27
Corresponding to: Dong Yi Kim, Department of Surgery, Chonnam National University Medical School, 8, Hak 1-dong, Dong-gu, Gwangju 501-757, Korea. Tel: 062-220-6456, Fax: 062-227-1635, E-mail: [email protected].
Received March 7, 2008, Accepted April 7, 2008
Survival of Node-Positive Mucosal Gastric Carcinoma Patients
Department of Surgery, Chonnam National University Medical School, Gwangju, Korea
Yong Chul Cho, M.D., Ho Goon Kim, M.D., Mi Ran Jung, M.D., Seong Yeob Ryu, M.D., Young Kyu Park, M.D., Dong Yi Kim, M.D. and Young Jin Kim
Purpose: The presence or absence of lymph node metastasis is significantly associated with the survival of patients
with gastric carcinoma. We compared node-positive and node-negative mucosal gastric carcinoma patients to identif y the clinicopathological characteristics of node-positive mucosal gastric carcinoma. We also evaluated the variables associated with lymph node metastasis and survival in this group of patients.
Methods: Of the 580 mucosal gastric carcinoma patients, 32 (5.5%) were node-positive. A statistical analysis using
the Cox model was performed to determine the factors that can predict the patients' outcomes.
Results: The mean tumor size was significantly larger in the patients with node-positive mucosal gastric carcinoma
than that in the node-negative patients (3.3 vs. 1.8 cm; P<0.001). The overall survival rate was lower for the patients who were node-positive than for the patients who were node-negative (83.3% vs. 91.4%, respectively), but the difference was not significant (P>0.05). Using the Cox proportional hazard regression model, tumor size was an independent statistically significant parameter associated with lymph node metastasis (risk ratio: 4.70, 95%
confidence interval: 1.20 to 18.35; P<0.05).
Conclusion: Tumor size is the most reliable predictor of lymph node metastasis for patients with node-positive
mucosal gastric carcinoma. Nevertheless, a large tumor size is not associated with a poor outcome for patients with node-positive mucosal gastric carcinoma. The patients with node-positive mucosal gastric carcinoma showed good survival rates after undergoing gastrectomy and extensive node dissection. (J Korean Surg Soc 2008;75:27-31)
Key Words: Gastric carcinoma, Node-positive, Mucosal, survival, Tumor sizeINTRODUCTION
Of the clinicopathological factors influencing the prognosis of patients with gastric carcinoma, the presence or absence of lymph node metastasis is one of the most important prognostic factors.(1-4) There are few reports on prognostic factors in patients with node-positive mucosal gastric carcinoma.(5,6) We compared node-positive and node-negative mucosal gastric carcinoma patients to identify the clinicopathological characteristics of node-positive mu- cosal gastric carcinoma. We also evaluated outcome indi-
cators in this group of patients.
METHODS
Between 1992 and 2001, 580 patients with mucosal gastric carcinoma were treated in the Chonnam National University Hospital Hospital Of these, 32 (5.5%) were node-positive. The clinicopathological characteristics of these patients with node-positive mucosal gastric carcinoma were reviewed retrospectively. The macroscopic and histological evaluation followed the Japanese General Rules for Gastric Cancer Study.
(7) Twenty-seven patients (84.4%) had pN1 metastasis. In five patients, metastasis was seen N2 nodes (along the left gastric, common hepatic, celiac arteries).
Our standard procedure is gastrectomy with dissection
above the D2 lymph node. Patient follow-up lasted until
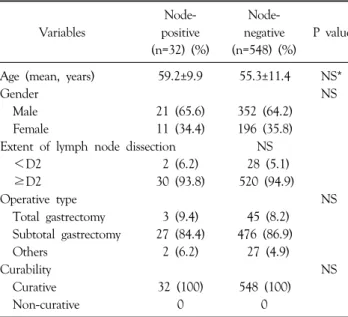
Table 1. Clinical features of patients with node-positive and -negative mucosal gastric carcinoma
Node- Node-
Variables positive negative P value
(n=32) (%) (n=548) (%) Age (mean, years) 59.2±9.9 55.3±11.4 NS*
Gender NS
Male 21 (65.6) 352 (64.2)
Female 11 (34.4) 196 (35.8)
Extent of lymph node dissection NS
<D2 2 (6.2) 28 (5.1)
≥D2 30 (93.8) 520 (94.9)
Operative type NS
Total gastrectomy 3 (9.4) 45 (8.2) Subtotal gastrectomy 27 (84.4) 476 (86.9)
Others 2 (6.2) 27 (4.9)
Curability NS
Curative 32 (100) 548 (100)
Non-curative 0 0
*NS, not significant.
Table 2. Histopathologic features of of patients with node-positive and -negative mucosal gastric carcinoma
Node- Node-
Variables positive negative P value
(n=32) (%) (n=548) (%) Tumor size (mean, cm) 3.3±2.2 1.8±1.1 <0.001
<2 cm 9 (28.1) 338 (61.7)
≥2 cm 23 (71.9) 210 (38.3)
Tumor location NS*
Upper 3 (9.4) 16 (2.9)
Middle 8 (25.0) 178 (32.5)
Lower 21 (65.6) 354 (64.6)
Macroscopic type NS
Elevated 7 (21.9) 113 (20.6)
Depressed 22 (68.7) 379 (69.2)
Flat 3 (9.4) 56 (10.2)
Histologic type NS
Well-differentiated 8 (25.0) 162 (29.6) Moderately differentiated 7 (21.9) 122 (22.3) Poorly differentiated 11 (34.4) 157 (28.7)
Mucinous 2 (6.2) 5 (0.9)
Signet ring cell 4 (12.5) 100 (18.2)
Others 0 2 (0.3)
Hepatic metastasis NS
H (−) 32 (100) 548 (100)
H (+) 0 0
Peritoneal dissemination NS
P (−) 32 (100) 548 (100)
P (+) 0 0
Stage < 0.001
1 27 (84.4) 548 (100)
2 5 (15.6) 0
*NS, not significant.
death or until the cut-off date of December 31, 2001. At the time of the last follow-up, one patient (3.1%) had been lost to follow-up. The mean follow-up interval for patients at the cut-off date was 84 months. Generally, patients return every 3 months for the first 2 years and then every 6 months until at least the end of the fifth year.
The survival rates of the patients were calculated using the Kaplan-Meier method, and differences between the curves were tested by the log rank test. The relative prognostic importance of the parameters was investigated using the Cox proportional hazards model. The chi-square test was used to evaluate the statistical significance of dif- ferences, and P<0.05 was considered statistically significant.
RESULTS
Table 1 summarizes the clinical findings of the 32 (5.5%) patients with node-positive mucosal gastric carcinoma and the 548 (94.5%) patients with node-negative mucosal gastric carcinoma. There were more males than females in each group, but the gender ratio was the same. A D2 lymphadenectomy was performed in 30 patients (93.8%), whereas the dissection was limited to D1 in two patients (6.2%). Subtotal gastrectomy was the procedure performed
most frequently (84.4% of cases) in patients with node- positive mucosal gastric carcinoma. The curative resection rate was 100% in both groups.
The histopathological characteristics are listed in Table
2. The mean tumor size was significantly larger in patients
with node-positive than node-negative mucosal gastric
carcinoma (3.3 vs. 1.8 cm; P<0.001). Most gastric carci-
nomas were located in the lower third of the stomach both
in patients with node-positive (21 cases; 65.6%) and
node-negative (354 cases; 64.6%) mucosal gastric carcinoma,
and the differences in location were not significant. Of the
patients with node-positive mucosal gastric carcinoma, five
(15.6%) were classified as stage II at the time of initial
diagnosis, whereas all of the patients with node-negative
Table 4. Node-positive mucosal gastric carcinoma: multivariate analysis of factors associated with survival rates Variables Risk ratio 95% CI† P value
Age (years) 1.53 0.27∼8.85 NS*
(<65 vs.≥65)
Gender 3.13 0.71∼17.41 NS
(male vs. female)
Tumor size (mm) 4.43 2.21∼12.35 NS
(<20 vs.≥20)
Histologic type 1.28 0.34∼6.73 NS
(differentiated vs.
undifferentiated)
Macroscopic type 1.76 0.33∼9.45 NS
(elevated vs. depressed)
*NS = not significant; †CI = confidence interval.
Fig. 1. Survival curves of patients with node-negative and -positive mucosal gastric carcinoma (91.4% vs. 83.3%) (P=0.509).
Table 3. Early gastric carcinoma with mucosal invasion: multivariate analysis of factors associated with lymph node metastasis Variables Risk ratio 95% CI† P value
Age (years) 1.46 0.38∼5.65 NS*
(<65 vs.≥65)
Gender 2.13 0.61∼7.41 NS
(male vs. female)
Location 0.97 0.75∼1.24 NS
(middle vs. distal)
Tumor size (mm) 4.70 1.20∼18.35 <0.05
(<20 vs.≥20)
Histologic type 1.53 0.44∼5.34 NS
(differentiated vs.
undifferentiated)
Macroscopic type 1.62 0.31∼8.52 NS
(elevated vs. depressed)
*NS = not significant; †CI = confidence interval.
mucosal gastric carcinoma were classified as stage I at the time of initial diagnosis (P<0.001).
The overall survival rate was lower for patients with node-positive than node-negative mucosal gastric carcinoma (83.3% vs. 91.4%), but the difference was not significant (P=0.509; Fig. 1). The clinicopathological variables associated with lymph node metastasis tested in the multivariate analysis are shown in Table 3. Using Cox's proportional hazard regression model, tumor size was an independent statistically significant parameter associated with lymph node metastasis (risk ratio 4.70, 95% confidence interval 1.20, 18.35; P<0.05). Variable factors for survival in patients with node-positive mucosal gastric carcinoma were tested (Table 4).
DISCUSSION
Although most patients with early gastric carcinoma (EGC) have a good prognosis, some will have recurrence and poor survival. Identifying the factors associated with poor survival in patients with EGC is important. It is known that lymph node involvement is the most important factor determining the prognosis of EGC. We compared node-positive and node-negative mucosal gastric carcinoma
patients to identify the clinicopathological characteristics of node- positive mucosal gastric carcinoma. We also eva- luated the variables associated with lymph node metastasis and survival outcome in this group of patients.
The reported rates of lymph node involvement from
mucosal gastric carcinoma range from 1 to 7%.(6,8-10)
Various risk factors for nodal metastasis from EGC have
been discussed. Large tumor size, macroscopically depressed
type, histologically undifferentiated type, and an intra-
tumoral ulcer or ulcer scar are reported risk factors for
lymph node metastasis.(11) Using Cox's proportional
hazard regression model, we found that tumor size was
determined to be an independent statistically significant parameter associated with lymph node metastasis in mucosal gastric carcinoma (risk ratio 4.70, 95% confidence interval 1.20, 18.35; P<0.05).
It is controversial whether tumor size is independently correlated with prognosis. Some investigators emphasize that tumor size is an independent prognostic factor, whereas others state that tumor size does not independently influence the survival of patients. Adachi et al.(12) reported that tumor size was a simple prognostic indicator for gastric carcinoma. By contrast, Yokota et al.(13) reported that the presence of lymph node metastasis, depth of invasion, and tumor location were more important than tumor size. We found that node-positive patients were characterized by a larger tumor size than in node-negative patients (3.3 vs. 1.8 cm), and tumor size was the one reliable factor associated with lymph node metastasis. Nevertheless, we found no significant difference in the overall survival rate between the two groups studied.
Surgery is the only potentially curative modality for gastric carcinoma.(12) However, the recommended extent of lymph node dissection in patients with EGC remains controversial.(14) Nakamura et al.(15) proposed gastrectomy with D1 or D2 lymph node dissection for EGC, based on tumor size and depth. The German Gastric Cancer Study group showed no difference in survival between stage I patients after D1 and D2 lymph node dissection.(16) Contrasting their results, some investigators reported that extended lymphadenectomy is a significant prognostic factor for patients with EGC.(5,17,18) Adachi et al.(19) emphasized that the macroscopic diagnosis of lymph node involvement is unreliable and recommended D2 lymph node dissection for curative treatment in patients with node-negative gastric carcinomas. Gunji et al.(20) also reco- mmended D2 extended lymphadenectomy as the standard treatment modality for EGC based on reports of metastatic lymph nodes downstream from the perigastric lymph nodes in patients with EGC.(21) Yamaguchi et al.(5) reported that 29% of node-positive mucosal gastric carcinoma was seen in Japanese N2 nodes metastasis (along the left gastric, common hepatic, splenic or celiac arteries) and two cases
had metastasis in the para-aortic nodes. They recommended that appropriate lymph node dissection for node-positive mucosal gastric carcinoma patients.
The prognosis in EGC is generally favourable. Especially in patients with mucosal carcinoma, the 5-year survival rate exceeds 95 per cent in patients without lymph node metastasis, and around 85 per cent or higher, even in those with lymph node metastasis. Some investigators reported that the presence of lymph node metastasis in EGC worsened the prognosis.(22,23) The prognosis of patients with metastases of N2 nodes is poor, the 5-year survival rate being less than 50 per cent8. We found that 5 patients (15.6%) had pN2 nodes metastasis in this study. Our standard treatment for EGC is radical gastric resection with dissection above the D2 lymph node and we performed extensive lymph node dissection in 93.8% of the patients with node-positive mucosal gastric carcinoma in our series.
This could explain the high survival rate in patients with node-positive mucosal gastric carcinoma (83.3%), regardless of lymph node involvement.
In conclusion, we found that tumor size is the most reliable predictor of lymph node metastasis for patients with mucosal gastric carcinoma. Nevertheless, large tumor size is not associated with a poor outcome for patients with node-positive mucosal gastric carcinoma. The prognosis of patients with node-positive mucosal gastric carcinoma was good after gastrectomy and extensive node dissection.
REFERENCES
1) Bozzetti F, Bonfanti G, Morabito A, Bufalino R, Menotti V, Andreola S et al. A multifactorial approach for the prognosis of patients with carcinoma of the stomach after curative resection. Surg Gynecol Obstet 1986;162:229-34.
2) Maruyama K. The most important prognostic factors for gastric cancer patients. Scand J Gastroenterol 1987;22:63-8.
3) Adachi Y, Ogawa Y, Sasaki Y, Yukaya H, Mori M, Sugimachi K. A clinicopathologic study of gastric carcinoma with reference to age of patients. J Clin Gastroenterol 1994;18:287-90.
4) Siewert Jr, Bottcher K, Stein HJ, Roder JD. Relevant pro- gnostic factors in gastric cancer: ten-year results of the German Gastric Cancer Study. Ann Surg 1998;228:449-61.
5) Yamaguchi T, Sano T, Katai H, Sasako M, Maruyama K.
Node-positive mucosal gastric cancer: a follow-up study. Jpn J
Clin Oncol 2001;31:153-6.
6) Song SY, Park S, Kim S, Son HJ, Rhee JC. Characteristics of intramucosal gastric carcinoma with lymph node metastatic disease. Histopathology 2004;44:437-44.
7) Japanese Gastric Carcinoma Association. Japanese classification of gastric carcinoma. Gastric Cancer 1998;1:10-24.
8) Korenaga D, Haraguchi M, Tsujitani S, Okamura T, Tamada R, Sugimachi K. Clinicopathological features of mucosal carcinoma of the stomach with lymph node metastasis in eleven patients. Br J Surg 1986;73:431-3.
9) Nakamura K, Ueyama T, Yao T, Xuan ZX, Ambe K, Adachi Y, et al. Pathology and prognosis of gastric carcinoma. Findings in 10,000 patients who underwent primary gastrectomy. Cancer 1992;70:1030-7.
10) Kim JP, Hur YS, Yang HK. Lymph node metastasis as a significant prognostic factor in early gastric cancer: analysis of 1,136 early gastric cancers. Ann Surg Oncol 1995;2:308-13.
11) Yamao T, Shirao K, Ono H, Kondo H, Saito D, Yamaguchi H, et al. Risk factors for lymph node metastasis from intra- mucosal gastric carcinoma. Cancer 1996;77:602-6.
12) Adachi Y, Oshiro T, Mori M, Maehara Y, Sugimachi K. Tumor size as a simple prognostic indicator for gastric carcinoma. Ann Surg Oncol 1997;4:137-40.
13) Yokota T, Ishiyama S, Saito T, Teshima S, Yamada Y, Iwamoto K, et al. Is tumor size a prognostic indicator for gastric carcinoma? Anticancer Res 2002;22:3673-7.
14) Park YK, Kim JC, Koh YS, Joo JK, Ryu SY, Kim YJ, et al.
Early gastric carcinoma in young patients. Int Surg 2006;91:
316-9.
15) Nakamura K, Morisaki T, Sugitani A, Oqawa T, Uchiyama A, Kinukawa N et al. An early gastric carcinoma treatment strategy
based on analysis of lymph node metastasis. Cancer 1999;85:
1500-5.
16) Siewert JR, Bottcher K, Roder JD, Busch R, Hermanek P, Meyer HJ. Prognostic relevance of systematic lymph node dissection in gastric carcinoma. German Gastric Carcinoma Study Group. Br J Surg 1993;80:1015-8.
17) Baba H, Maehara Y, Takeuchi H, Inutsuka S, Okuyama T, Adachi Y, et al. Effect of lymph node dissection on the prognosis in patients with node-negative early gastric cancer.
Surgery 1995;117:165-9.
18) Otsuji E, Toma A, Kobayashi S, Cho H, Okamoto K, Hagiwara A, et al. Long term benefit of extended lymphadenectomy with gastrectomy in distally located early gastric carcinoma. Am J Surg 2000;180:127-32.
19) Adachi Y, Mori M, Maehara Y, Kitano S, Sugimachi K.
Prognostic factors of node-negative gastric carcinoma: univariate and multivariate analyses. J Am Coll Surg 1997;184:373-7.
20) Gunji Y, Suzuki T, Hori S, Hayashi H, Matsubara H, Shimada H, et al. Prognostic significance of the number of metastatic lymph nodes in early gastric cancer. Dis Surg 2003;20:148-53.
21) Oertli D, Herzog U, Rothenbuhler JM, Torhorst J, Spichtin HP, Tondelli P, et al. Results following resection in early stomach carcinoma. Dtsch. Med. Wochenschr 1994;119:539- 43.
22) Maehara Y, Orita H, Okuyama T, Moriguchi S, Tsujitani S, Korenaga D, et al. Predictors of lymph node metastasis in early gastric carcinoma. Br J Surg 1992;79:245-7.
23) Kitamura K, Yamaguchi T, Taniguchi H, Hagiwara A, Sawai K, Takahashi T. Analysis of lymph node metastasis in early gastric carcinoma: rationale of limited surgery. J Surg Oncol 1997;64:42-7.