- 37 -
Effect of Roxithromycin and Intranasal Fluticasone Spray in Reducing Symptoms of Chronic Sinusitis, Polyp Size
and IL-4 in Allergic Patients
Byung-Guk Kim, M.D., Dong-Mok Lee, M.D., Jin-Hee Jo, M.D., Dae-Gun Jung, M.D., Jun-Myung Kang, M.D. and Sung-Won Kim, M.D.
ABSTRACT
Nasal polyp is an intractable condition usually associated with chronic hyperplastic sinusitis with allergic rhinitis. IL-4 is known to contribute to the inflammatory reaction by enhancing binding of inflammatory cells in the nasal polyp. The objectives of this study were to evaluate the effect of roxithromycin (300 mg daily) and intranasal fluticasone spray (200 μg daily ) in reducing symptoms of chronic sinusitis and polyp size and to compare pre - and post-treatment secretion of IL-4. Twenty-four patients with chronic sinusitis with nasal polyp and allergic rhinitis were selected and allocated into 3 groups;roxythromycin, fluticasone propionate and combined use group. Statistically significant decrease in symptoms was observed in both the roxythromycin and fluticasone propionate groups. Significant improvement of rhinorrhea and postnasal drip was observed in the combined use group. The polyp size decreased significantly in all three groups. IL-4 secretion decreased significantly in the combined use group after treatment. Long term medication of roxithromycin and intranasal fluticasone spray were effective in reducing symptoms and polyp size in chronic sinusitis with allergic rhinitis. They were also effective in reducing IL-4.
KEY WORDS
:Nasal polyp・Chronic sinusitis ・IL-4・Roxithromycin・Fluticasone propionate.
INTRODUCTION
Nasal polyp is an intractable condition commonly encountered in otolaryngologic clinics. Nasal polyp in adult patients is usually associated with extensive sinus mucosal thickening and is referred to as chronic hy- perplastic sinusitis with nasal polyp.
Although nasal polyp is the most common mass lesion arising within the nasal cavity, its etiology and pathogenesis have not yet been fully elucidated in spite of the numerous studies conducted by many inves-
tigators.
Some of the consistent observations in nasal polyp are universal presence of infection, frequent coexistence of respiratory allergy, poor response to therapy and high recurrence rate after surgical removal.
Medical treatment has been attempted to shrink the polyp size and to prevent recurrence. Antibiotic therapy may temporarily result in polyp remission, but in most patients it has had little therapeutic benefit. Oral ste- roids are valuable in shrinking the polyp and decreasing their vascularity. However, long term medication with this type of drug is not feasible because of the side effects, but topical application of steroid has been accepted as a new therapeutic modality.
Recent studies have shown long-term application of low dose roxithromycin, a 14-membered macrolide, to be effective in countering nasal polyp associated with chronic sinusitis.
1)Topical intranasal corticosteroids are also well known for reducing the size of polyps, suppressing formation of new polyps and inhibiting recurrence after poly- Department of Otorhinolaryngology-Head and Neck Surgery,
College of Medicine, The Catholic University of Korea, Seoul, Korea
Address correspondences and reprint requests to Byung-Guk Kim, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, The Catholic University of Korea, St. Paul’s Hospital, 620-56 Jeonnong 2-dong, Dongdaemun-gu, Seoul 130-709, Korea
Tel:82-2-958-2485, Fax:82-2-959-5375 E-mail:[email protected]
Accepted for publication on August 2, 2003
pectomy. It acts by interfering with the initial inflamm- atory reaction of polyp formation.
2)Fluticasone propionate is a fluorinated steroid, highly effective when used topically in the nose for allergic rhinitis.
Among various cytokines that influence inflamm- atory reaction in allergic rhinitis, IL-4 contributes to this mainly by enhancing the binding ability of lym- phocytes, monocytes, eosinophils and stimulating IgE production.
3)Recent studies have shown that supp- ression of IL-4 is induced by intranasal fluticasone spray.
4)The objectives of this study were to evaluate the effectiveness of roxithromycin (300 mg daily) and in- tranasal fluticasone spray (200 μg daily) in reducing symptoms and polyp size in chronic sinusitis with allergic rhinitis and to compare pre- and post-treatment secretion of IL-4.
MATERIAL AND METHOD
Adults diagnosed with chronic sinusitis with nasal polyp at St. Paul’s Hospital (College of Medicine, Catholic University of Korea) from March, 2001 to July, 2002 were enrolled in this study.
Selection criteria are as follows:first, all patients should not have any history of either taking any kind of medication which could affect the study 3 weeks prior to visiting the hospital, or otolaryngologic opera- tion. Second, all patients should have visible polyps in the nasal cavity, and third, all patients should have a positive skin prick or RAST test to more than one all- ergen, to confirm diagnosis of allergic rhinitis.
The selected 24 patients were allocated randomly into three groups. The roxythromycin group (Group I) was instructed to take roxythromycin 150 mg b.i.d 30 minutes after meal for 2 months.
The fluticasone propionate group (Group II) was instructed to spray fluticasone propionate 50 μg twice daily to each nostril (total 200 μg) for 2 months. The roxythromycin and fluticasone propionate combined use group (Group III) was instructed to use both roxy- thromycin and fluticasone propionate, as described above.
The patients’ ages ranged from 21 to 55 years (mean age, 39.5 years) and 15 were male and 9 were female.
The mean age of groups I, II and III was 36.8, 41.1 and
40.5 years, respectively. There was no significant di- fference among the groups .
For radiologic evaluation, PNS CT scan grading score by Lund and Mackay was used. Patients with no abnormal or quite minimal specific findings were ex- cluded from the study. The average score was 6.75±
3.32, 6.44±2.97, 6.00±2.09 in groups I, II and III, respectively. No significant difference was found be- tween them (p=0.570). Patients whose PNS CT fin- ding was insignificant (PNS CT grading score:0) were also excluded to eliminate bias.
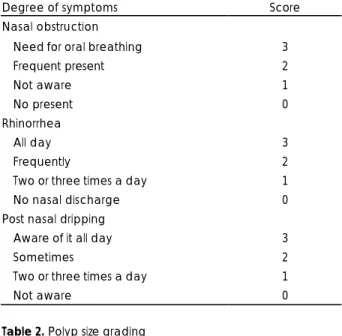
At the first visit, patients were asked to state the severity of their symptoms of rhinorrhea, post nasal dripping and nasal obstruction. Then the severity of their symptoms were assessed by investigators accor- ding to severity criteria graded from 0 to 3 score (Table 1). Visual assessment of nasal polyp size, graded from 1 to 5, was performed by more than 2 investigators (Table 2).
Nasal lavage was done with 5 ml saline. The lavage
Table 1. Criteria for symptoms
Degree of symptoms Score
Nasal obstruction
Need for oral breathing 3
Frequent present 2
Not aware 1
No present 0
Rhinorrhea
All day 3
Frequently 2
Two or three times a day 1
No nasal discharge 0
Post nasal dripping
Aware of it all day 3
Sometimes 2
Two or three times a day 1
Not aware 0
Table 2. Polyp size grading Grade Polyp size
I Located in but not fully occupy middle meatus or olfactory cleft
II Occupy middle meatus fully
III Almost completely obstruct nasal cavity with small airway space at the nasal floor IV Completely obstruct nasal cavity with
visible inferior turbinate V Completely obstruct nasal cavity
without visible inferior turbinate
was then centrifuged at 3000 rpm and stored at -20℃.
The patients were asked to visit at a weekly interval, and were observed to check whether or not they had been taking their medicine regularly as required by the study. Those who failed to comply were excluded from the study.
After a follow up period of 2 months, the patients were asked to record scores for the symptoms of rhin- orrhea, post nasal dripping and nasal obstruction. Saline lavage of the nasal cavity was repeated and polyp size was measured again.
Among patients who followed the scheme strictly for 2 months, 24 patients were selected for the final study, with 8 in each group.
Changes in symptoms and polyp size after treatment were evaluated and analyzed statistically for each group. In the combined use group, IL-4 levels detected by ELISA from saline lavage were quantitatively an- alyzed and compared with those before treatment.
Paired t-test and ANOVA were used for statistical
analysis. A value of p<.05 was considered to be sta- tistically significant.
RESULTS Polyp size
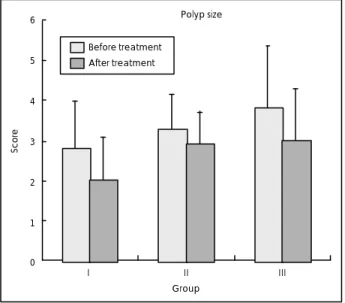
The polyp size score decreased significantly in group I (2.8±1.17 before treatment, 2.0±1.07 after treat- ment on average, p=0.016), and in group II (3.3±0.87 before treatment, 2.9±0.83 after treatment on average, p=0.013). In group III, there was also a statistically significant difference (3.8±1.58 before treatment, 3.0±
1.31 after treatment on average, p=0.011).
No significant difference was found among the groups (p=0.496)(Fig. 1).
Symptoms
Significant improvement was observed for all three symptoms of rhinorrhea, nasal obstruction and post nasal dripping in groups I and II. But in group III, there was no statistically significant difference (p=0.351) just in nasal obstruction although there was a decrease in numerical values. Rhinorrhea and post nasal dripping improved significantly in group III (Table 3).
IL-4
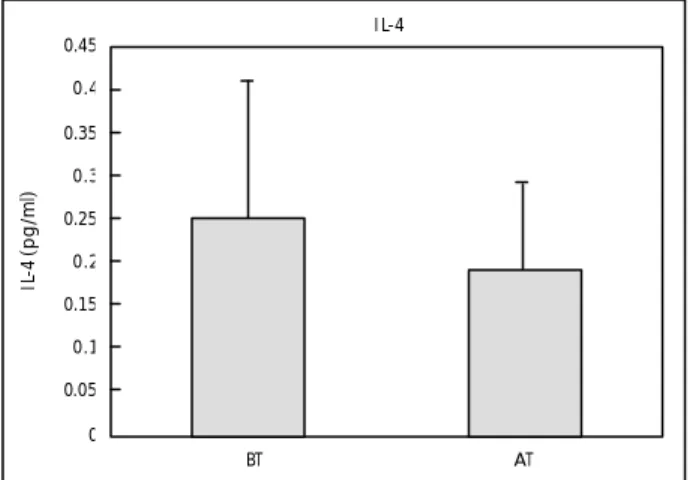
IL-4 in nasal lavage was reduced significantly from 0.25±0.16 pg/ml before treatment to 0.19±0.10 pg/ml after treatment in group III (p=0.000)(Fig. 2).
DISCUSSION
Many hypotheses have been proposed for polyp for- mation. Among them, two theories, epithelium rupture or new gland formation theory presented by Tos and Mogensen and increased ion transport theory proposed by Bernstein et al are worth considering.
Table 3. Comparison of symptoms scores between before and after treatment
Group I Group II Group III
BT AT BT AT BT AT
Rhinorrhea 1.38±1.30 0.25±0.46 0.75±0.70 0.25±0.46 1.63±0.92 0.13±0.35
Nasal obstruction 2.13±0.64 0.63±0.51 1.25±1.28 0.50±0.76 0.25±0.46 0.13±0.35*
PND 2.38±0.74 0.38±0.52 2.63±0.74 1.50±0.53 2.38±0.52 1.63±0.52
PND:postnasal dripping, BT:before treatment, AT:after treatment, *:p>.05 Fig. 1. Comparison of polyp size between before and after
treatment. The polyp size score decreased significantly in groups I (p=0.016), II (p=0.013) and III (p=0.011) statistically. No significant difference was found between the groups (p=
0.496)(I:roxythromycin group, II:fluticasone group, III:com- bined group).
6 5 4 3 2 1 0
Score
Polyp size
I II III Group
Before treatment After treatment
According to the former theory, the first step is infiltration of inflammatory cells and edema, followed by rupture of the epithelium, and then granulation tissue prolapse, followed by new gland formation.
5)The latter theory explains the mechanism of edema formation by increased transepithelial ion transport.
Transepithelial ion transport increases through an increased sodium absorption and increased chloride permeability induced by chemical mediators released from inflammatory cells.
6)In both hypotheses, the role of inflammatory cells is important. The dominant inflammatory cells found in most polyps are lymphocytes, plasma cells, and eosin- ophils.
Eosinophils play an important role in the induction of inflammation and in epithelial damage. Significantly more activated eosinophils are found in the polyp than in the macroscopically unaffected mucosa of the tur- binate.
7)The activated eosinophils cause inflammation by releasiang inflammatory mediators such as major basic protein, eosinophilic cationic protein, as well as leukotrienes and platelet activating factor.
The activating process of eosinophil is regulated by interleukin-5 (IL-5) mainly released from T lympho- cytes,
8)and although far less, from other locally infil- trated inflammatory cells such as mast cells. Some cy- tokines also contribute to this process.
Thus substances that inhibit production and release of IL-5 or other involving cytokines may suppress eosinophil induced tissue damage.
Macrolide is a potent inhibitor of IL-5 production.
Roxithromycin markedly inhibits production of IL-5 in T lymphocytes of allergic rhinitis patients.
9)Neutrophils are also associated with acute inflamm- atory reactions. They release PAF, Leukotriens B
4, and superoxide which may result in tissue damage. They are known to be activated by various cytokines such as IL-8, IL-6, whose production is suppressed by roxi- thromycin.
Transforming growth factor β (TGF-β) may also be a target for macrolides. It has recently been shown that there is a high expression of TGF-β in nasal polyp and in inflammatory nasal mucosa. In yeast cells, ma- crolide blocks the TGF-β receptor, providing a ten- tative mechanism by which the effect of TGF-β may be reduced, which in turn may increase inflammatory cell apoptosis, a key feature in reducing nasal polyp.
10)Intranasal fluticasone significantly decreases eosin- ophil, expression of endothelial P-selectin and a number of IL-4 and IL-13 mRNA-expressing cells. Because IL-4 is an inducer of P-selectin on human endothelial cells,
11)suppression of IL-4 by fluticasone contributes significantly to suppression of P-selectin expression and this reduction of P-selectin in turn contributes to reduced eosinophil influx.
12)VCAM-1 expression on endothelium, which pro- motes accumulation of eosinophils into inflamed tissues, is strongly induced by TNF-α and IL-1β. and this induction is believed to occur by means of an NFκB- dependent mechanism. Because corticosteroids anta- gonize NFκB-induced gene transcription, a direct ph- armacologic effect to suppress endothelial VCAM-1 and resultant eosinophil reduction is possible.
13)14)We got results similar to those of other studies in that roxithromycin and intranasal fluticasone treatment reduces symptoms and polyp size.
Only in the combined group of our study, did nasal obstruction not improve, although there was decrease in numerical values. We presume that result was caused by the fact that the polyp size of the combined group was bigger than that of others.
But contrary to our expectation, the two treatments did not produce any synergic effect or offset result in the combined use group.
In the normal state, the components of the nasal mucosa, such as ciliated columnar cells, germ cells, nonciliated columnar cells and basal cells are under
Fig. 2. Comparison of IL-4 between before and after treatment.
In group III (combined group of roxythromycin and fluticasone propionate), IL-4 was reduced significantly from 0.25±0.16 pg/ml before treatment to 0.19±0.10 pg/ml after treatment on average (p=0.000). BT:befo re treatment, AT:after treat- ment.
I L-4
BT AT 0.45
0.4 0.35 0.3 0.25 0.2 0.15 0.1 0.05 0
IL-4 (pg/ml)
physiologic control. But in allergic rhinitis, this control is lost, resulting in increase of germ cells, mast cells, eosinophils, hypertrophy of glandular cells, decrease of ciliated cells and increased vascular permeability.
IL-4 is a major mediator in this initial inflammatory reaction in allergic rhinitis. In the nasal mucosa of perennial allergic rhinitis, 99-100% of IL-4 conta- ining cells are mast cells. It is known that ready-made and stored IL-4 is released from mast cells at the initial allergic reaction and stimulates the change described above.
3)We could verify the blocking effect of this process by combined use of roxithromycin and intranasal flu- ticasone in this study.
CONCLUSION
Both long term medication of roxithromycin (300 mg daily) and intranasal fluticasone spray (200 μg daily) were effective in reducing symptoms and polyp size in chronic sinusitis with allergic rhinitis. Com- bined use of roxithromycin and fluticasone were also effective in reducing IL-4.
But no significant difference was found between the two treatments, and combined treatment did not show any superiority either.
■
Acknolwedgement
This articles was financially supported by the korean rhinologic society.
REFERENCES
1) Ichimura K, Shimazaki Y, Ishibashi T, Higo R. Effect of new ma-
crolide Roxithromycin upon nasal polyps associated with chronic sinusitis. Auris Nasus Larynx 1996;23:48-56.
2) Svensson C, Klementsson H, Andersson M, Pipkorn U, Alkner U, Persson CG. Glucocorticoid-induced attention of mucosal exudation of fibrinogen and bradykinins in seasonal allergic rhinitis. Allergy 1994;49:177-83.
3) Kim SW, Cho JS, Park JK, Cha JI, Kim KI. Effect of interleukin -4 and histamine on the fibroblast in the nasal mucosa of allergic rhinitis and non-allergic rhinitis. Korean J Otolaryngol 1999;42:
329-35.
4) Kondo H, Nachtigal D, Frenkiel S, Schotman E, Hamid Q. Effect of steroids on nasal inflammatory cells and cytokine profile. Lary- ngoscope 1999;109(1):91-7.
5) Park CH, Na SK, Lim HJ, Jung YG. The effect of steroid and steroid receptor blocker in initial polyp formation. Korean J Otolaryngol 2000;43:1312-7.
6) Bernstein JM, Cropp GA, Nathanson I. Bioelectric properties of cultured nasal polyp and turbinate epithelial cells. Am J Rhinol 1990;4:45-9.
7) Stoop AE, Van der Heijden H, Biewenga J, Van der Baan S. Eosin- ophils in nasal polyps and nasal mucosa: an immunohistochemical study. J Allergy Clin Immunol 1993;91:616-22.
8) Takasu K, Tominaga A. Interleukin -5 and its receptor. Prog Growth Factor Res 1991;3:87-102.
9) Asano K, Kamakazu K, Hisamitsu T, Suzaki H. Modulation of Th2 type cytokine production from human peripheral blood leukocytes by a macrolide antibiotics, Roxithromycin, in vitro. Int Immunoph- armacol 2001. Oct ;1(11):1913-21.
10) Anders Cervin. The anti-inflammatory effect of Erythromycin and its derivatives, with special reference to nasal polyposis and chronic sinusitis. Acta Otolaryngol 2001;121:83-92.
11) Yao L, Pan J, Setiadi H, Patel KD, McEver RP. Interleukin 4 or oncostain M induces a prolonged increase in P-selectin mRNA and protein in human endothelial cells. J Exp Med 1996;184(1);81-92.
12) Rothenberg MW, Owen WF, Silberstein DS, Woods J, Soberman RJ, Austen KF, et al. Eosinophil co-cultured with endothelial cells have increased survival and functional properties. Science 1987;
237:645-7.
13) Gille J, Paxton LL, Lawley TJ, Caughman SW, Swerlick RA.
Retinoic acid inhibits the regulated expression of vascular cell adhesion molecule-1 by cultured dermal microvascular endothelial cells. J Clin Invest 1997;99:492-500.
14) Johnson DR, Douglas I, Jahnke A, Ghosh S, Pober JS. A sustained reduction in IκB-β may contribute to persistent NF-κB activa- tion in human endothelial cells. J Biol Chem 1996;271:16317-22.