서 론
청력의 저하는 대화를 통한 의사소통을 어렵게 하고, 이에 따라 행동장애 및 사회심리적 장애 등을 초래할 수 있기 때문에 심각한 문제가 될 수 있다.1) 청력의 저하는 30대부터 시작되나, 40–60세에는 1 kHz 부근의 회화 영역에 청력 저하가 발생하고, 60대 이후 질병, 외 상, 퇴행성 변화 등의 요인에 의하여 저주파 영역도 떨어지게 된다.2) 2009년 국민건강통계 보고에 따르면 0.5, 1, 2, 3 kHz의 순음청력평균
치 40 dB을 기준으로 할 때 만 12세 이상에서 일측성 난청 유병률은 5.7% (남자 5.1%, 여자 6.2%)였고, 양측성 난청 유병률은 4.5% (남자 4.4%, 여자 4.5%)였다. 난청 유병률은 50대 이후 연령이 10세 높아짐에 따라 증가하여 일측성은 50대 6.9%, 60대 14.7%, 70대 이상 17.8%였고, 양측성은 50대 2.9%, 60대 12.1%, 70대 이상 31.7%였다.3)
청력 저하에 영향을 미치는 요인으로는 연령, 소음, 흡연, 약물 등 이 있으며, 이외에도 고혈당, 고혈압 등 심혈관 질환의 위험요인도 영 향을 주었다.4-9) 하지만 이상지질혈증과 청력의 관련성은 이전의 연
Original Article
한국 성인 남녀에서 이상지질혈증 유병 및 치료 여부에 따른 평균 청력의 차이: 제5기 국민건강영양조사 2010-2012년 자료 이용
김동휘, 박선기*, 김경민, 신성군
동의병원 가정의학과
Association between Hearing Loss and Dyslipidemia Prevalence and Treatment in Adults in Korea:
The Fifth Korean National Health and Nutrition Examination Survey in 2010–2012
Dong-Hui Kim, Seon-Ki Park*, Kyung-Min Kim, Seong-Gun Shin
Department of Family Medicine, Dong-Eui Medical Center, Busan, KoreaBackground: Several studies have indicated that dyslipidemia affects hearing; however, the results are not consistent. Here, we investigated average hearing, as well as the association between hearing loss and dyslipidemia prevalence and treatment.
Methods: We analyzed the data for 4,148 individuals aged 30–49 years from the fifth Korean National Health and Nutrition Examination Survey (2010–
2012). Dyslipidemia prevalence and treatment were defined using a questionnaire and blood test results. An average hearing threshold of 0.5, 1, or 2 kHz was used to define low-frequency pure tone average, while high-frequency pure tone average was defined as average hearing thresholds of 3, 4, or 6 kHz in the more impaired ear. Hearing loss was defined as pure tone averages ≥26 dB.
Results: There was no significant difference in low-frequency and high-frequency pure tone averages between the dyslipidemia and control groups and between the dyslipidemia treatment and non-treatment groups. Dyslipidemia prevalence and treatment were not associated with hearing loss after adjusting for age, sex, body mass index, blood pressure, fasting glucose, glycated hemoglobin, total cholesterol, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, alcohol use, smoking, history of noise exposure, hypertension, diabetes, and coronary disease.
Conclusion: Dyslipidemia prevalence and treatment in men and women aged 30–49 years was not associated with hearing loss.
Keywords: Dyslipidemia; Middle Aged; Hearing; Audiometry
http://dx.doi.org/10.21215/kjfp.2016.6.4.235 eISSN 2233-9116
Korean J Fam Pract. 2016;6(4):235-241
KJFP
Korean Journal of Family PracticeReceived February 17, 2016 Revised April 22, 2016 Accepted May 5, 2016 Corresponding author Seon-Ki Park
Tel: +82-51-850-8763, Fax: +82-51-850-8965 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dong-Hui Kim, et al. Association between Hearing Loss and Dyslipidemia Prevalence and Treatment
Korean Journal of Family Practice
KJFP
구들에서 결과가 다양하게 나타났다. Axelsson과 Lindgren10)은 고콜 레스테롤혈증으로 인해 청력 저하가 일어난다고 하였으나, 반면 Sousa 등5)과Anbari 등11)은 청력 저하와 연관이 없었다고 보고하였 다. 또한 이상지질혈증의 약물 치료가 청력에 어떤 영향을 주는지에 대한 연구도 있었는데, statin이 청력에 영향이 없다는 결과도 있었으 며,12) Liu 등13)에 의한 연구에서는 오히려 약물의 부작용으로 청력이 저하된다는 결과도 있었다.
2009–2011년 국민건강영양조사를 이용한 Lee 등14)의 최근 국내 연 구에서는 이상지질혈증이 있는 군에서 없는 군보다 청력이 더 좋다 는 보고가 있었는데, 설문으로 이상지질혈증의 유병 여부만을 조사 하여 나온 결과이기 때문에 이상지질혈증에 대한 치료 여부와 진단 받지 않은 이상지질혈증에 대한 분석이 부족했다. 이에 본 연구에서 는 30–49세 남녀를 대상으로 이상지질혈증 유병 및 치료 여부에 따 른 평균 청력의 차이와 난청의 빈도, 연관성을 알아보고자 한다.
방 법
1. 연구대상
제5기 1–3차년도(2010–2012년) 국민건강영양조사 대상자 중에서 지질검사, 청력검사 및 설문조사를 시행한 30–49세 성인 남녀 7,140 명 중, 중이염이 있거나 치료 중인 경우, 보청기 및 인공와우를 사용 중인 경우, 이과시진에서 외이 이상이 있는 경우, 이과 0도 내시경에 서 외이도 협착이나 고막 이상이 있는 경우를 제외하였고, 항목별로 결측값과 무응답을 제외하여 최종적으로 총 4,148명(남자 1,776명, 여자 2,372명)을 본 연구대상에 포함하였다.
국민건강영양조사는 시도별, 동읍면, 성별, 연령대별, 주거유형 등 으로 층화한 후 표본조사구를 설정하여 계통추출방법으로 조사구 당 20개의 조사대상가구를 추출하여 매년 192개 표본조사구에서 전국 3,840가구의 만 1세 이상 가구원 전체 약 1만 명을 대상으로 1 월–12월까지 실시하였다.
2. 연구방법
대상자의 고혈압, 당뇨, 이상지질혈증의 유병 여부 및 치료 여부, 귀 질환 등의 병력, 소음노출 여부, 음주, 흡연 등을 포함한 생활습관 등은 설문지를 통해 조사하였다. 흡연은 평생흡연 여부를 기준으로 흡연하지 않았거나 5갑(100개비) 미만인 경우는 비흡연군(none), 5갑 이상 흡연하였으나 현재는 금연하는 경우는 금연군(past), 흡연량과 관계없이 현재 흡연하는 경우는 흡연군(current)으로 분류하였다. 음 주는 1년간 음주 빈도를 기준으로 주 2회 이상이면 위험음주군(haz- ardous), 주 2회 미만이면 건강음주군(moderate)으로 분류하였다.
소음노출 여부는 설문을 통해 버스나 지하철 등 시끄러운 장소에 서 이어폰을 사용하여 크게 음악을 들은 적이 있는지, 기계음 등 소 음이 큰 장소에서 3개월 이상 근무한 적이 있는지, 직업적 노출 외에 한 주에 5시간 이상 큰 소음에 노출된 적이 있는지, 총소리나 폭발음 등 순간적 큰 소음에 노출된 적이 있는지에 따라 분류하였다.
혈압은 질병관리본부 전문조사 수행팀 내 혈압측정 담당 간호사 4명이 측정하였으며, 4 cm 높이의 팔받침대를 여러 개 사용하여 대 상자별 팔높이를 심장높이에 맞추어 상완에서 3차례 혈압 측정 후 2, 3차 혈압 평균치를 사용하였다.
채혈은 공복상태에서 이루어졌고, 공복혈당, 총콜레스테롤(total cholesterol, TC), 고지단백 콜레스테롤(high density lipoprotein choles- terol, HDL-C), 저지단백 콜레스테롤(how density lipoprotein choles- terol, LDL-C), 중성지방(triglyceride, TG)은 Hitachi Automatic Analyz- er 7600 (Hitachi, Tokyo, Japan)을 이용한 효소법으로 측정하였다. 본 연구에서 LDL-C는 Friedewald 공식(LDL-C=TC–HDL-C–TG/5)을 이 용하여 계산하여 사용하였다. 당화혈색소(hemoglobin A1c, HbA1c) 는 HLC-723G7 (Tosho, Tokyo, Japan)을 이용한 high performance liq- uid chromatography 방법으로 측정하였다.
이상지질혈증의 유병 및 치료 여부는 설문조사와 혈액검사 결과 로 설정하였다. 설문조사에서 이상지질혈증이 없다고 답한 대상자 중에서도 LDL-C 160 mg/dL 이상, HDL-C 40 mg/dL 미만, TG 200 mg/
dL 이상, TC 240 mg/dL 이상 중 한 가지 이상 해당하면 이상지질혈증 이 있는 것으로 정하였다. 치료 여부에서는 설문조사 외에도 혈액검 사에서 이상지질혈증이 있다고 나온 사람 중 치료하지 않는 사람도 비치료군으로 추가 설정하였다.
청력검사, 이과 시진, 이과 0도 내시경 등 이비인후검사는 숙련된 이비인후과 전공의에 의해 진행되었으며, 청력검사는 소음이 차단 된 청력부스에서 자동화청력기기 Automated diagnostic audiometer (SA 203; Entomed, Malmo, Sweden)를 이용하여 양측에서 0.5, 1, 2, 3, 4, 6 kHz에서 검사를 시행하였다. 0.5, 1, 2 kHz의 평균 청력을 저주파수 평균 청력으로 하고, 3, 4, 6 kHz의 평균 청력을 고주파수 평균 청력 으로 정의하였다. 그리고 양측 중에 검사 결과가 더 나쁜 일측의 청 력을 평균 청력값으로 분석하였고, 난청은 평균 청력이 26 dB 이상 인 경우로 정의하였다.
3. 통계분석
대상자의 일반적인 특성은 성별에 따라서 t-검정과 카이제곱검정 을 이용하여 비교하였다. 이상지질혈증의 여부에 따른 평균 청력의 차이는 t-검정과 카이제곱검정으로 분석하였으며, 이상지질혈증이 있는 대상자 중 치료 여부에 따른 평균 청력의 차이는 1:2 age-sex
김동휘 외. 한국 성인 남녀에서 이상지질혈증 유병 및 치료 여부에 따른 평균 청력의 차이 Korean Journal of Family Practice
KJFP
matching을 하여 t-검정 및 카이제곱검정으로 분석하였다. 이상지질 혈증 유병 및 치료 여부와 난청의 연관성은 나이, 성별, 체질량지수, 혈압, 공복혈당, HbA1c, TC, TG, HDL-C, LDL-C, 음주, 흡연, 소음노 출 여부, 질병 유병 여부(고혈압, 당뇨, 심혈관 질환)를 보정한 후 로 지스틱 회귀분석을 이용하여 분석하였다.
통계분석은 IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) 프로그램을 사용하여 분석하였으며, P값이 0.05 미만인 경우 통계적으로 유의한 것으로 정의하였다.
결 과
1. 연구대상자의 특성
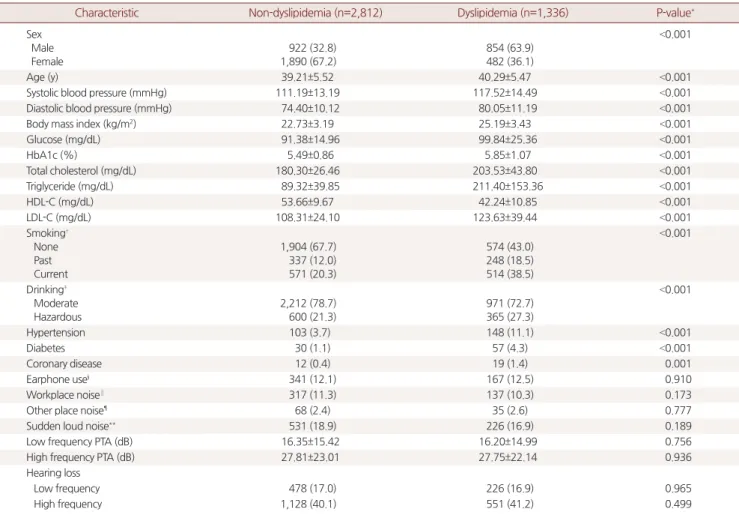
전체 대상자 중 이상지질혈증군이 1,336명(남자 854명, 여자 482 명), 정상군은 2,812명(남자 922명, 여자 1,890명)이었다. 평균 나이는 이상지질혈증군이 40.29세, 정상군이 39.21세로 유의한 차이를 보였 다. 혈압, 체질량지수, 공복혈당, HbA1c에서 정상군보다 이상지질혈 증군이 유의하게 더 높았다. 흡연군은 정상군 20.3%, 이상지질혈증 군 38.5%로 나타났고, 금연군은 정상군 12.0%, 이상지질혈증군 18.5%
로 나타났으며, 비흡연군은 각각 67.7%, 43.0%로 유의한 차이를 보였 다. 음주력에서 위험음주군은 정상군 21.3%, 이상지질혈증군 27.3%
로 나타났고, 건강음주군은 정상군 78.7%, 이상지질혈증군 72.7%로
Table 1. Baseline characteristics of the study population, comparison of characteristics and pure tone average between non-dyslipidemia and dys- lipidemia group (n=4,148)
Characteristic Non-dyslipidemia (n=2,812) Dyslipidemia (n=1,336) P-value*
Sex Male Female
922 (32.8) 1,890 (67.2)
854 (63.9) 482 (36.1)
<0.001
Age (y) 39.21±5.52 40.29±5.47 <0.001
Systolic blood pressure (mmHg) 111.19±13.19 117.52±14.49 <0.001
Diastolic blood pressure (mmHg) 74.40±10.12 80.05±11.19 <0.001
Body mass index (kg/m2) 22.73±3.19 25.19±3.43 <0.001
Glucose (mg/dL) 91.38±14.96 99.84±25.36 <0.001
HbA1c (%) 5.49±0.86 5.85±1.07 <0.001
Total cholesterol (mg/dL) 180.30±26.46 203.53±43.80 <0.001
Triglyceride (mg/dL) 89.32±39.85 211.40±153.36 <0.001
HDL-C (mg/dL) 53.66±9.67 42.24±10.85 <0.001
LDL-C (mg/dL) 108.31±24.10 123.63±39.44 <0.001
Smoking† None Past Current
1,904 (67.7) 337 (12.0) 571 (20.3)
574 (43.0) 248 (18.5) 514 (38.5)
<0.001
Drinking‡ Moderate Hazardous
2,212 (78.7) 600 (21.3)
971 (72.7) 365 (27.3)
<0.001
Hypertension 103 (3.7) 148 (11.1) <0.001
Diabetes 30 (1.1) 57 (4.3) <0.001
Coronary disease 12 (0.4) 19 (1.4) 0.001
Earphone use§ 341 (12.1) 167 (12.5) 0.910
Workplace noise∥ 317 (11.3) 137 (10.3) 0.173
Other place noise¶ 68 (2.4) 35 (2.6) 0.777
Sudden loud noise** 531 (18.9) 226 (16.9) 0.189
Low frequency PTA (dB) 16.35±15.42 16.20±14.99 0.756
High frequency PTA (dB) 27.81±23.01 27.75±22.14 0.936
Hearing loss
Low frequency 478 (17.0) 226 (16.9) 0.965
High frequency 1,128 (40.1) 551 (41.2) 0.499
Values are presented as number (%) or mean±standard deviation.
HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; PTA, pure tone average.
*P-value represented differences between male and female group by t-test for continuous variables, and chi-squared test for categorical variables. †Smoking none: never smoking or <5 packs, past ≥5 packs and stop smoking, current ≥5 packs and smoking. ‡Drinking moderate <2 times a week, hazardous ≥2 times a week. §Participants with a history of earphone use in noisy environment. ∥Participants with a history of workplace noise exposure (≥3 mo). ¶Participants with a history of noise exposure other place noise exposure (≥5 hour per week). **Participants with a history of exposure to acute explosive noise.
Dong-Hui Kim, et al. Association between Hearing Loss and Dyslipidemia Prevalence and Treatment
Korean Journal of Family Practice
KJFP
유의한 차이를 보였다. 고혈압은 정상군 3.7%, 이상지질혈증군 11.1%
로 나타났고, 당뇨는 각각 1.1%, 4.3%로 나타났으며, 심혈관 질환은 각 각 0.4%, 1.4%로 유의한 차이를 보였다. 소음노출 경험에서는 유의한 차이를 보이지 않았으며, 저주파수와 고주파수에서의 평균 청력과 난청의 빈도도 유의한 차이는 없었다(Table 1).
2. 이상지질혈증 치료 여부에 따른 평균 청력의 차이 및 난청의 빈도
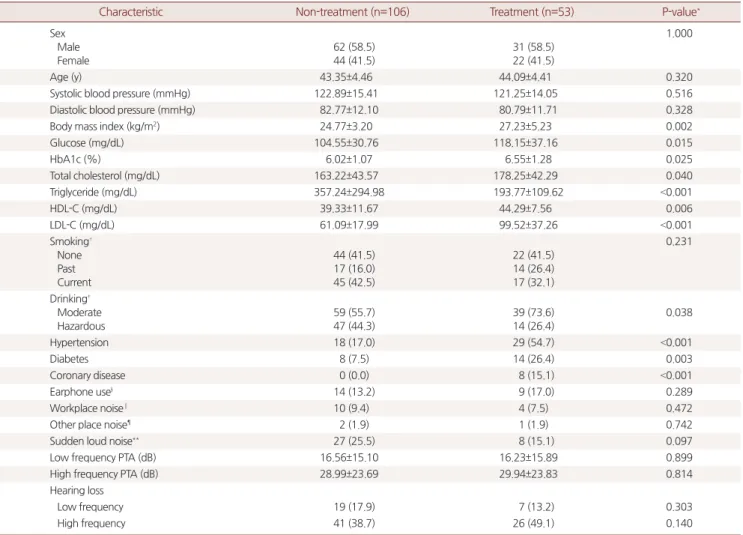
이상지질혈증군 중에서 치료군과 비치료군을 1:2 age-sex match- ing을 하여 치료군 53명, 비치료군 106명을 분석대상으로 하였다. 평 균 나이, 수축기혈압, 이완기혈압은 두 군 간에 유의한 차이를 보이 지 않았다. 체질량지수, 공복혈당, HbA1c, TC, HDL-C, LDL-C는 비치
료군보다 치료군에서 유의하게 더 높았으나, TG는 비치료군에서 유 의하게 더 높았다. 흡연력은 두 군 간에 유의한 차이를 보이지 않았 다. 음주력은 위험음주군은 치료군 26.4%, 비치료군 44.3%로 유의한 차이를 보였다. 고혈압은 치료군 54.7%, 비치료군 17.0%로 나타났고, 당뇨는 각각 26.4%, 7.5%, 심혈관 질환은 각각 15.1%, 0.0%로 유의한 차 이를 보였다. 소음노출 경험에서 유의한 차이를 보이지 않았으며, 저 주파수와 고주파수에서의 평균 청력과 난청의 빈도도 유의한 차이 는 없었다(Table 2).
3. 이상지질혈증 유병 및 치료 여부와 난청의 연관성
이상지질혈증 유병 여부와 난청의 연관성을 알아보기 위해 나이, 성별, 체질량지수, 혈압, 공복혈당, HbA1c, TC, TG, HDL-C, LDL-C, 음
Table 2. Comparison of characteristics and pure tone average between non-treatment and treatment group (n=159)
Characteristic Non-treatment (n=106) Treatment (n=53) P-value*
Sex Male Female
62 (58.5) 44 (41.5)
31 (58.5) 22 (41.5)
1.000
Age (y) 43.35±4.46 44.09±4.41 0.320
Systolic blood pressure (mmHg) 122.89±15.41 121.25±14.05 0.516
Diastolic blood pressure (mmHg) 82.77±12.10 80.79±11.71 0.328
Body mass index (kg/m2) 24.77±3.20 27.23±5.23 0.002
Glucose (mg/dL) 104.55±30.76 118.15±37.16 0.015
HbA1c (%) 6.02±1.07 6.55±1.28 0.025
Total cholesterol (mg/dL) 163.22±43.57 178.25±42.29 0.040
Triglyceride (mg/dL) 357.24±294.98 193.77±109.62 <0.001
HDL-C (mg/dL) 39.33±11.67 44.29±7.56 0.006
LDL-C (mg/dL) 61.09±17.99 99.52±37.26 <0.001
Smoking† None Past Current
44 (41.5) 17 (16.0) 45 (42.5)
22 (41.5) 14 (26.4) 17 (32.1)
0.231
Drinking‡ Moderate Hazardous
59 (55.7) 47 (44.3)
39 (73.6) 14 (26.4)
0.038
Hypertension 18 (17.0) 29 (54.7) <0.001
Diabetes 8 (7.5) 14 (26.4) 0.003
Coronary disease 0 (0.0) 8 (15.1) <0.001
Earphone use§ 14 (13.2) 9 (17.0) 0.289
Workplace noise∥ 10 (9.4) 4 (7.5) 0.472
Other place noise¶ 2 (1.9) 1 (1.9) 0.742
Sudden loud noise** 27 (25.5) 8 (15.1) 0.097
Low frequency PTA (dB) 16.56±15.10 16.23±15.89 0.899
High frequency PTA (dB) 28.99±23.69 29.94±23.83 0.814
Hearing loss
Low frequency 19 (17.9) 7 (13.2) 0.303
High frequency 41 (38.7) 26 (49.1) 0.140
Values are presented as number (%) or mean±standard deviation.
HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; PTA, pure tone average.
*P-value represented differences between male and female group by t-test for continuous variables, and chi-squared test for categorical variables. †Smoking none: never smoking or <5 packs, past ≥5 packs and stop smoking, current ≥5 packs and smoking. ‡Drinking moderate <2 times a week, hazardous ≥2 times a week. §Participants with a history of earphone use in noisy environment. ∥Participants with a history of workplace noise exposure (≥3 mo). ¶Participants with a history of noise exposure other place noise exposure (≥5 hour per week). **Participants with a history of exposure to acute explosive noise.
김동휘 외. 한국 성인 남녀에서 이상지질혈증 유병 및 치료 여부에 따른 평균 청력의 차이 Korean Journal of Family Practice
KJFP
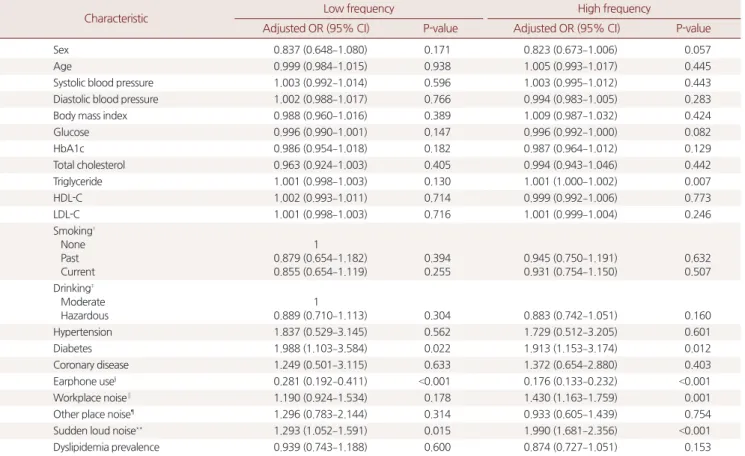
주, 흡연, 소음노출 여부, 질병 유병 여부(고혈압, 당뇨, 심혈관 질환) 를 보정한 후 로지스틱 회귀분석을 시행하였다. 저주파수에서 이어 폰 사용, 순간적 소음노출 여부, 당뇨 유무가 난청에 유의한 영향을 미치는 것으로 나타났는데, 이어폰을 사용한 군은 사용하지 않은 군에 비해 난청 발생이 0.281배로 나타났고, 순간적 소음노출이 있는 군은 1.293배, 당뇨가 있는 군의 위험도는 1.988배 높은 것으로 나타 났다. 이상지질혈증이 있는 경우가 없는 경우에 비해 난청의 교차비 가 0.939 (95% confidence interval [CI], 0.743–1.188)로 나타났으나 유의 한 결과는 아니었다. 고주파수에서는 TG, 이어폰 사용, 기계음 노출 여부, 순간적 소음노출 여부, 당뇨 유무가 난청에 영향을 미치는 것 으로 나타났다. TG의 영향은 1.001배, 이어폰 사용은 0.176배, 기계음 노출은 1.430배, 순간적 소음노출은 1.990배, 당뇨는 1.913배로 나타 났다. 이상지질혈증이 있는 경우가 없는 경우에 비해 난청의 교차비 는 0.874 (95% CI, 0.727–1.051)로 나타났으나 통계적으로 유의하지는 않았다.
이상지질혈증 치료 여부와 난청의 연관성을 알아보기 위한 분석 에서는 저주파수와 고주파수에서 이상지질혈증 치료군이 비치료 군에 비해 각각 난청의 교차비가 0.793 (95% CI, 0.167–3.763)과 0.761 (95% CI, 0.229-2.527)로 나타났으나 유의한 결과는 아니었다. 저주파 수에서는 난청에 대한 나이의 영향력은 1.141배로 나이가 높아질수 록 위험도가 높아지는 것으로 나타났다. 고주파수에서는 이어폰 사 용의 영향이 0.070배로 이어폰을 사용하지 않은 집단에 비해 위험도 가 낮아지는 것으로 나타났다(Tables 3, 4).
고 찰
본 연구에서는 제5기(2010–2012년) 국민건강영양조사에 참여한 30–49세 남녀를 대상으로 이상지질혈증 유병 및 치료 여부에 따라 평균 청력, 난청의 빈도에 차이가 있는지 알아보았다. 그 결과 이상지 질혈증군과 정상군은 저주파수와 고주파수 모두에서 평균 청력과
Table 3. Adjusted OR and 95% CI of hearing loss by prevalence of dyslipidemia*
Characteristic Low frequency High frequency
Adjusted OR (95% CI) P-value Adjusted OR (95% CI) P-value
Sex 0.837 (0.648–1.080) 0.171 0.823 (0.673–1.006) 0.057
Age 0.999 (0.984–1.015) 0.938 1.005 (0.993–1.017) 0.445
Systolic blood pressure 1.003 (0.992–1.014) 0.596 1.003 (0.995–1.012) 0.443
Diastolic blood pressure 1.002 (0.988–1.017) 0.766 0.994 (0.983–1.005) 0.283
Body mass index 0.988 (0.960–1.016) 0.389 1.009 (0.987–1.032) 0.424
Glucose 0.996 (0.990–1.001) 0.147 0.996 (0.992–1.000) 0.082
HbA1c 0.986 (0.954–1.018) 0.182 0.987 (0.964–1.012) 0.129
Total cholesterol 0.963 (0.924–1.003) 0.405 0.994 (0.943–1.046) 0.442
Triglyceride 1.001 (0.998–1.003) 0.130 1.001 (1.000–1.002) 0.007
HDL-C 1.002 (0.993–1.011) 0.714 0.999 (0.992–1.006) 0.773
LDL-C 1.001 (0.998–1.003) 0.716 1.001 (0.999–1.004) 0.246
Smoking† None Past Current
1 0.879 (0.654–1.182) 0.855 (0.654–1.119)
0.394 0.255
0.945 (0.750–1.191) 0.931 (0.754–1.150)
0.632 0.507 Drinking‡
Moderate Hazardous
1
0.889 (0.710–1.113) 0.304 0.883 (0.742–1.051) 0.160
Hypertension 1.837 (0.529–3.145) 0.562 1.729 (0.512–3.205) 0.601
Diabetes 1.988 (1.103–3.584) 0.022 1.913 (1.153–3.174) 0.012
Coronary disease 1.249 (0.501–3.115) 0.633 1.372 (0.654–2.880) 0.403
Earphone use§ 0.281 (0.192–0.411) <0.001 0.176 (0.133–0.232) <0.001
Workplace noise∥ 1.190 (0.924–1.534) 0.178 1.430 (1.163–1.759) 0.001
Other place noise¶ 1.296 (0.783–2.144) 0.314 0.933 (0.605–1.439) 0.754
Sudden loud noise** 1.293 (1.052–1.591) 0.015 1.990 (1.681–2.356) <0.001
Dyslipidemia prevalence 0.939 (0.743–1.188) 0.600 0.874 (0.727–1.051) 0.153
OR, odds ratio; CI, confidence interval; HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
*P-value and OR was calculated by logistic regression analysis. Adjusted for age, sex, body mass index, blood pressure, fasting glucose, HbA1c, triglyceride, HDL-C, LDL- C, alcohol, smoking, history of noise exposure, hypertension, diabetes, coronary disease. Chi-square: low frequency 81.23 (P<0.001), high frequency 317.27 (P<0.001).
Nagelkerke R square: low frequency 0.033, high frequency 0.101. †Smoking none: never smoking or <5 packs, past ≥5 packs and stop smoking, current ≥5 packs and smoking. ‡Drinking moderate <2 times a week, hazardous ≥2 times a week. §Participants with a history of earphone use in noisy environment. ∥Participants with a histo- ry of workplace noise exposure (≥3 mo). ¶Participants with a history of noise exposure other place noise exposure (≥5 hour per week). **Participants with a history of exposure to acute explosive noise.
Dong-Hui Kim, et al. Association between Hearing Loss and Dyslipidemia Prevalence and Treatment
Korean Journal of Family Practice
KJFP
난청의 빈도에 유의한 차이가 없었으며, 이상지질혈증 치료군과 비 치료군에서도 유의한 차이가 없었다.
이상지질혈증과 청력에 대해서 이전 연구들에서는 다양한 결과 들이 보고되었는데, 40세 이상 성인을 대상으로 한 Sousa 등5)의 연구 와 5–18세를 대상으로 한 Anbari 등11)의 연구 결과는 본 연구 결과와 마찬가지로 이상지질혈증과 청력은 관련이 없는 것으로 보고되었 다. 반면, 50세 남성을 대상으로 한 Axelsson과 Lindgren10)의 연구에 서는 이상지질혈증으로 인해 혈압이 상승되고, 말초혈관이 수축되 며, 동맥경화성 변화가 발생하여 달팽이관의 혈액 순환에 장애를 유 발시켜 감각신경성 청력 저하가 발생할 것이라 하였다. Spencer15)도 이상지질혈증과 청력이 관련이 있다고 보고하였다. Lee 등14)의 20세 이상 성인을 대상으로 한 연구에서는 이상지질혈증이 있는 군에서 오히려 청력이 더 좋았다는 보고도 있었다. 또한 이상지질혈증의 약 물 치료가 청력에 어떤 영향을 주는지에 대한 연구들도 결과가 다양 하였는데, Liu 등13)은 atrovastatin의 부작용으로 인해 30대 성인에서
비가역적인 청력 저하가 발생한다고 하였고, 40대 이상 성인을 대상 으로 한 Chung 등16) 의 연구에서도 statin 사용이 난청의 유병률을 증 가시킨다고 보고하였다. Olzowy 등12)은 3-hydroxy-3-methylglutaryl–
coenzyme A reductase inhibitors (statin)가 청력에 영향을 주지 않는다 고 하였고, 본 연구 결과에서도 이상지질혈증 유병 및 치료 여부가 평균 청력과 난청의 빈도에 영향을 주지 않았다. 그리고 청력에 영향 을 주는 요인들을 보정한 후 나온 결과도 통계적인 의미가 없었다. 이 번 연구는 기존의 연구들과는 다르게 노화성 난청의 영향을 배제하 기 위하여 난청의 유병률이 증가되는 50대 이상을 제외한 30–49세 만을 대상으로 하였기 때문에 혈액 순환 장애 등의 퇴행성 변화가 아직 진행되지 않아 발생한 결과일 수 있다고 생각된다.
이번 연구는 몇 가지 제한점이 있다. 첫 번째, 이번 연구는 단면 연 구이므로 이상지질혈증과 청력 간의 인과적 관계를 알 수 없었다. 두 번째, 국민건강영양조사 자료에서 이상지질혈증 치료 여부를 설문 조사만으로 진행하였고, 복용 약물에 대한 자료가 없어 자세한 연 Table 4. Adjusted OR and 95% CI of hearing loss by treatment of dyslipidemia*
Characteristic Low frequency High frequency
Adjusted OR (95% CI) P-value Adjusted OR (95% CI) P-value
Sex 1.943 (0.417–9.045) 0.397 0.473 (0.154–1.455) 0.192
Age 1.141 (1.001–1.301) 0.048 1.032 (0.944–1.128) 0.493
Systolic blood pressure 1.015 (0.965–1.068) 0.566 1.020 (0.979–1.063) 0.348
Diastolic blood pressure 0.995 (0.930–1.065) 0.887 0.977 (0.925–1.033) 0.419
Body mass index 0.935 (0.781–1.118) 0.458 1.099 (0.987–1.224) 0.086
Glucose 0.986 (0.963–1.008) 0.216 0.987 (0.971–1.003) 0.107
HbA1c 0.977 (0.911–1.044) 0.202 0.978 (0.925–1.032) 0.192
Total cholesterol 0.995 (0.967–1.024) 0.478 0.994 (0.958–1.031) 0.459
Triglyceride 1.001 (0.998–1.003) 0.576 1.000 (0.998–1.002) 0.869
HDL-C 0.994 (0.941–1.049) 0.819 1.006 (0.964–1.050) 0.771
LDL-C 0.997 (0.978–1.017) 0.798 1.032 (0.944–1.128) 0.493
Smoking† None Past Current
1 5.806 (0.889–37.90) 2.859 (0.550–14.86)
0.066 0.212
0.791 (0.206–3.034) 0.779 (0.238–2.551)
0.733 0.680 Drinking‡
Moderate Hazardous
1
0.931 (0.250–3.465) 0.915 0.572 (0.204–1.602) 0.288
Hypertension 0.913 (0.271–3.078) 0.884 1.357 (0.531–3.468) 0.524
Diabetes 4.074 (0.697–23.82) 0.119 4.547 (0.982–21.06) 0.053
Coronary disease 0.671 (0.047–9.592) 0.769 1.965 (0.329–11.76) 0.459
Earphone use§ 0.128 (0.014–1.168) 0.068 0.070 (0.013–0.378) 0.002
Workplace noise∥ 1.570 (0.377–6.549) 0.536 1.002 (0.270–3.716) 0.998
Other place noise¶ 2.007 (0.127–31.69) 0.621 2.185 (0.162–29.55) 0.556
Sudden loud noise** 1.346 (0.428–4.232) 0.611 2.170 (0.848–5.552) 0.106
Dyslipidemia treatment 0.793 (0.167–3.763) 0.770 0.761 (0.229–2.527) 0.655
OR, odds ratio; CI, confidence interval; HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
*P-value and OR was calculated by logistic regression analysis. Adjusted for age, sex, body mass index, blood pressure, fasting glucose, HbA1c, triglyceride, HDL-C, LDL- C, alcohol, smoking, history of noise exposure, hypertension, diabetes, coronary disease. Chi-square: low frequency 19.56 (P=0.485), high frequency 34.13 (P=0.025).
Nagelkerke R square: low frequency 0.198, high frequency 0.263. †Smoking none: never smoking or <5 packs, past ≥5 packs and stop smoking, current ≥5 packs and smoking. ‡Drinking moderate <2 times a week, hazardous ≥2 times a week. §Participants with a history of earphone use in noisy environment. ∥Participants with a histo- ry of workplace noise exposure (≥3 mo). ¶Participants with a history of noise exposure other place noise exposure (≥5 hour per week). **Participants with a history of exposure to acute explosive noise.
김동휘 외. 한국 성인 남녀에서 이상지질혈증 유병 및 치료 여부에 따른 평균 청력의 차이 Korean Journal of Family Practice
KJFP
구를 할 수 없었다. 대표적인 약물로는 statin, nicotinin acid, fibrate 등 이 있는데, 이러한 복용 약물에 대한 자료가 없어 치료 약물의 종류 나 용량에 따른 차이를 알 수 없었다. 세 번째, 청력에 영향을 주는 이 독성 약물에 대해서도 정확한 자료가 없어 조사하지 못하였다. 대표 적인 약물로는 aminoglycoside 계열의 항생제와 cisplatin과 같은 백금 (platinum)계 항암제 등이 있다.17) 네 번째, LDL-C는 직접 측정한 자 료가 부족하여 Friedewald 공식으로 계산한 값을 사용하였기 때문 에 TG가 높은 사람은 LDL-C 수치에 오류가 있을 수 있다.
본 연구는 이러한 제한점이 있지만, 국민건강영양조사라는 표준 화된 집단을 대상으로 연구가 이루어졌으며, 이전 연구들과는 다르 게 대상을 30–49세 남녀로 하였고, 이상지질혈증에 설문조사와 혈 액검사를 함께 반영하여 진단 받지 않은 대상자도 포함하여 진행된 연구라는 것에 의의가 있다. 아직까지는 이상지질혈증과 청력의 관 계에 대해 일관성 있는 결과가 없기 때문에 향후 이상지질혈증과 청 력의 명확한 관계를 밝히기 위한 추가적인 연구가 더 필요할 것으로 생각된다.
요 약
연구배경:
이상지질혈증이 청력에 영향을 줄 것이라는 가설이 있지 만, 아직까지는 다양한 연령층에서 진행된 여러 연구들에서 일관성 있는 결과가 없었다. 이에 본 연구에서는 30–49세 남녀를 대상으로 이상지질혈증 유병 및 치료 여부에 따른 평균 청력의 차이와 난청의 빈도, 연관성을 알아보았다.방법:
2010–2012년도 국민건강영양조사에 참여한 30–49세 남녀 4,148명을 대상으로 하였다. 이상지질혈증의 유병 및 치료 여부는 설 문조사와 혈액검사 결과로 정하였고, 설문에서 이상지질혈증이 없 다고 답한 대상자 중에서도 진단기준이 되면 이상지질혈증이 있다 고 설정하였으며, 이들 중 치료하지 않는 대상자들을 비치료군으로 추가 설정하였다. 청력은 양측에서 0.5, 1, 2 kHz를 저주파수 평균 청 력 3, 4, 6 kHz를 고주파수 평균 청력으로 하여 양측 중 결과가 더 나 쁜 일측의 청력을 청력값으로 분석하였다. 난청은 평균 청력이 26 dB 이상인 경우로 정의하였다.결과:
저주파수와 고주파수 평균 청력 모두에서 이상지질혈증군과 정상군 간의 평균 청력에 유의한 차이는 없었으며, 이상지질혈증 치 료군과 비치료군에서도 유의한 차이는 없었다. 이상지질혈증 유병 및 치료 여부와 난청의 연관성은 나이, 성별, 체질량지수, 혈압, 공복 혈당, 당화혈색소, 총콜레스테롤, 중성지방, 고지단백 콜레스테롤, 저 지단백 콜레스테롤, 음주, 흡연, 소음노출 여부, 질병 유병 여부(고혈 압, 당뇨, 심혈관 질환)를 보정한 후 분석하였으나 통계적으로 유의하지 않았다.
결론:
30–49세 성인 남녀에서 이상지질혈증 유병 및 치료 여부에 따 른 평균 청력의 차이는 없었고, 난청과도 관련이 없었다.중심단어:
이상지질혈증; 중년; 청력; 청력검사REFERENCES
1. Choi J, Chung WH. Age-related hearing loss and the effects of hearing aids. J Korean Med Assoc 2011; 54: 918-24.
2. Kim SH, Yeo SG. Presbycusis. Hanyang Med Rev 2015; 35: 78-83.
3. Korea Health Statistics 2009: Korea National Health and Nutrition Exami- nation Survey (KNHANESIV-3) [Internet]. Cheongju: Korea Centers for Disease Control and Prevention; 2011 [cited 2015 Dec 25]. Available from:
http://knhanes.cdc.go.kr.
4. Kim BH. Presbycusis: review for its environmental risk factors. Korean J Otolaryngol-Head Neck Surg 2006; 49: 962-7.
5. Sousa CS, Castro Júnior Nd, Larsson EJ, Ching TH. Risk factors for presby- cusis in a socio-economic middle-class sample. Braz J Otorhinolaryngol 2009; 75: 530-6.
6. Agrawal Y, Platz EA, Niparko JK. Risk factors for hearing loss in US adults:
data from the National Health and Nutrition Examination Survey, 1999 to 2002. Otol Neurotol 2009; 30: 139-45.
7. Kim S, Lim EJ, Kim HS, Park JH, Jang SS, Lee SH. Sex differences in a cross sectional study of age-related hearing loss in Korean. Clin Exp Otorhinolar- yngol 2010; 3: 27-31.
8. Noorhassim I, Rampal KG. Multiplicative effect of smoking and age on hearing impairment. Am J Otolaryngol 1998; 19: 240-3.
9. Kim JS, Yeh MH, Chun BY, Woo KH, Kang YS, Kim KY, et al. Effect of ciga- reet smoking on air-conduction hearing threshold level in adult men. Kore- an J Prev Med 1998; 31: 285-92.
10. Axelsson A, Lindgren F. Is there a relationship between hypercholesterolae- mia and noise-induced hearing loss? Acta Otolaryngol 1985; 100: 379-86.
11. Anbari S, Isazadeh D, Safavi A, Alaie M, Azizi F. The role of dyslipidemia in sensorineural hearing loss in children. Int J Pediatr Otorhinolaryngol 2010;
74: 32-6.
12. Olzowy B, Canis M, Hempel JM, Mazurek B, Suckfüll M. Effect of atorvas- tatin on progression of sensorineural hearing loss and tinnitus in the elderly:
results of a prospective, randomized, double-blind clinical trial. Otol Neu- rotol 2007; 28: 455-8.
13. Liu M, Alafris A, Longo AJ, Cohen H. Irreversible atorvastatin-associated hearing loss. Pharmacotherapy 2012; 32: e27-34.
14. Lee JS, Choi HG, Jang JH, Sim S, Hong SK, Lee HJ, et al. Analysis of predis- posing factors for hearing loss in adults. J Korean Med Sci 2015; 30: 1175-82.
15. Spencer JT Jr. Metabolic-syndromic sensorineural hearing loss and in- creased noise vulnerability. Ear Nose Throat J 2007; 86: 314.
16. Chung SD, Chen CH, Hung SH, Lin HC, Wang LH. A population-based study on the association between statin use and sudden sensorineural hear- ing loss. Otolaryngol Head Neck Surg 2015; 152: 319-25.
17. Sim HJ. Noise-induced hearing loss. Hanyang Med Rev 2015; 35: 84-91.