대 한 소 아 신 경 학 회 지
Vol. 15, No. 2, November, 2007
□ 원 저 □1)
서 론
모야모야병은 비교적 드문 폐쇄성 혈관질환으로 소아에서 허혈성 증상을 초래하는 질환이다. 1969 년 일본의 Suzuki와 Takaku1)에 의해 뇌혈관 촬영 상 공기중에 담배연기가 퍼지는 모양과 비슷하여 moyamoya로 명명되었으며 내경동맥이나 그 말단 부에서 협착 또는 폐쇄가 진행되며 뇌기저부에서 망상형의 이상 미세 혈관총을 형성하는 아직 그 원 인이 밝혀지지 않은 질환이다2). 일본과 한국에서
책임저자 : 황태규, 인제의대 부산백병원 소아청소년과 Tel : 051)890-6290, Fax : 051)895-7785 E-mail : [email protected]
많이 발생하며3-5) 여아에서 더 많이 발생하고 어느 연령에서나 증상이 나타날 수 있지만, 연령분포 양 상을 보면 10세 미만과 30대에 2개 정점을 나타낸 다3).
국내에서도 1970년대 이후 많은 보고들이 있어 왔으나 소아 청소년 모야모야병의 발병양상이나 신 경학적 예후 등에 대해서는 아직 명확히 알려져 있 지 않다. 이에 저자들은 인제대학교 의과대학 부산 백병원에 내원하여 자기공명혈관조영술 및 혈관촬 영을 통해 모야모야병으로 진단받은 소아청소년 36 명을 대상으로 연령, 성별 분포, 임상양상 및 방사 선학적 소견들을 조사 분석 하였다.
소아 청소년 모야모야병 환자의 임상양상에 대한 연구
이승익·지근하·황태규
인제의대 부산백병원 소아청소년과
= Abstr act =
Moyamoya Disease in Children and Adolescents
Seung Ik Lee, M.D., Geun Ha Chi, M.D. and Tae Gyu Hwang, M.D.
Department of Pediatrics, School of Medicine, Inje University, Busan, Korea
Purpose : Moyamoya disease is a chronic cerebrovascular illness characterized by bi- lateral stenoses or occlusions of the arteries around the circle of Willis with prominent collateral circulation. We studied 36 children and adolescents with Moyamoya disease to evaluate the clinical features and outcomes.Methods : Records were reviewed of 36 pediatric patients admitted at the Busan Paik Hospital for Moyamoya disease between January 2000 and July 2007. The clinical records were reviewed in terms of the patient profiles, imaging findings, surgical techniques, and pathologic findings.
Results : Overall clinical features, responses to treatment and outcome were nearly same as those of other previous reports in Korea as well as the other countries. The mean age of onset was 8 years and 5 months and the ratio of male to female was 1:1.2. Is- chemia was more often than infarction(5.6: 1). Half of the patients had conservative the- rapy and 17 cases(47%) were treated with EDAS.
Conclusion : The clinical features of childhood Moyamoya disease are similar to the result from other studies in Korea.
Key Words : Childhood Moyamoya disease, Clinical features
대상 및 방법
2000년 1월 부터 2007년 7월까지 인제대학교 부 산 백병원에 내원하여 뇌자기공명영상, 뇌자기공명 혈관 조영술, 경동맥 조영술 상에서 모야모야병으로 진단받은 20세 이하의 소아 청소년 36명을 대상으 로 연령, 성별, 발병빈도, 발생시기, 임상증상, 방사 선 소견과 신경학적 휴유증, 추적관찰시 예후를 후 향적으로 비교 분석 하였다. 모든 환아들에서 뇌혈 관 조영술이 시행되었고 이 소견에 따라 definite (bilateral)과 probable(unilateral)로 구분하였다 (Table 1).
결 과
1. 연령적 분포
남자는 17명, 여자는 19명으로 성비는 1:1.12로 여자가 더 많았다. 증상발생의 연령분포는 2세 3개 월에서 16세 7개월 사이로 평균 8세 5개월이었고 6세에서 10세 사이에서 가장 많이 발생하였다(Table 2).
2. 임상양상
첫 임상양상으로는 반신마비 증상이 25례(69%) 로 가장 많았으며 그 외에 두통 5례(14%), 경련 3 례(8%), 의식소실 2례(6%), 경련과 반신마비가 동 반된 경우가 1례(3%)였다(Table 3).
허혈성이 28명(78%)으로 출혈성 5명(14%) 보다 많았으며 연령이 증가할수록 출혈성의 비율이 좀
더 많았다. 허혈성에서 일과성 허혈 발작은 15명, 뇌경색은 13명이었다. 5명의 출혈성에서는 뇌내 출 혈(4명)이 일차성 뇌실내 출혈(1명) 보다 더 많이 발생하였다. 이중 3명(8%)은 안면 경련을 주소로 내원하여 우연히 진단된 예였다(Table 4).
호발한 시기는 4월이 8례(22%)로 가장 많았고 9 월에는 한 례도 없었다(Table 5).
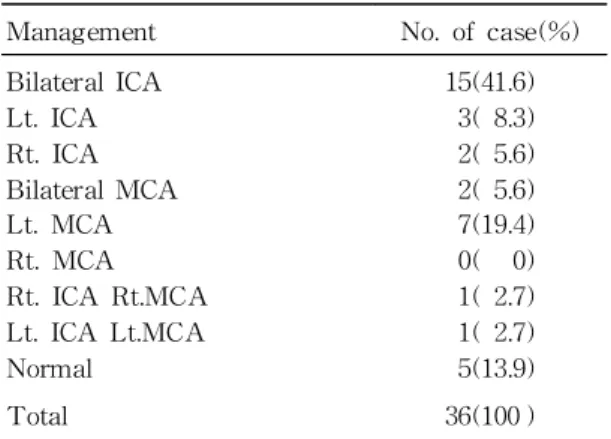
3. 혈관폐쇄부위
반대편의 병변이 전혀없는 일측성(Table 1의 Cri- teria 3를 만족하지 않는 경우)이 16명, 양측성이 20명이었다. 일측성 16명중 남자가 6명, 여자는10명 으로 여자가 1.7배 더 많았고, 평균연령은 8.33세로 양측성 3.6세에 비해 늦게 발생하였다(Table 6).
Table 1. Angiographic Findings for the Diagnosis of Moyamoya Disease36)
Stenosis or occlusion is observed at the terminal portionof the intracranial ICA and/or at the proxismal portion of the ACA and/or the MCA.
Abnormal vascular moyamoya networks are observed in the vicinity of the above-mentioned area in the arterial phase
These findings are recognized bilaterally
Abbreviations : ICA, internal carotid artery; ACA, Anterior cerebral artery; MCA, Middle cerebral artery Note : definite case, fulfills all the above findings; probable case, does not fulfill the criteria 3
Table 2. Age and Sex of Moyamoya Disease
Age No. of Patients
Male Female Total -5 years
6-10 years 11-15 years 16-20 years Total
6 4 6 1 17
1 15 2 1 19
7 19 8 2 36
Table 3. Clinical Features on Admission Clinical Feature No. of Cases(%) Hemipharesis
Conversion
Hemiparesis+Conversion Headache
Loss of consciousness Total
25(69.4) 3( 8.3) 1( 2.8) 5(13.9) 2( 5.6) 36(100 )
4. 치 료
치료로는 보존적 요법이 18례(50%)였고, Encep- halo-duro-arterio-synangiosis는 17례(47%), 혈 종 제거술은 1례(2%)였다(Table 7).
5. 추적관찰
총 36명의 환아중 18례(50%)에서 임상적으로 신 경학적 휴유증이 없었다. 재발이 총 4례(11%)에서 있었으며 사망한 환아는 1례(1%)가 있었다. 퇴원 후 환자들의 상태를 보면 총 36명의 환아 중 25명 의 환아에서 외래 추적결과를 확인할 수 있었으며,
평균 관찰기간은 4년 3개월이었다. 이중 14례에서 합병증을 보였으며 그 종류로는 편측마비 10례, 두 통 3례, 정신지체 2례 순이었으며 아무런 합병증 없 이 지내는 환아도 11례 있었다.
고 찰
1956년 Kudo2)가 처음으로 일반적인 두뇌 혈관 양상과는 다른 미만성 두개강내 혈관 연결 양상을 처음 보고하였다. 모야모야란 경동맥 조영술상, 조 영제가 이상 뇌혈관으로 채워가는 모습이 마치 연 기가 공기중으로 뿜어져 나가는 듯한 모양을 지칭 하는 말로써 1969년 Suzki와 Takaku1)가 최초로 이 병을 이렇게 명명하였다. 성인에서는 주로 기저 핵 부위에 호발하는 뇌출혈 또는 뇌 지주막하 출혈, 뇌실내 출혈로 관찰되지만 가끔씩 반복되는 일시적 허혈증, 감각이상, 시각장애와 같은 대뇌 허혈증이 나 불수의적인 움직임, 경련, 편두통과 같은 증상으 Table 4. Initial Manifestations of Moyamoya Dis-
ease
Features Number(%)
Ischemic TIA Infarction Hemorrage
ICH
ICH with IVH Incidental(facial spasm) Total
28(77.8) 15(41.7) 13(36.1) 5(13.9) 4(11.1) 1( 2.8) 3( 8.3) 36(100 ) Abbreviations : TIA, transient ischemic attack; ICH, intracerebral hemorrhage; IVH, intraventricular he- morrage
Table 6. Site of Occlusion
Management No. of case(%)
Bilateral ICA Lt. ICA Rt. ICA Bilateral MCA Lt. MCA Rt. MCA Rt. ICA Rt.MCA Lt. ICA Lt.MCA Normal
Total
15(41.6) 3( 8.3) 2( 5.6) 2( 5.6) 7(19.4) 0( 0) 1( 2.7) 1( 2.7) 5(13.9) 36(100 ) Abbreviations : ICA, internal carotid artery; ACA, anterior cerebral artery; MCA, middle cerebral artery; PCA, posterior cereblral artery
Table 7. Type of Management
Management No. of Cases(%)
Encephloduroarteriosynangiosis Conservative
Hematoma evacuation Total
17(47.2) 18(50 ) 1( 2.8) 36(100 ) Table 5. Month of Onset
Month No. of cases(%)
January February March April May June July August September October November December Total
5(13.9) 3( 8.3) 5(13.9) 8(22.2) 2( 5.6) 2( 5.6) 2( 5.6) 5(13.9) 0( 0) 1( 2.7) 1( 2.7) 2( 5.6) 36(100 )
로 나타난다6, 7). 소아에 있어 치료받지 않은 모야모 야병의 자연경과는 좋지 않았고 73% 정도의 비율 로 주 신경학적 결손 또는 사망으로 이어진다8).
원인은 아직 불분명하나 모야모야 혈관들이 뇌혈 관들의 선천적인 형성장애로 생긴다는 가설과 자가 면역학적 질환이나 혈액응고질환, 동맥 경화성 질 환, 혈관의 감염성 질환과 같은 후천적인 원인으로 양측성 내경동맥의 분지부위에서 점차적인 폐색이 진행됨에 따라 만성적으로 뇌허혈상태에 빠져 측부 순환으로 모야모야 혈관이 발생한다는 가설이 있다
9-11)
. 최근 연구에 의하면 가족력이 있는 경우가 약 10% 정도에서 보고되고 있으며12, 13), 이는 염색체 3p24.2-2614), 염색체 17q2515)과 연관되어 있는 것 으로 나타나 있다. 그 외에 섬유모세포 성장인자 (fibroblast growth factor)가 뇌척수액, 혈관 중간 층, 평활근에서 발견되며16, 17). 혈액속의 전환성장인 자 베타-1(transforming growth factor beta-1)18,
19) 및 뇌척수액과 경동맥 기시부위에서의 간세포 성장인자(hepatocyte growth factor)의 높은 농도
20) 역시 모야모야병의 원인인 혈관 협착 및 신생혈 관형성과 관련이 있는 것으로 보고되고 있다.
Suzuki와 Kodama3) 등은 주 호발나이로 10세 이하 소아 그리고 30대 성인이라 기술하였으며, 남 녀 성별비는 Nishimoto 등21)에서 남:녀=1:1.65였으 며 본 연구에서는 1:1.2 였다. 본 연구의 결과에 따 르면 주로 봄에 많이 발생하였으나 모야모야병에 있어서 계절적 변동, 특정시기에 호발하는 유발요인 은 아직 연구된 바 없다.
임상증상은 크게 뇌허혈로 인한 증상과 뇌출혈로 인한증상 그리고 그 외의 증상으로 나눌 수 있다.
Maki와 Enomoto22)는 경색이 주로 남자 그리고 출 혈은 여자에서 호발한다고 제안하였으나, 본 연구에 서는 남아에서는 출혈과 경색의 비율이 1:1.33이었 고 여아에서는 1:4.5였고 전체 5례의 출혈 환아 중 2례가 여아였다. 이는 환아군을 소아 청소년에 한정 했으며 이시기에는 출혈보다는 경색이 더 많이 나 타나기 때문으로 생각된다. 반복되는 일과성 허혈 발작, 뇌허혈로 인한 증상인 경련, 반신마비, 일시적 신경학적이상 등이 질병의 최초 임상증상이다23). 본
연구에서는 허혈성에서 일과성 허혈 발작은 15명, 뇌경색은 13명이었으며, 뇌내 출혈이 일차성 뇌실 내 출혈보다 더 많이 발생하였고 연령이 증가할수 록 출혈성의 비율이 좀 더 많았다.
모야모야병의 치료는 내과적, 외과적 치료 모두 가능하며 내과적 치료는 급성기 상태에서는 도움을 줄 수 있으나 스테로이드, 항혈소판제제 등을 사용 한 보고에 따르면 재발이나 뇌혈관조영술상의 병의 진행을 변화시키지는 못한다고 하였다24). 재혈관화 수술치료의 일차목적은 인위적으로 측부 순환을 형 성시켜 모야모야 혈관의 혈역학적 부하(hemodyna- mic stress)를 줄이고 모야모야 혈관들의 발생을 저지시키는 데 있다25, 26). 수술방법으로는 크게 두 가지로 대별된다. 첫째 천측두동맥-중뇌동맥 문합 등의 직접재혈관화 방법으로 문합의 성공률이 높고 즉각적으로 측부 순환을 발생시키는 장점이 있다.
둘째 EDAS와 같은 간접재혈관화 방법으로 수술 수기가 비교적 간단하고 피질동맥 혈류의 일시적 차단이 필요 없어서 안전한 것이 장점이다27). 소아 는 진단 후 빨리 수술을 시행할수록 신경학적 결손 을 줄일 수 있으나27), 만약 양성의 경과를 보인다면 보존적 치료만 시행하기도 한다. 대부분의 소아의 허혈성 증상과 일부 성인의 허혈성 증상에 재혈관 화 수술이 효과가 있다고 알려져 있다9, 28-34).
질환의 예후는 비교적 양호한 것으로 알려져 있 으며 예후 결정인자는 모야모야병의 후유증 정도 출혈이나 경색부위에 따라 달라지는 것으로 알려져 있다22, 35).
본 연구는 이전의 연구들과 비교하여 유사한 결 론을 얻을 수 있었으나 계절적 호발성 및 여아에서 출혈성 모야모야병이 높게 나온 결과 등이 이전의 결과와는 차이를 보였다. 소아 청소년기에 한정하였 지만 나이가 많을수록 출혈성향이 높아지는 것을 확인할 수 있었다. 영상 진단기법의 발달로 모야모 야병의 진단은 보다 용이해 졌으나 임상경과 및 예후 그리고 치료법에 있어서는 예전의 연구결과와 크게 다르지 않았다.
요 약
목 적 : 모야모야병은 소아청소년기에 심각한 후 유증을 남기는 뇌혈관 질환이다. 본 연구에서는 모 야모야병을 가진 소아청소년 환아의 임상양상 및 치료경과에 대한 고찰을 하고자 하였다.
방 법 : 2000년 1월부터 2007년 7월까지 인제의 대 부산 백병원에서 모야모야병으로 진단받은 환자 를 대상으로 발병당시 증상, 연령별, 성별 발병빈도, 발생시기, 임상증상, 방사선 소견과 신경학적 휴유 증, 추적관찰 시 예후를 후향적으로 비교 분석 하였 다.
결 과 : 남자는 17명, 여자는 19명으로 성비는 1:
1.2로 여자가 더 많았고, 증상발생의 연령분포는 2 세 3개월에서 16세 7개월 사이로 평균 8세 5개월 이었다. 첫 임상양상은 허혈성이 28명으로 출혈성 5명 보다 많았으며 연령이 증가할수록 출혈성의 비 율이 좀 더 많았다. 허혈성에서 일과성 허혈 발작은 15명, 뇌경색은 13명이었다. 18례에서 임상적으로 신경학적 휴유증이 없었고 재발이 총 4례, 사망한 환아는 1례였다.
결 론 : 영상 진단기법의 발달로 모야모야병의 진 단은 보다 용이해졌으나 그 임상경과 및 예후는 크게 변하지 않았다.
References
1) Suzuki J, Takaku A. Cerebrovascular Moya- moya disease. Archs Neurol 1969;20:288-99.
2) Kudo T. Spontaneous occlusion of the circle of Willis : A disease apparently confined to Japanase. Neurol 1968;18:485-96.
3) Suzuki J, Kodama N. Moyamoya disease: a review. Stroke 1983;14:104-9.
4) Goto Y, Yonekawa Y. Worldwide distribution of Moyamoya disease. Neurol Med Chir 1992;
32:883-6.
5) Ikezaki K, Han DH, Kawano T, Inamura T, Fukui M. Epidemiological survey of Moyamoya disease in Korea. Clin Neurol Neurosurg 1997;
99(2 suppl):6S-10S.
6) Yonekawa Y, Ogata N, Kaku Y. Moyamoya disease in Europe, past and present status.
Clin Neurol Neurosurg 1997;99(2 Suppl):58-60.
7) Chiu D, Shedden P, Bratina P. Clinical features of moyamoya disease in United States. Stroke 1998;29:1347-51.
8) Olds MV, Griebel RW, Hoffman HI, Craven M, Chuang S, Schutz H. The surgical treatment of childhood moyamoya disease. J Neurosurg 1987;66:675-80.
9) Mabuchi A, Tanabe H, Fujigawa Y, Fujimoto K, Nakata K. An autopsy case of the abnor- mal network of the intracranial artery con- genital dysplasia of the cerebral artery. Brain
& Nerve 1973;25:1759-68.
10) Leeds NE, Abbott KH. Collateral circulation in cerebrovascular disease in childhood via rete mirabile and perforating branches of anterior choroidal and posterior cerebral arteries. Radiol 1965;85:628-34.
11) Nishimoto A, Takeuchi S. Hemangiomatous malformation of bilateral international carotid artery at the base of brain. Brain Nerve 1965;
17:750-61.
12) Kitahara T, Ariga N, Yamaura Q, Makino H, Mak Y. Familial occurrence of moyamoya disease: report of three Japanese families. J Neurol Neurosurg Psych 1979;42:208-14.
13) Houkin K, Abe H, Yoshimoto T, Takahashi A. Is "unilateral" moyamoya disease different from moyamoya disease? J Neurosurg 1996;85:
772-6.
14) Ikeda H, Sasaki T, Yoshimoto T, Fukui M, Arinami T. Mapping of a familial moyamoya disease gene to chromosome 3p24.2-p26. Am J Hum Genet 1999;64:533-7.
15) Yamauchi T, Tada M, Houkin K, Tanaka T, Nakamura Y, Kuroda S et al. Linkage of fa- milial moyamoya disease(spontaneous occlusion of the circle of Wilis) to chromosome 17q25.
Stroke 2000;31;930-5.
16) Inoue TK, Ikezaki K, Sasazuki T, Matsushima T, Fukui M. Analysis of class II genes of human leukocyte antigen in patients with mo- yamoya disease. Clin Neurol Neurosurg 1997;
99(2 Suppl):234S-7S.
17) Malek AM, Connors S, Robertson RL, Folkman J, Scott RM. Elevation of cerebrospinal fluid
level of basic fibroblast growth factor in mo- yamoya and central nervous system disorder.
Pediatr Neurosurg 1997;27:182-9.
18) Yamamoto M, Aoyagi M, Tajima S, Wachi H, Fukai N, Matsushima Y et al. Increase in elastin gene expression and protein synthesis in arterial smooth muscle deverived from pa- tients with moyamoya disease. Stroke 1997;28:
1733-8.
19) Hojo M, Hoshimaru M, Miyamoto S, Taki W, Nagata I, Asashi M et al. Role of transforming growth factor-beta 1 in the pathogenesis of moyamoya disease. J Neurosurg 1998;89:623-9.
20) Nanba R, Kuroda S, Ishikawa T, Houkin K, Iwasaki Y. Increased expression of hepatocyte growth factor in cerebrospinal fluid and intra- cranial artery in moyamoya disease. Stroke 2004;35:2837-42.
21) Nishimoto A, Suzuki K, Homma A, Mirota T.
Moyamoya disease in children(in japanese with English abstract) Nerv Syst Child 1984;9:189- 97.
22) Maki Y, Enamoto T. Moyamoya disease. Childs Nerv Syst 1988;4:204-12.
23) Fujiwara J, Nakahara S, Enomoto T, Nakata Y, Takita H. The effectiveness of O2 admini- stration for transient ischemic attacks in Mo- yamoya disease in children. Childs Nerv Syst 1996:12:69-75.
24) Robertson RL, Burrows PE, Barnes PD, Robson CD, Poussaint TY. Scott RM. Angiographic changes after pial synangiosis in childhood Moyamoya disease. Am J Neuroradiol 1997;18:
837-45.
25) Ueki K, Meyer F, Mellinger JF. Moyamoya disease: the disorder and surgical treatment.
Mayo Clin Proc 1994;69:749-57.
26) Aoki N, Nagawa M. Management of adult Moyamoya disease. Neurol Med Chir 1993;33:
300-5.
27) Kim EY, Kim DS, Choi JU, Chung SS, Lee KC. Surgical treatment of Moyamoya disease by indirect revascularization procedure. J Neu- rosurg Soc 1996;25:69-80.
28) Kuwabara Y, Ichiya Y, Otsuka M, Tahara T, Gunasekera R, Hasno K, et al. Cerebral hemo- dynamic change in the child and adult with Moyamoya disease. Stroke 1990;21:272-7.
29) Tagawa T, Naritomi H, Mimaki T, Yabuuchi H, Sawada T. Regional cerebral blood flow, clinical manifestations, and age in children with moyamoya disease. Stroke 1987;18:906-10.
30) Watanabe H, Ohta S, Oka Y, Kumon Y, Sakaki S, Sugawara Y, et al. Changes in cortical CBF and vascular response after vascular recon- struction in patients with adult onset Moya- moya disease. Acta Neurochir(Wien) 1996;148:
1211-7.
31) Kinugasa K, Mandai S, Kamata I, Sugin K, Ohmoto T. Surgical treatment of moyamoya diseases: operative technique for encephalo- duro-arterio-myo-synangiosis, its follow-up, clinical results, and angiograms. Neurosurg 1993;32:527-31.
32) Ishikawa T, Houkin K, Kamiyama H, Abe H.
Effects of surgical revascularization on out- come of patients with pediatric Moyamoya disease. Stroke 1997;28:1170-3.
33) Kohno K, Oka Y, Kohno S, Ohta S, Kumon Y, Sakaki S. Cerebral blood flow measurement as an indicator for an indirect revascularization procedure for adult patients with Moyamoya disease. Neurosurg 1998;42:752-8.
34) Kobayashi H, Hayashi M, Handa Y, Kubota M, Noguchi Y, Aradachi H. EC-IC bypass for adult patients with Moyamoya disease.
Neurol Res 1991;13:113-6.
35) Karasawa J, Kikuchi H, Furuse S, Sakai T, Onishi H, Taki W. A surgical treatment of moyamoya disease: Encephalomyosynangiosis.
Neurol Med Chir 1977;17:29-37.
36) Yonekawa Y, Goto Y, Ogata N. Moyamoya disease: diagnosis, treatment and recent achi- evement. In: Barnett HJM, Mohr JP, Stein BM, Yatsu FM, eds. Stroke: Pathophysiology, Diagnosis, and Management. 2nd ed. New York: Churchill Livingstone 1992:721-47.