위험하다.1) 또한 전두와의 형태가 모
래시계의 모양과 유사하여 점막 손상시 반흔 형성으로 인해 전두와의 폐쇄가 쉽게 일어나 재발의 원인이 된다. 특히, 전 두봉소(frontal cell)와 전두동간 중격봉소(interfrontal sinus septal cell)의 유무나 구상돌기(uncinate process)의 부착위 치, 비제봉소(agger nasi cell)나 상안와 사골봉소(supraor- bital cell) 등의 해부학적인 구조물들에 의해 전두와로의 접 근이 어려울 뿐만 아니라 이들에 의해 전두와 유출로가 좁 아지기도 한다.2) 그러나 이러한 해부학적 구조물들이 전두 동 유출로의 폐쇄를 일으킬 수 있는 요소이기는 하지만 전 두동염과의 연관성을 규명하기위해 한국인을 대상으로 한 연구는 많지 않을 뿐만 아니라, 전두봉소와 비제봉소의 전 두동염과의 관련성에 대해서는 서로 상반된 결과를 나타내 논문접수일:2008년 7월 9일 / 심사완료일:2008년 9월 4일
교신저자:김용대, 705-717 대구광역시 남구 대명5동 317-1 영남대학교 의과대학 이비인후-두경부외과학교실
전화:(053) 620-3781·전송:(053) 628-7884 E-mail:[email protected]
고 있는 실정이다.2-4)
이에 저자들은 2 mm 간격으로 촬영한 부비동 전산화단 층촬영의 분석을 통해 전두와 주위의 해부학적 변이들의 빈 도를 알아보고, 이들 상호간의 관계 및 전두동염과의 연관성 에 대해 알아보고자 하였다.
대상 및 방법
2004년 7월부터 2005년 6월 사이에 코막힘, 비루 등의 비염이나 부비동염에 관련된 증상이 있어 진단 혹은 수술목 적으로 부비동 전산화단층촬영을 시행한 환자 675명을 대상 으로 Marotech사의 m-view Picture Archiving and Com- mucation System(PACS, version 4.0, Marotech Co., Seoul, Korea)을 이용하여 조사하였다. 전체 675명 중 종양, 안면 골 기형 및 성장부전, 광범위한 병변으로 인해 해부학적 구 조의 확인이 불가능한 경우, 촬영 중 움직임이나 보철물에 인한 인공음영이 심한 경우 및 부비동 수술이나 외상의 기 왕력이 있는 경우를 제외한 317명의 634측의 전산화단층촬
영을 분석하여 전두봉소의 유무 및 형태, 전두동 유출로 주 위에 위치하는 해부학적 구조물인 상안와 사골봉소, 비제봉 소, 전두동간 중격봉소의 유무와 구상돌기의 부착형태 및 전두동의 함기화 정도를 조사하였다. 전산화단층촬영에서 전 두동의 점막비후나 혼탁이 25%가 넘는 경우를 전두동염이 있는 것으로 간주하였다.2)
전산화단층촬영은 Siemens사의 SOMATOM plus 4(Sie- mens, Erlangen, Germany)를 이용하였으며 관상면과 축 상면 영상을 각각 2 mm 간격으로 촬영하였고 이를 이용하 여 시상면을 재구성하여 분석에 이용하였다.
전두와 봉소의 분류는 Lee 등5)이 정리하여 발표한 기준에 의해 분류하였고(Table 1), 구상돌기의 부착형태는 Stamm- berger의 분류6)를 기준으로 하였다. 전두동의 함기화 정도 는 함기화가 전두골의 안와판(orbital plate)와 편평부(squa- mous portion)까지 연장된 경우를 과함기화, 전후 방향으로 6 mm 미만이며 전두골 편평부로의 함기화가 없는 경우를 저함기화로 구분하였다.7)
또한 전두와 주위에 있는 각각의 해부학적 변이의 빈도를
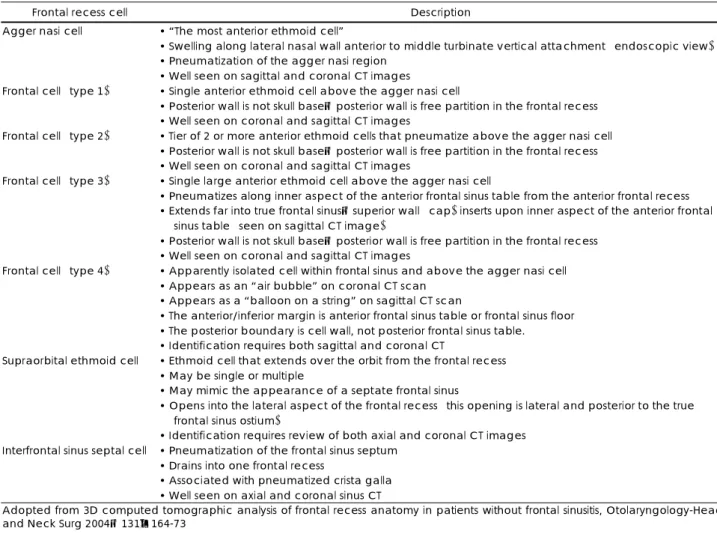
Table 1. Frontal pneumatization pattern definitions and criteria
Frontal recess cell Description
Agger nasi cell • “The most anterior ethmoid cell”
• Swelling along lateral nasal wall anterior to middle turbinate vertical attachment (endoscopic view)
• Pneumatization of the agger nasi region
• Well seen on sagittal and coronal CT images Frontal cell (type 1) • Single anterior ethmoid cell above the agger nasi cell
• Posterior wall is not skull base;posterior wall is free partition in the frontal recess
• Well seen on coronal and sagittal CT images
Frontal cell (type 2) • Tier of 2 or more anterior ethmoid cells that pneumatize above the agger nasi cell
• Posterior wall is not skull base;posterior wall is free partition in the frontal recess
• Well seen on coronal and sagittal CT images
Frontal cell (type 3) • Single large anterior ethmoid cell above the agger nasi cell
• Pneumatizes along inner aspect of the anterior frontal sinus table from the anterior frontal recess
• Extends far into true frontal sinus;superior wall (cap) inserts upon inner aspect of the anterior frontal sinus table (seen on sagittal CT image)
• Posterior wall is not skull base;posterior wall is free partition in the frontal recess
• Well seen on coronal and sagittal CT images
Frontal cell (type 4) • Apparently isolated cell within frontal sinus and above the agger nasi cell
• Appears as an “air bubble” on coronal CT scan
• Appears as a “balloon on a string” on sagittal CT scan
• The anterior/inferior margin is anterior frontal sinus table or frontal sinus floor
• The posterior boundary is cell wall, not posterior frontal sinus table.
• Identification requires both sagittal and coronal CT
Supraorbital ethmoid cell • Ethmoid cell that extends over the orbit from the frontal recess
• May be single or multiple
• May mimic the appearance of a septate frontal sinus
• Opens into the lateral aspect of the frontal recess (this opening is lateral and posterior to the true frontal sinus ostium)
• Identification requires review of both axial and coronal CT images Interfrontal sinus septal cell • Pneumatization of the frontal sinus septum
• Drains into one frontal recess
• Associated with pneumatized crista galla
• Well seen on axial and coronal sinus CT
Adopted from 3D computed tomographic analysis of frontal recess anatomy in patients without frontal sinusitis, Otolaryngology-Head and Neck Surg 2004;131:164-73
조사하였고, 각 해부학적 변이와 전두동염과의 통계적 의의 를 알아보기 위해 Pearson ’s chi-square test를 이용하였 고 통계 프로그램은 SPSS version 12.0(SPSS, Chicago, USA)을 사용하였다.
결 과
연구에 포함된 317예 중 남자가 144예, 여자가 173예였으 며 평균나이는 41세였다.
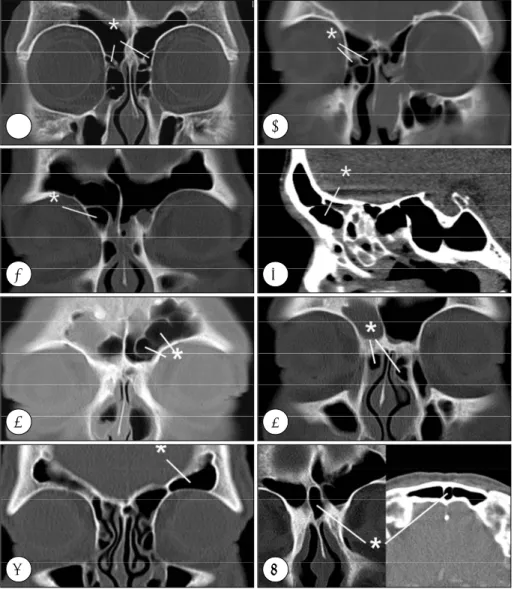
317예의 634측 중 21.6%에서 전두봉소가 존재하였으며 제 1형 전두봉소(Fig. 1A)가 13.6%, 제2형 전두봉소(Fig. 1B)가 3.2%, 제3형 전두봉소(Fig. 1C, D)가 1.9%였고 제4형 전두 봉소(Fig. 1E)가 3.1%였다. 전두봉소가 존재한 경우 24.1%
에서 전두동염을 보였으나 전두동염과의 유의한 관련은 없 었고, 제1형의 경우 20.9%, 제2형은 15%, 제3형은 16.7%에 서 전두동염이 동반되었는데, 역시 전두동염과 유의한 관련
성은 없는 것으로 나타났다. 그러나 제4형은 52.6%에서 전 두동염이 동반되는 것으로 나타나 전두동염과 통계적으로 유 의한 관련성이 있었다(p<0.001)(Table 2). 전두봉소의 유무 에 따른 해부학적 변이와의 관계에 있어서 전두봉소가 존재 하는 군에서 비제봉소(p<0.001), 상안와 사골봉소(p=0.002), 전두동간 중격봉소(p=0.006)가 통계적으로 유의하게 높은 빈도로 나타났다.
또한 전두봉소가 존재하는 군에서 전두동의 과함기화가 유 의하게 높은 빈도로 나타났으며, 전두봉소가 없는 군에서 전 두동의 저함기화가 유의하게 높은 빈도로 나타냈다(p<0.001) (Table 3).
비제봉소(Fig. 1F)는 67.8%에서 관찰되었다. 비제봉소가 존재한 429측 중 16.8%에서 전두동염을 보였고 비제봉소가 없는 경우 28.1%에서 전두동염이 나타나, 비제봉소가 없는 경우와 전두동염간에 통계학적으로 유의한 관련성이 있었다 (p=0.010)(Table 4).
A B
C D
E F
G H
Fig. 1. Paranasal sinus CT scans repre- senting frontal recess cells. A:Type 1 frontal cells (*) are seen above the ag- ger nasi cell. B:Type 2 frontal cells (*), a tier of frontal cells above an agger nasi cell. C, D:A type 3 frontal cell (*), which occurs above the agger nasi cell and enters the true frontal sinus.
E:Type 4 frontal cells (*), apparently isolated within frontal sinus. F:Bilateral agger nasi cells (*). G:A supraorbital ethmoid cell (*) which pneumatizes over the orbit. H:An interfrontal sinus septal cell (*) appears as a central compartment within the frontal bone.
상안와 사골봉소(Fig. 1G)는 7.7%에서 관찰되었고, 상안 와 사골봉소가 존재한 49측 중 24.5%에서 전두동염이 동반 되어, 상안와 사골봉소가 없는 경우보다 다소 높은 빈도를 보였으나 통계적인 유의성은 없었다(Table 4).
전두동간 중격봉소(Fig. 1H)는 14.5%에서 관찰되었으며, 전두동간 중격봉소가 존재한 92측 중 22.8%에서 전두동염 을 보였으나 전두동간 중격봉소가 없는 경우와 유의한 차이 는 없었다(Table 4).
구상돌기의 부착형태는 Stammberger의 분류를 기준으로 제I형이 73.5%, 제II형이 16.7%, 제III형이 9.8%였다. 구상 돌기의 부착형태에 따른 전두동염과의 관계는 제I형의 22.9%, 제II형의 15.1%, 제III형의 9.7%에서 전두동염을 보여 제I형 이 전두동염과 가장 유의한 관련성이 있는 것으로 나타났다 (p=0.017)(Table 4).
전두동이 과함기화된 경우가 24.0%에서 관찰되었으며 저 함기화된 경우가 17.0%였다. 전두동이 과함기화된 경우의 22.4%에서 전두동염이 동반되었으나 통계학적 유의성은 없 었다. 저함기화된 경우에서는 12.9%에서 전두동염이 존재 한 반면, 저함기화가 동반되지 않은 경우에서는 21.9%에서 전두동염이 나타나, 전두동이 저함기화된 경우에서 전두동 염이 나타나는 빈도가 유의하게 낮았다(p=0.036)(Table 4).
고 찰
전두동염에 대한 수술은 전두동천공술 등의 고전적 술식 에서부터 골성형피판전두동폐쇄술 및 내시경적 수술까지 많 은 변화를 보여왔고, 근래에 부비동 내시경의 발달로 인해 내시경적 전두동 수술이 보편화되었다. 그러나 전두동염의 비내시경적 접근은 전두와 주위의 협소하고 복잡한 해부학 적인 구조와 전사골동맥, 두개기저부, 지판 등 주변의 중요 구조물의 손상위험으로 인해 내시경적 접근이 어려운 경우 가 많고 잔존 병소로 인해 재수술이 필요한 경우가 많다.3) 따라서 전두동의 내시경적 접근을 위해서는 전두와의 복잡 한 해부학적 구조를 정확하게 파악해야 하며 이를 위해서는 전두와 봉소의 종류와 그 발현빈도에 대해 숙지하는 것이 필 수적이다.
전두봉소는 1916년 Schaeffer에 의해 처음 명명되었으며,8)
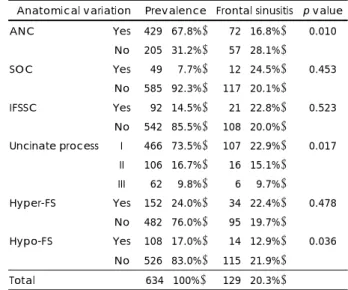
Table 4. The association of anatomical variations with frontal si- nusitis
Anatomical variation Prevalence Frontal sinusitis p value Yes 429 (67.8%) 072 (16.8%) 0.010 ANC
No 205 (31.2%) 057 (28.1%)
Yes 049 (07.7%) 012 (24.5%) 0.453 SOC
No 585 (92.3%) 117 (20.1%)
Yes 092 (14.5%) 021 (22.8%) 0.523 IFSSC
No 542 (85.5%) 108 (20.0%) I 466 (73.5%) 107 (22.9%) II 106 (16.7%) 016 (15.1%) Uncinate process
III 062 (09.8%) 006 (09.7%)
0.017
Yes 152 (24.0%) 034 (22.4%) 0.478 Hyper-FS
No 482 (76.0%) 095 (19.7%)
Yes 108 (17.0%) 014 (12.9%) 0.036 Hypo-FS
No 526 (83.0%) 115 (21.9%)
Total 634 (100%) 129 (20.3%)
ANC:agger nasi cell, SOC:supraorbital ethmoid cell, IFSSC:
interfrontal sinus septal cell, Hyper:hyperpneumatized, Hypo:
hypopneumatized, FS:frontal sinus, Yes:presence of anatom- ical variation, No:absence of anatomical variation, I, II, III:type I, II, III of uncinate process attachment according to Stammber- ger classification
Table 3. The association of frontal cells with anatomical variations A
All individuals (n=634)
B
Individuals with FCs (n=137)
C
Individuals without FCs (n=497) p value (B vs C)
FC 137 (21.6%) - - -
ANC 429 (67.8%) 114 (83.2%) 315 (63.4%) <0.001
SOC 049 (07.7%) 019 (13.9%) 030 (06.0%) <0.002
IFSSC 092 (14.5%) 030 (21.9%) 062 (12.5%) <0.006
Hyper-FS 152 (24.0%) 056 (40.3%) 096 (19.3%) <0.001
Hypo-FS 108 (17.0%) 008 (05.8%) 100 (20.1%) <0.001
FC:frontal cell, ANC:agger nasi cell, SOC:supraorbital ethmoid cell, IFSSC:interfrontal sinus septal cell, Hyper-:hyperpneumatized, Hypo-:hypopneumatized, FS:frontal sinus
Table 2. The association of frontal cells (Bent’s classification) with frontal sinusitis
Prevalence Frontal sinusitis p value FC (type 1) Yes 086 (13.6%) 018 (20.9%)
No 548 (86.4%) 111 (20.3%) <0.727 FC (type 2) Yes 020 (03.2%) 003 (15.0%)
No 614 (96.8%) 126 (20.5%) <0.631 FC (type 3) Yes 012(01.9%) 002 (16.7%)
No 622 (98.1%) 127 (20.4%) <0.818 FC (type 4) Yes 019 (03.1%) 010 (52.6%)
No 615 (96.9%) 119 (19.3%) <0.001 Any FC (type 1-4) Yes 137 (21.6%) 033 (24.1%)
No 497 (78.4%) 096 (19.3%) <0.219
Total 634 (100%) 129 (20.3%)
FC:frontal cell
1941년 Van Alyea 등9)이 242예의 사체해부를 통하여 119예 를 보고하였다. 1994년 Bent 등1)이 전산화단층촬영에 근거 하여 전두봉소를 제1형부터 제4형까지 분류하였으며 전두봉 소를 전두동염의 원인이 될 수 있다고 주장하였다. 한국인에 서 전두봉소 출현 빈도는 연구자 및 부비동염의 동반 유무 에 따라 8.8%에서 39.1%까지 다양하게 보고되고 있다.2)4) 본 연구에서는 21.9%의 빈도로 나타났는데, 다른 보고에서 와 마찬가지로 제1형 전두봉소가 가장 많은 빈도로 나타났 으며 다른 보고들에 비해 제3형과 제4형 전두봉소가 비교적 높은 빈도로 나타났다.
Lee 등4)은 한국인 225명의 450측을 분석하여 39.1%에서 전두봉소의 발현을 보고하였고, 이 중 제4형 전두봉소는 전 두동염과 유의한 연관성이 있다고 보고하였다. Meyer 등7)은 768명을 분석하여 제3형 및 4형 전두봉소는 전두봉소가 없 는 경우에서보다 전두동 점막의 비후와 통계적으로 높은 빈 도로 관찰된다고 보고하였다. 그러나 DelGaudio 등10)은 117 명의 환자를 대상으로 시상면을 포함한 전산화단층촬영을 분 석하여 전두봉소와 전두동염간에는 유의한 상관관계가 없는 것으로 보고하였다. 이렇듯 전두봉소와 전두동염과의 관련 성에 대한 연구들은 서로 상반된 결과를 보이고 있는데, 본 연구에서는 제4형 전두봉소만이 전두동염과 유의하게 연관 성을 보여 한국인을 대상으로 하였던 Lee 등4)의 연구결과 와 일치하였다. 그러나 해부학적으로 제4형 전두봉소보다 좀 더 전두동염과 연관성이 있을 것으로 예상되었던 제3형 전 두봉소는 전두동염과 관련성이 없는 것으로 나타났는데, 이 는 연구대상이 된 634측 중 제3형 전두봉소가 존재하는 경 우가 12측에 불과해 의미있는 분석이 되지 않았을 수 있으 며, 전두봉소의 존재 그 자체보다는 전두봉소의 크기, 전두 동의 유출로를 막고 있는 정도 등의 더 세분화된 인자들에 의한 것일 가능성도 있으므로 좀 더 많은 대상을 이용하여 이러한 인자들에 대한 분석이 이루어져야 한다.
전두봉소와 다른 해부학적 변이들과의 연관성을 알아본 결과, 전두봉소가 존재하는 경우 전두동의 과함기화가 유의 하게 높은 빈도를 보였고, 전두봉소가 존재하지 않는 경우 전두동의 저함기화가 유의하게 높은 빈도를 보였다. 또한, 과함기화된 전두동이 전두봉소를 동반하는 경우가 36.8%나 되는 반면, 저함기화된 전두동이 전두봉소를 동반하는 경우 가 7.4%에 불과해, 함기화가 잘 된 전두동을 수술할 때 술 전에 전두봉소의 존재를 더 면밀히 관찰한 뒤 수술에 임해 야 할 것으로 생각된다. 그리고 전두봉소가 존재하는 경우에 비제봉소와 상안와 사골봉소, 전두동간 중격봉소가 유의하 게 높은 빈도로 나타났는데, 이러한 현상은 전두동의 함기 화정도 뿐만 아니라 전두봉소나 비제봉소, 상안와 사골봉소
등의 함기화와 관련된 해부학적 변이들이 비강측벽의 발생 과정에서 동일한 요인에 의해 영향을 받기 때문인 것으로 생 각된다.6)
비제봉소가 존재하는 빈도는 컴퓨터단층촬영을 이용한 분석 에서 52.9%에서 98.5%까지 다양하게 보고되고 있으며,3)4)10-13) 본 연구에서는 67.8%로 나타났다. Bradley 등14)은 내시경적 부비동 수술 후 재발한 전두동염은 비제봉소의 점막병변 존 재유무와 유의한 상관관계가 있다고 하였고, Lee 등4)은 비 제봉소의 존재와 전두동염 간에 유의한 상관관계가 있다고 보고하였다. 그러나 이들보다 많은 수의 연구결과들이 비제 봉소와 전두동염간에는 유의한 관련성이 없다고 보고하고 있다.3)12)15)16)
본 연구에서는 비제봉소가 존재하는 경우보다 오히려 비제봉소가 없는 경우에서 전두동염이 동반되는 비 율이 높았는데, 이는 비제봉소의 존재는 전두동염의 발생과 관련이 없음을 보여준다. 비제봉소가 없는 경우에서 전두동 염의 비율이 더 높게 나온 원인으로 여러 가지를 추측해볼 수 있는데, 비제봉소가 없을 경우 동반될 수 있는 기능적·
해부학적 이상이 전두동염의 유발인자가 될 수 있고, 본 연 구에서 비제봉소가 나타난 비율이 67.8%로 비교적 낮게 나 온 것으로 미루어 볼 때 비제봉소로 판정하는 기준에 대한 견해가 관찰자마다 조금씩 차이가 날 수 있기 때문일 수도 있다. 하지만 전두동염이 없는 환자의 89%에서도 비제봉소 가 존재하며,5) 비제봉소가 전체 성인에 존재하는 비율이 90%
이상이라고 보고한 연구결과들3)4)13)14)이 있음을 감안해 보면, 비제봉소의 존재 자체가 전두동염의 발생에 영향을 주는 것 이 아니라 비제봉소의 크기와 전두동 유출로를 막고 있는 정 도가 전두동염의 병인에 중요할 것으로 생각된다.
상안와 사골봉소와 전두동간 중격봉소는 각각 7.7%와 14.5%
에서 관찰되어 다른 보고들과 유사한 빈도를 보였으며, 구 상돌기의 형태에 따른 빈도 또한 기존의 보고들과 큰 차이 가 없었다.14)17)18) 구상돌기의 부착형태와 전두동염간의 관련 성을 조사한 연구들을 고찰해 보면, 구상돌기의 부착형태와 전두동염간에 관련성이 없다는 연구들과,3)4) 전두동의 유출 로가 누두(infundibulum)가 아닌 중비도로 연결된 경우에 서 전두동염이 높은 반도로 나타난다는 주장으로 양분되어
있는데,2)19) 본 연구에서는 구상돌기가 지판에 부착된 제1형
에서 전두동염과의 연관성이 가장 높았다. 이는 비강 내에 존 재하는 염증을 일으킬 수 있는 물질들이 누두보다 중비도를 통해 전두동및 전두와로 침입하기 쉽기 때문이라는 추측을 해볼 수 있으나 증명된 바는 없다. 그리고 전두동의 저함기 화가 있을 경우 전두동염이 동반되는 빈도가 통계적으로 의 미있게 낮았는데, 전두동 자연공의 크기가 동일하다면 염증 시에 생성되는 분비물의 양이 저함기화된 전두동에서는 상
대적으로 적으므로 분비물이 정체되지 않고 배출되기에 유 리하기 때문이 아닐까하는 가정을 해볼 수 있다.
본 연구는 비부비동과 관련된 증상을 호소하는 환자들만 을 대상으로 하였기 때문에 일반인구 전체를 대변하지 못하 는 한계점이 있으며, 또한 전두와 주위의 광범위한 병변으로 인해 해부학적인 구조의 확인이 불가능한 경우를 제외하였 기 때문에 전두봉소나 전두동염의 빈도가 과소평가 되었을 가능성이 있다. 향후에는 최근 부비동의 해부학적 연구에 이 용되고 있는 1∼1.25 mm 두께의 단층촬영을 이용하여 전 두동의 전두봉소의 크기와 위치, 전두동의 유출로를 막고 있 는 정도가 전두동염의 발생에 미치는 영향을 조사해야할 것 으로 사료된다.
결 론
전두봉소가 존재하면 비제봉소, 상안와 사골봉소, 전두동 간 중격봉소, 전두동의 과함기화가 동반되는 빈도가 증가한 다. 그리고 전두봉소의 종류, 구상돌기의 부착형태, 전두동 의 함기화 정도는 전두동염과 관련이 있는 것으로 생각되므 로, 전두동염에 대한 내시경 수술시 특히 이들 구조물의 존 재여부와 그 형태를 사전에 숙지하고 수술에 임해야할 것으 로 사료된다.
중심 단어:전두와 봉소·전두동염·전산화단층촬영.
REFERENCES
1) Bent JP, Cuilty-Siller C, Kuhn FA. The frontal cell as a cause of fron- tal sinus obstruction. Am J Rhinol 1994;8:185-91.
2) Shin SH, Lee HS, Park JY. Computed tomographic findings of fron- tal sinusitis. Korean J Otolaryngol-Head Neck Surg 1997;40:169-74.
3) Min YG, Choo MJ, Rhee CS, Jin HR, Shin JS, Cho YS. CT analysis of the paranasal sinuses in symptomatic and asymptomatic groups.
Korean J Otolaryngol-Head Neck Surg 1993;36:916-24.
4) Lee JH, Lee SO. Frontal sinusitis related to anatomic variations. Ko- rean J Otolaryngol-Head Neck Surg 2004;47:751-5.
5) Lee WT, Kuhn FA, Citardi MJ. 3D computed tomographic analysis of frontal recess anatomy in patients without frontal sinusitis. Otolar- yngol Head Neck Surg 2004;131:164-73.
6) Stammberger HR, Kennedy DW. Paranasal sinuses: Anatomic termi- nology and nomenclature. Ann Otol Rhinol Laryngol Suppl 1995;
167:7-16.
7) Meyer TK, Kocak M, Smith MM, Smith TL. Coronal computed to- mography analysis of frontal cells. Am J Rhinol 2003;17:163-8.
8) Schaeffer JP. Further observations on the anatomy of the sinus fron- talis in man. Ann Surg 1916;64:665-71.
9) Van Alyyea OE. Frontal cells: An anatomic study of these cells with consideration of their clinical significance. Arch Otol 1941;34:11-23.
10) Krzeski A, Tomaszewska E, Jakubczyk I, Galewicz-Zielinska A. An- atomic variations of the lateral nasal wall in the computed tomog- raphy scans of patients with chronic rhinosinusitis. Am J Rhinol 2001;
15:371-5.
11) Landsberg R, Friedman M. A computer-assisted anatomical study of the nasofrontal region. Laryngoscope 2001;111:2125-30.
12) DelGaudio JM, Hudgins PA, Venkatraman G, Beningfield A. Multi- planar computed tomographic analysis of frontal recess cells. Arch Otolaryngol Head Neck Surg 2005;131:230-5.
13) Bolger WE, Butzin CA, Parsons DS. Paranasal sinus bony anatomic variation and mucosal abnormalities: CT analysis for endoscopic si- nus surgery. Laryngoscope 1991;101:56-64.
14) Bradley DT, Kountakis SE. The role of agger nasi air cells in patients requiring revision endoscopic frontal sinus surgery. Otolaryngol Head Neck Surg 2004;131:525-7.
15) Kim HJ, Jung Cho M, Lee JW, Tae Kim Y, Kahng H, Sung Kim H, et al. The relationship between anatomic variations of paranasal si- nuses and chronic sinusitis in children. Acta Otolaryngol 2006;126 (10):1067-72.
16) Al-Qudah M. The relationship between anatomical variations of the sino-nasal region and chronic sinusitis extension in children. Int J Pediatr Otorhinolaryngol 2008;72(6):817-21.
17) Wormald PJ. The agger nasi cell: The key to understanding the anat- omy of the frontal recess. Otolaryngol Head Neck Surg 2003;129:
497-507.
18) Owen RG, Kuhn FA. Supraorbital ethmoid cell. Otolaryngol Head Neck Surg 1997;116:254-61.
19) Turgut S, Ercan I, Sayin I, Başak M. The relationship between fron- tal sinusitis and localization of the frontal sinus outflow tract: a com- puter-assisted anatomical and clinical study. Arch Otolaryngol Head Neck Surg 2005;131(6):518-22.