J Rhinol 20(1), 2013 www.ksrhino.or.kr
- 65 -
BBilateral Intranasal Supernumerary Teeth
Jinsu Choi MD and Bo Sung Kim, MD
Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine Dongguk University, Gyeongju, Republic of Korea.
ABSTRACT
The presence of an ectopic supernumerary tooth in the nose is an uncommon phenomenon. A supernumerary tooth may be asymptomatic but must be given special attention as it has the potential to cause significant mor- bidity. Bilateral intranasal supernumerary teeth are an extremely rare disease entity. We report the clinical and radiologic findings of bilateral ectopic supernumerary teeth erupted from the nasal floor.
KEY WORDS : Supernumerary Tooth · Nose.
INTRODUCTION
Intranasal supernumerary tooth is a rare clinical entity.
Nasal teeth manifest in different ways depending on site.
Symptoms and signs associated with nasal teeth include facial pain, nasal obstruction, headache, epistaxis, foul- smelling rhinorhea, external nasal deformities, and na- solacrimal obstruction.1) 2) The etiology is not completely understood. However, some factors proposed including obstruction at the time of tooth eruption secondary to crowded dentition, persistent deciduous teeth, dens bone;
a genetic predisposition; developmental disturbances such as a cleft palate, infections, cysts or operations and dis- placement as a result trauma.3) 4)
We report a case of bilateral intranasal supernumer- ary teeth which successfully extracted by endoscopic ap- proach.
CASE
A 37-year-old man presented with a history of long- standing left nasal obstruction and frequent nasal crust.
No previous history of maxillofacial trauma or surgery was given. No cleft palate or congenital abnormality was noted and his general medical history was unremarkable.
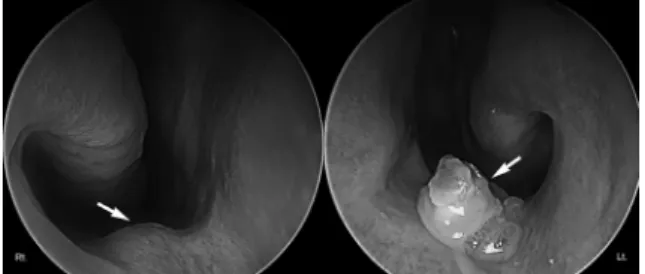
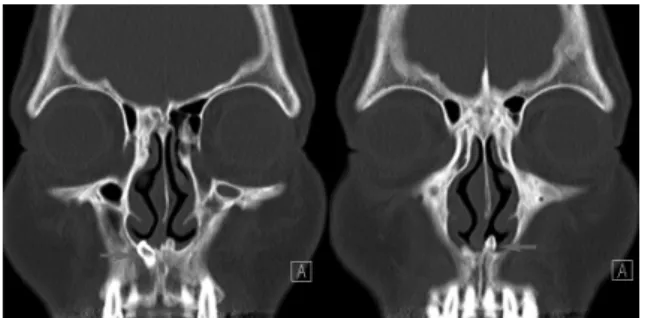
Nasal endoscopic examination revealed a whitish, en- crusted hard mass uncovered by mucosa and surrounded by granulation tissue in the left nasal cavity and anterior nasal floor elevation in the right nasal cavity (Fig. 1, white arrows). The mass was firm and tooth-like appearance, approximately 5 mm in the length and 4 mm in the diam- eter, apparently erupting from the floor of the left nasal cavity. The septum was moderately deviated to the left side. The intraoral examination revealed normal dentition and mucosa. The paranasal sinus computed tomography (CT) scan identified bilateral calcified lesions in both na- sal floors, which were consistent with a dental structure as inverted mesiodens (Fig. 2, red arrows). No cystic or inflammatory changes were noted.
We performed the extraction of the bilateral ectopic teeth under general anesthesia by trans-nasal endoscopic approach. The operative findings suggested that the teeth were erupting from nasal floor. The mucosa membrane covering the teeth, granulation tissue, and debris sur- rounding the teeth were removed. Palatal bone around the
Address correspondence and reprint requests to Jinsu Choi, MD, De- partment of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Dongguk University, 1090-1, Seokjang-dong, Gyeongju-si, Gyeongsangbuk-do, 780-350, Republic of Korea.
Tel: +82-54-770-8261, Fax: +82-54-770-8378 E-mail: [email protected]
Received for publication on November 1, 2012 Accepted for publicatoin on January 2, 2013
Figure 1. Nasal endoscope showed elevated nasal floor mu- cosa in the right nasal cavity and whitish encrusted mass in the left nasal cavity (white arrows).
66 / J Rhinol 20(1), 2013
teeth was removed by chisels until there was sufficient mobility to deliver the teeth. The extracted bilateral na- sal teeth were about 5 mm conical typed mesiodens (Fig.
3). Postoperative bleeding was controlled with Vaseline gauze. The patient did well postoperatively and healed uneventfully.
DISCUSSION
The incidence of supernumerary teeth generally affects 0.1%-1% of the population.3) Most supernumerary teeth are diagnosed in the third decade of life.5)
Supernumerary teeth develop either from a third tooth bed that arises from the dental lamina near the permanent tooth bud or, possibly, from splitting of the permanent bud itself.3) Another theory is that their development is a rever- sion to the dentition of extinct primates, which had three pairs of incisors.3) Although the cause of ectopic growth is not well understood, it has been attributed to obstruction at the time of tooth eruption secondary to crowded dentition, persistent deciduous teeth, or exceptionally dense bone.4 Other proposed pathogenetic factors include a genetic pre- disposition; developmental disturbances, such as a cleft palate, rhinogenic or odontogenic infection, and displace- ment as a result of trauma or cysts.4) The most frequent hypothesis for the aberration of teeth was the existence of an obstacle to the tooth’s eruption, most commonly crowding.6) It is now suggested that a defect in migration of the frontonasal neural crest cells before the end of the fifth embryonic week might cause ectopic development of
tooth germs in the area of the premaxilla.7)
The most common location is the upper incisor area, known as mesiodens. The extra teeth have an atypical crown, and they may be in a vertical, horizontal, or in- verted position.
The teeth may be asymptomatic or cause a variety of signs and symptoms, including facial pain, nasal obstruc- tion, headache, epistaxis, foul-smelling rhinorhea, exter- nal nasal deformities, and nasolacrimal obstruction.1) 2) Complications of nasal teeth include rhinitis caseosa with septal perforation, aspergillosis, and naso-oral fistula.8) 9)
The diagnosis of nasal teeth is made on the basis of clinical and radiographic findings. Clinically, an intrana- sal tooth may be seen as a white mass in the nasal cav- ity surrounded by granulation tissue and debris.1) Radio- graphically, the nasal teeth appeared as radiopaque lesions with the same attenuations that of the oral teeth. With the bone window setting, the central radiolucency, which is correlated with the pulp cavity, may have a spot or split, depending on the orientation of the teeth.8)
The differential diagnosis of nasal teeth includes ra- diopaque foregn body; rhinolith; inflammatory lesions due to syphilis, tuberculosis, or fungal infection with calcifi- cation; benign tumors, including hemangioma, osteoma, calcified polyps, enchondroma, and dermoid; and malig- nant tumors, such as chondrosarcoma and osteosarcoma.8) However, the CT findings of tooth-equivalent attenuation and a centrally located cavity are highly discriminating features that help to confirm the diagnosis.8)
When an extra tooth is in the nasal cavity, the proce- dure is usually a minor operation. When a tooth has a bony socket in the floor of the nose, it may be extremely dif- ficult to extract.10) Early extraction of nasal tooth is gen- erally advocated to alleviate the symptoms and prevent complications because supernumerary tooth can cause considerable morbidity.6)
저자역할(Author Contributions)
최진수, 김보성은 본 연구에서 모든 자료에 접근할 수 있으며, 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습니다. 연구 기획 : 최 진수, 김보성. 자료 해석 및 분석 : 최진수, 김보성. 논문 초안 : 최진 수, 김보성. 연구 총괄 :최진수
REFERENCES
1) Smith RA, Gordon NC, De Luchi SF. Intranasal teeth: report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol 1979;47:120-2.
2) Alexandrakis G, Hubbell RN, Aitken PA. Nasolacrimal duct ob- struction secondary to ectopic teeth. Ophthalmol 2000;107:189- 3) Thawley SE, Ferriere KA. Supernumerary nasal tooth. Laryngo-92.
scope 1977;87:1770-3.
Figure 2. Coronal computed tomography of the paranasal si- nuses revealed bilateral nasal supernumerary teeth erupted from nasal floor (red arrows).
Figure 3. Extracted bilateral supernumerary teeth specimens.
4) Moreano EH, Zich DK, Goree JC, et al. Nasal tooth. Am J Otolar- yngol 1998;19:124-6.
5) Kirmeier R, Truschnegg A, Payer M, Malyk J, Daghighi S, Jakse N. The supernumerary nasal tooth. Int J Oral Maxillofac Surg 2009;38:1219-22.
6) Solokov M, Jecker P, Roth Y. Nasal teeth associated with rhinosi- nusitis. Rhinology 2004;42:167-70.
7) Kuroda H, Tsutsumi K, Tomisawa H, Koizuka I. A case of an invert- ed tooth in the nasal cavity. Auris Nasus Larynx 2003;30:s127-9.
8) Chen A, Huang JK, Cheng SJ, Sheu CY. Nasal teeth: report of three cases. Am J Neuroradiol 2002;23:671-3.
9) El-Sayed Y. Sinonasal teeth. J otolaryngol 1995;24:180-3.
10) Wurtele P, Dufour G. Radiology case of the month; a tooth in the nose. J Otolaryngol 1994;23:67-8.
Choi et al : Bilateral nasal teeth / 67