Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):752-757
KJFP
Korean Journal of Family Practice서 론
비만은 골관절염의 주요 원인이다.1,2,3) 우리나라
50
세 이상의 성 인 중 남자5
.1
%, 여자22
.4
%가 골관절염에 진단되었으며, 복부비 만을 가진 군의 골관절염이 정상군에 비해1
.9
배 더 높게 나타나 는 것으로 알려졌다.1) 비만으로 인한 체중 부하는 관절에 부담을 주어 골관절염 발생에 영향을 미치며,2) 대체로 골관절염으로 진단 된 군의BMI
와 허리둘레 측정치는 그렇지 않은 군에 비하여 더 높 은 것을 볼 수 있었다.3) 최근 연구에서는 비만 환자의 지방 조직에 서 분비되는 여러 아디포카인(adipokines
)들이in vitro
상에서 골 관절염의 병태 생리에 영향을 미치며, 특히 여러 염증성 사이토카인(
inflammatory cytikine
)의 반응을 촉진하는 것으로 알려진 렙틴 (leptin
)은 단백분해효소(proteolytic enzyme
)의 상향조절을 통하여 관절 연골 대사에 이화 작용(catabolic effect
)을 유도하는 것으로 알 려져 비만으로 인한 골관절염이 단순한 물리적인 압력 뿐 아니라, 대 사적인 요인도 관여하고 있음을 예측할 수 있다.4)나트륨과잉섭취는 체내 염증반응을 유발하는 주요한 인자로, 면 역 세포의 활성으로 염증반응을 촉진시켜 자가면역질환을 발생시키 고,5) 청소년기에 비만과 염증을 증가시킨다고 알려져 있으며,6) 골 내의 칼슘대사에 영향을 미쳐 칼슘의 소변배출을 증가시켜서 골 대 사에 부정적 영향7, 8, 9)을 주고 있다.
2011
년 우리나라 국민의 평균적인 소금 섭취는 약12g
(나트륨비만한 성인의 요나트륨 수치와 골관절염의 연관성:
제5기 국민건강영양조사(2010~2011) 자료이용
임현정, 이연지
*, 최지호, 조세욱, 안지은, 최병오
인하대학교 의과대학 가정의학교실
The association of urinary sodium level and osteoarthritis prevalence in Korean obese adults:
Using fifth Korean National Health and Nutrition Examination Survey in 2010~2011
Hyun-Jung Im, Yeon-Ji Lee
*, Ji-Ho Choi, Se-Wook Cho, Jee-Eun An, Byung-Ho Choi
Department of Family Medicine, Inha University School of Medicine, Incheon, KoreaBackground: Osteoarthritis (OA) in the obese results not only from mechanical burden but also from metabolic reactions involving inflammatory cytokines. Inflammatory reactions in the obese are associated with excessive sodium intake. This study was designed to investigate the relationship between urine sodium and osteoarthritis (OA) in obese Korean adults.
Methods: This study included a total of 1,822 obese adults over 50 years of age (725 men, 1,097 women) who participated in the fifth Korea National Health and Nutrition Examination of 2010~2011. We divided all subjects into tertiles according to urinary sodium levels corrected by urinary creatinine or specific gravity (SG), and OA was diagnosed by radiographs of the knee, hip and L-spine joint and by a self-reporting questionaire.
Results: Male participants who belonged to the lowest tertile in urinary sodium levels (T1) had significantly lower risk of knee OA than others. However, female participants did not exhibit a significant association between urinary sodium levels and OA. [U[Na
+]/SGU; 1.634( 95% CI: 1.076~2.484)]
Conclusion: Lower urinary sodium levels is associated with lower prevalence of knee OA in obese men, supporting the possible clinical value of U[Na
+]/SGU in general medical facilities.
Therefore, it may be advisable for obese men to reduce sodium intake in order to help prevent OA of the knees.
Keywords: Obesity, Osteoarthritis, Urinary sodium
Received February 27, 2015 Revised July 15, 2015 Accepted September 11, 2015 Corresponding Author Yeon-Ji Lee
Tel: +82-32-890-2240, Fax: +82-32-890-2195 E-mail:[email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
4791mg
)으로WHO
(세계보건기구)가 제시하는 권고기준5g
에 비 하면2
배 이상 높은 상태10)로, 나트륨에 의해 유발되는 대사 및 염 증 반응에 의한 질환에 이환 될 위험성이 큰 실정이다.비만 세포와 나트륨과잉섭취는 골 및 연골의 대사에 관여하고 있 으며, 염증반응을 유발하는 인자로써 연골의 염증에 의하여 발생하 는 골관절염에 직·간접적으로 영향을 줄 것으로 생각되어진다.
이에 저자는 비만한 우리나라 성인을 대상으로 요 나트륨과 골관 절염의 연관 관계를 연구해 보고자 한다.
방 법
1. 연구 대상
본 연구는 제
5
기, 국민 건강 영양 조사 중2010
년,2011
년도 자료를 이용하여 만50
세 이상의 성인을 대상으로 비만치료 지침 (2010
)11)에서 제시한 진단기준인 체질량지수(BMI
)가25kg
/m
2이상 이거나, 허리둘레 여자의 경우85cm
이상, 남자는90cm
이상인 남 자725
명, 여자1097
명, 총1822
명을 연구 대상으로 하였으며,GFR 25
% 이하이거나 신장 기능에 이상을 보이는 사람, 설문지 작성을 완료하지 못한 사람, 혈액 검사 및 방사선 검사가 누락된 경우는 연 구 대상에서 제외하였다.이들의 원시자료에서
2010
년,2011
년 무릎, 엉덩, 요추관절염에 대한 설문지 및 방사선검사(Dual
-Energy X
-ray absorptiometry
,DXA
)결과 자료를 이용하였고,2010
년,2011
년 자료에서 요중 나트륨과 요중 크레아티닌, 요 비중 결과를 이용하였다. 요중 나트 륨 측정은 국민 건강 영양 조사에서
2011
년까지만 시행되었으므로,2012
년 자료는 제외하고 제5
기 자료 중,2010
년과2011
년 자료를 이용하였다.2. 연구 내용 및 방법
1) 일반적 특성 및 건강 행태 요인 변수
일반적 특성에 대한 관련 요인으로 가구의 소득 수준, 교육 수준, 배우자 유무, 거주 지역을 설문조사를 통해 수집하였고, 건강 행태 관련 요인으로 비만인 남녀 간 평균
BMI
지수, 평균 허리 둘레, 평 균 수축기 및 이완기 혈압, 평균 공복 혈당, 흡연 유무, 고위험 음주 여부, 운동 실천 여부를 설문조사와 검진 조사를 통해 확인하였다.소득 수준은 가구당 소득 수준을 사분위로 나누어서 하위
25
%이내 의 군과 그렇지 않은 군으로 구분하였고. 교육 수준은 최종학력이 고졸(9
~11
년) 이상인 경우를 고학력군으로 구분하였으며, 배우자 는 결혼 유무와 관계없이 배우자와 함께 사는 군과 혼자 사는 군(사 별, 이혼, 별거, 미혼)으로 나누었고, 거주 지역은 시에 해당하는 지 역에 거주하는 군과 그렇지 않은 군으로 구분하였다. 흡연 유무는 현재 담배를 피우는 경우와 피우지 않은 경우의 두 군으로 구분하였으며, 알코올 섭취는 소비된 순수한 알코올의 양을 술의 종류와 상 관 없이 음주 빈도와 섭취한 술병의 수를 이용하여 일일당 소비하는 양을 계산하였으며, 측정치가 일일당
30g
(그람) 이상인 경우를 고 위험 음주군으로 정의하였다. 운동의 평가는 주3
일 이상,1
회20
분 이상의 격렬한 신체활동을 하였거나, 주5
일 이상 중등도의 신체 활 동1
회30
분 이상 실천한 경우로 구분하였다.2) 임의뇨 검사 및 농도 측정 자료
총
1822
명의 연구 대상 남녀에게 임의뇨 표본을 채취하여 수집하 였고, 요중 나트륨과 크레아틴의 값은Hitachi Automatic Analyzer 7600
(Hitachi
/Japan
)를 이용하여 측정하고, 요비중 값은Uris ys2400
(Roche
/Germany
)분석기를 사용하여 측정하였다.12)임의뇨 나트륨농도가 희석 또는 농축 상태로 측정되었을 가능 성을 배제하기 위하여 요 농도를 보정하는 식; 요중나트륨/요중크 레아티닌(
U
[Na
+]/Cr
) 비, 혹은 요중나트륨/요비중[(요비중-1
)×100
)](U
[Na
+]/SGU
[(SG
-1
)×100
]을 사용하여 교정13, 14, 15)하였고, 측정된 값은 삼분위(tertile
) 로 나누어 비교하였다.GFR
은ID
-MS traceable Modification of Diet in Renal Disease
(MDRD
)16) 연산 방정식을 이용하여 평가하였다.3) 골관절염의 정의
국민 건강 영양 조사 제
5
기(2010
~2011
)에 만50
세 이상을 대 상으로 무릎 관절과 엉덩 관절, 요추 관절의 통증 여부에 대한 설 문 조사 및 방사선 촬영을 시행하였다. 무릎 관절과 엉덩 관절은Kellgren
-Lawrence grading scale
17)을 이용하여 등급을 부여하였으 며, 요추 관절은Kellgren
&Lawrence
(1957
)에 준하여 진단기준을 개발하고, 등급평가는Yoshimura
등(2009
)로 나누었다.18) 퇴행성 골 관절염(Osteoarthritis
)은 방사선 상Kellgren
-Lawrence grade 2
등 급이상17) 혹은 관절 통증을 호소하는 경우로 정의 하였다.4) 통계 분석
연구 대상자들의 일반적 특성은 성별에 따라서 연속형 변수는 평 균± 표준오차, 범주형 변수는 %(표준오차)로 제시하고, 각각
t
검 정 및 카이제곱 검정을 이용하여 비교하였다. 골관절염과 요중 나 트륨 농도(U
[Na
+],U
[Na
+]/Cr
또는,U
[Na
+]/SGU
)와의 관련성을 보기 위해서 각각을 삼분위(tertile
)로 나누고, 연령과BMI
를 보정 한 모형 (Model 1
)과 연령,BMI
, 흡연력, 음주력, 운동 행태를 보 정(Model 2
)하여 다중 로지스틱 회귀분석을 시행하여 교차비(95
% 신뢰구간)로 제시하였다. 통계 분석은SAS ver
.9
.2
(SAS Institute
,Cary
,NC
,USA
)를 이용하여 시행하였고, 복합 표본설계를 시행 하여 위해Survey procedure
를 이용하였다. 통계학적 유의 수준은P
-value
<0
.05
로 하였다.yun-Jung Im, et al. The association of urinary sodium level and osteoarthritis prevalence in Korean obese adults:
Using fifth Korean National Health and Nutrition Examination Survey in 2010~2011
Korean Journal of Family Practice
KJFP
결 과
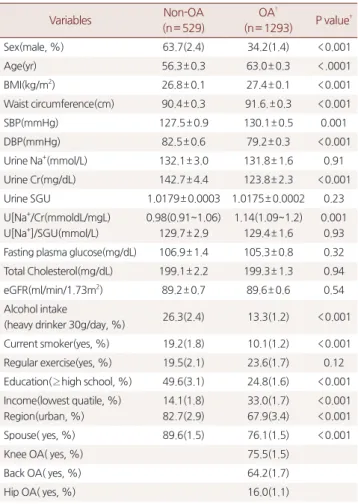
1. 연구대상자의 특성 (Table 1)
연구대상자 총
1822
명 중, 골관절염으로 진단된 군은1293
명 이 었으며, 이 중 남자의 비율은34
.2
%였다. (P
<0
.001
) 평균 연령, 평 균 체질량지수, 평균 허리둘레는 골관절염으로 진단된 군에서 그렇 지 않은 군에 비해 높게 나타났다.(OA
;63
.8
.±0
.3
세,Non
-OA 57
.7
±0
.3
세,OA
;27
.4
±0
.1 kg
/m
2,Non
-OA
;26
.8
±0
.1kg
/m
2,OA
;91
.6
±0
.3cm
,Non
-OA
;90
.4
±0
.3cm
,P
<0
.001
), 골 관절염이으로 진단된 군에서 음주 빈도와 흡연은 유의하게 낮게 나 타났고, 운동 비율은 더 높았으며, 교육 및 수입, 배우자의 존재는 유의하게 낮게 나타났다. 골관절염 중, 무릎관절염은75
.5
%, 허리 관절염64
.2
%, 엉덩관절염은16
.0
%로 나타났으며, 대부분 중복되 어 진단되었다.2. 요 나트륨 삼분위(Tertile)와 무릎관절염 유병률에 대한 남 녀간의 분 석 (Table 2, Figure 1)
무릎 관절염으로 진단된 경우, 남자에서 요 나트륨 삼분위 (
Tertile
) 중 가장 낮은 구간에서(T1
) 관절염 유병률이 유의하게 가 장 낮았다. (U
[Na
+];25
.6
%,P
=0
.0489
,U
[Na
+]/SGU
;25
.6
%,P
=0
.0481
) 그러나 여성의 경우, 무릎, 요추, 엉덩관절염의 모든 경 우에서 요 나트륨과 상관 관계가 유의하지 않았다. 이것을, 요 나 트륨이 낮은 군(T1
)과 그렇지 않은 군(T2
,3
)으로 분류하고, 요 나 트륨과 관절염과의 유병률의 상관 관계를 보면,(Figure 1
) 무릎관 절염이 진단된 남자는, 요 나트륨값(U
[Na
+],U
[Na
+]/SGU
)이 낮 은 군(Tertile 1
)에서 유병률이 유의하게 낮았다. (U
[Na
+]25
.6
%,P
=0
.0292
,U
[Na
+]/SGU 25
.6
%,P
=0
.0292
) 반면, 여자는 요 나트 륨과 무릎 골관절염과의 유병률의 상관관계는 유의하지 않았다. 그 밖의 요 나트륨과 엉덩 관절염, 요 나트륨과 요추 관절염의 유병률 과의 관계는 남, 녀 모두에서 유의하지 않았다.Table 1. Basal Characteristics of study populations by presence or absence of OA*
Variables Non-OA
(n= 529)
OA†
(n= 1293) P value‡
Sex(male, %) 63.7(2.4) 34.2(1.4) <0.001
Age(yr) 56.3± 0.3 63.0± 0.3 <.0001
BMI(kg/m2) 26.8± 0.1 27.4± 0.1 <0.001
Waist circumference(cm) 90.4± 0.3 91.6.± 0.3 <0.001
SBP(mmHg) 127.5± 0.9 130.1± 0.5 0.001
DBP(mmHg) 82.5± 0.6 79.2± 0.3 <0.001
Urine Na+(mmol/L) 132.1± 3.0 131.8± 1.6 0.91
Urine Cr(mg/dL) 142.7± 4.4 123.8± 2.3 <0.001
Urine SGU 1.0179± 0.0003 1.0175± 0.0002 0.23
U[Na+/Cr(mmoldL/mgL) U[Na+]/SGU(mmol/L)
0.98(0.91~1.06) 129.7± 2.9
1.14(1.09~1.2) 129.4± 1.6
0.001 0.93 Fasting plasma glucose(mg/dL) 106.9± 1.4 105.3± 0.8 0.32 Total Cholesterol(mg/dL) 199.1± 2.2 199.3± 1.3 0.94
eGFR(ml/min/1.73m2) 89.2± 0.7 89.6± 0.6 0.54
Alcohol intake
(heavy drinker 30g/day, %) 26.3(2.4) 13.3(1.2) <0.001 Current smoker(yes, %) 19.2(1.8) 10.1(1.2) <0.001 Regular exercise(yes, %) 19.5(2.1) 23.6(1.7) 0.12 Education(≥ high school, %) 49.6(3.1) 24.8(1.6) <0.001 Income(lowest quatile, %)
Region(urban, %)
14.1(1.8) 82.7(2.9)
33.0(1.7) 67.9(3.4)
<0.001
<0.001
Spouse( yes, %) 89.6(1.5) 76.1(1.5) <0.001
Knee OA( yes, %) 75.5(1.5)
Back OA( yes, %) 64.2(1.7)
Hip OA( yes, %) 16.0(1.1)
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure;
eGFR: estimated Glomeru-
Lar filtration rate; Cr: creatinine; SGU: specific gravity unit, (urine SG-1.0) × 100;
U[Na+]/Cr: urinary sodiu-
m/creatinine ratio; U[Na+]/SGU: urinary sodium/specific gravity unit ratio ;OA, osteoarthritis.
* Data are presented as mean±SE or percentage(SE).
*Geometric mean(95% CI)
† Knee or hip or back OA was defined by Kellgren-Lawrence grade ≥2 or has symptomatic arthralgia
‡ P-values were obtained by Student's t-test or Chi-square test.
Table 2. Knee OA prevalence according to urinary sodium excretion*
Variables Male(n= 725)
P† Female(n= 1097)
P||
T1† T2‡ T3§ T1† T2‡ T3§
Urine Na+ 25.6(3.5) 38(3.9) 32.1(3.6) 0.04 65.1(3.2) 59.9(3.6) 65.1(3.2) 0.45
U[Na+/Cr 31.4(3.1) 31.9(3.6) 35(4.6) 0.81 66.2(3.6) 58.3(3.3) 65.7(3.0) 0.15
U[Na+]/SGU 25.6(3.5) 38(3.9) 32.1(3.6) 0.04 65.8(3.2) 59.1(3.7) 65.1(3.2) 0.30
OA, osteoarthritis; U[Na+]/Cr: urinary sodium/creatinine ratio; U[Na+]/SGU: urinary sodium/specific gravity unit ratio.
* Data are presented as percentage(SE).
† The lowest interval in each tertile(urinary sodium, urinary sodium/creatinine, urinary sodium,/specific gravity unit ratio)
‡ The median interval in each tertile(urinary sodium, urinary sodium/creatinine, urinary sodium,/specific gravity unit ratio)
§ The highest interval in each tertile(urinary sodium, urinary sodium/creatinine, urinary sodium,/specific gravity unit ratio) Tertile of Urine Na+(mmol) for men, women: ≤109(T1), 110~151(T2), and > 151(T3)
Tertile of U[Na+]/Cr(mmol/mmol) for men, women:≤0.89172(T1), 0.89173~1.563(T2), and >1.563(T3).
Tertile of U[Na+]/SGU for men, women: ≤107.283(T1),107.284~148.728(T2), and >148.728(T3).
|| P-values were obtained by Chi-square test
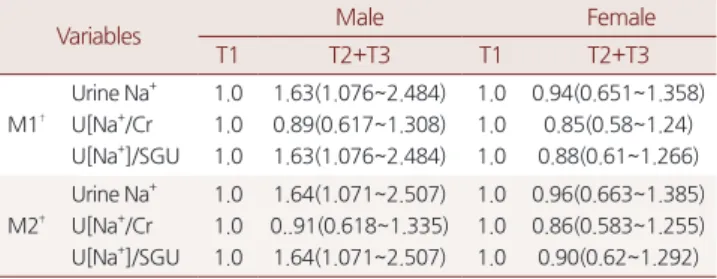
3. 요 나트륨 값과 무릎관절염의 교차비 (Table 3)
요 나트륨 삼 분위 중 유의한 값을 갖는 가장 낮은 구간(
T1
)과 낮 지 않은 구간(T2
+3
) 으로 나누어 무릎관절염과의 연관성을Table 3
에 제시하였다. 나이와BMI
를 보정한 모델 (Model 1
)에서 남자의 경우, 요 나트륨 (U
[Na
+]/SGU
)과 무릎 관절염 사이에서T1
과 비 교한T2
+T3
의 교차비가 유의한 양의 연관성을 있었고, [U
[Na
+];1
.634
(95
%CI
:1
.076
~2
.484
),U
[Na
+]/SGU
;1
.634
(95
%CI
:1
.076
~2
.484
)] 여자는 요 나트륨과 무릎관절염 사이에 유의한 연 관성이 없었다. 나이,BMI
, 음주, 흡연, 운동을 포함하여 보정한 모 델(Model 2
)에서 남자는 요 나트륨(U
[Na
+]/SGU
)과 무릎관절염 사 이에T1
과 비교한T2
+3
의 교차비가 유의한 양의 연관성을 보였 으나,U
[Na
+]1
.639
(95
%CI
:1
.071
~2
.507
)),U
[Na
+]/SGU 1
.639
(95
%CI
:1
.071
~2
.507
) 여자는 요 나트륨과 무릎관절염 사이에 유 의한 연관성이 없었다.요 나트륨과 엉덩 관절염 및 요추관절염과의 연관성에서는 남 녀 모두에서
M1
,M2
가 유의하지 않았다.고 찰
이번 연구는 요 나트륨 수치와 골 관절염과의 관계를
50
세 이상 의 비만 집단을 대상으로 시행하였으며, 비만인 남성에서 요 나트 륨 값이 가장 낮은 구간(T1
)에서 무릎 관절염의 유병률이 가장 낮았 고,T1
과T2
+T3
사이의 무릎 관절염의 교차비가 약1
.63
배로 나타 났다.65
세 이상을 대상으로 시행한 골관절염의 관련요인에 대한 연 구12
)에서는 골관절염의 위험인자로 고령, 여성, 비만, 농촌 거주, 낮은 교육 수준과 낮은 소득 수준, 비타민A
와 리보플라빈의 평균 권장량 이하로의 섭취 등을 제시하였다. 국내외 여러 연구에서 고령, 여성, 비만은 골관절염의 위험 요인으로 제시되고 있으며,1-
3) 특히 비만은 체중 부하에 의한 관절 부담이 그 원인으로 여겨졌 다. 그러나 최근에는 이러한 물리적인 접근 이외에 대사적인 접근 에 대한 연구가 이루어지고 있다. 대사증후군에서 무릎관절염을 일 으키는 요인은 단순한 체중 부하만이 아니라, 인슐린 저항성과 대 사적 혼란(
metabolic disturbance
), 염증 및 고혈압 등이 있을 수 있 으며,19) 지방세포는 렙틴(leptin
), 아디포넥틴(adiponectin
), 레시스 틴(resistin
), 비스파틴(visfatin
) 등의 여러아디포카인(adipokines
)들 을 분비하며,20) 그 중에서 렙틴(leptin
)은 여러 염증성 사이토카인 (inflammatory cytokine
)의 반응을 촉진시키고, 관절 연골 대사에서 단백분해효소(proteolytic enzyme
)의 상향 조절(up
-regulation
)을 통하여 이화 작용(catabolic effect
)을 유도4, 21) 한다고 제시하였다.소금과다섭취 또한 체내 염증 반응을 유발한다는 연구도 있다.
나트륨과잉섭취는
in vivo
에서p38
/MAPK pathway
를 활성화시키 고, 이로 인하여Th17
세포의 작용이 항진되며,Th17
세포는 면역 세포의 활성화를 유도하고,GM
-CSF
,TNFα
,IL
-2
등의 염증 반 응을 유발 하는 사이토카인(cytokine
)을 상향 조절(up
-regulation
) 시켜 자가면역질환을 유발한다고 하였다.5) 또한, 청소년기의 나트 륨과잉섭취는 체중,BMI
, 허리둘레, 체지방률, 지방량(fat mass
) 피하복부지방조직, 렙틴(leptin
), 종양괴사인자(tumor necrosis factor
-α
)들과 독립적으로 연관되어 있으며, 이들은 모두 체내 염증 반응을 유도하므로 비만과 체내염증반응을 증가시킬수 있다.6)즉, 비만한 군에서 소금의 과잉 섭취는 염증 반응에 의한 비정상 적 대사 작용을 더욱 촉진시킬 수 있고, 결국 골관절염의 유병률를 증가시킬 수 있다고 할 수 있다. 그러므로 소금섭취량이 많은 우리 나라의 경우, 이들의 상호 관계를 규명할 필요가 있다고 생각 된다.
그러나 이 연구는 몇 가지 제한점이 있다. 첫 번째, 단면 연구이 므로 골관절염과 소금 섭취량간의 선후 관계를 밝힐 수 없고, 두 번 째, 소금섭취량을 예측하는 보정 값이 정확한 소금섭취량을 반영하 Figure 1. Knee OA prevalence according of divided to T1 and T2,3 for
Tertile of urinary sodium/creatinine ratio and Tertile of urinary sodium/
specific gravity unit ratio by gender
[Na+]/Cr(mmol/mmol): urinary sodium/creatinine ratio; SGU: specific gravity unit,(urine SG-1.0)×100; U[Na+]/SGU: urinary sodium/specific gravity unit ratio.
* Urine Na+ ; P = 0.0292; U[Na+]/SGU: P = 0.0292( P<0.05) P-values were obtained by Chi-square test.
Table 3. Multivariate-adjusted ORs and 95% CIs of Knee OA acording to urinary sodium excretion*
Variables Male Female
T1 T2+T3 T1 T2+T3
M1†
Urine Na+ U[Na+/Cr U[Na+]/SGU
1.0 1.0 1.0
1.63(1.076~2.484) 0.89(0.617~1.308) 1.63(1.076~2.484)
1.0 1.0 1.0
0.94(0.651~1.358) 0.85(0.58~1.24) 0.88(0.61~1.266)
M2‡
Urine Na+ U[Na+/Cr U[Na+]/SGU
1.0 1.0 1.0
1.64(1.071~2.507) 0..91(0.618~1.335) 1.64(1.071~2.507)
1.0 1.0 1.0
0.96(0.663~1.385) 0.86(0.583~1.255) 0.90(0.62~1.292) OR: odds ratio; CIs, confidence intervals; [Na+]/Cr(mmol/mmol): urinary sodium/
creatinine ratio; SGU: specific gravity unit, (urine SG-1.0)×100; U[Na+]/SGU:
urinary sodium/specific gravity unit ratio; T1: Tertile 1;T2: Tertile 2; T3: Tertile 3.
* Data are presented as ORs(95% CIs).
† Model 1 was adjusted for age, BMI
‡ Model 2 was adjusted for age, BMI, smoking status, alcohol consumption and exercise
yun-Jung Im, et al. The association of urinary sodium level and osteoarthritis prevalence in Korean obese adults:
Using fifth Korean National Health and Nutrition Examination Survey in 2010~2011
Korean Journal of Family Practice
KJFP
는지를 확인할 수 없다는 점, 그리고 세 번째로 비만군을 대상으로 시행한 연구이므로 정상체중인 사람에게 일반화 할 수 없으며, 네 번째, 나트륨 배설에 영향을 주는 약물의 복용 유무를 확인할 수 없 어 제외기준을 세우지 못했다는 점, 다섯 번째로 골관절염의 조작 적 진단 상, 과잉추정의 가능성을 배제 할 수 없다는 것이다. 그러 나 이 연구는 우리나라의 대표성 있는 표본을 통해 얻어진 국가 자 료를 이용한 연구라는 점과 요 나트륨 수치와 골관절염간의 통계적 유의성을 확인한 연구라는 점에서 의의가 있겠다.
이 연구는 엉덩 관절, 요추 관절염도 포함하였으나 요 나트륨과 유의한 관계를 보이지 않았다. 이는 표본수가 현저히 적고, 무릎관 절에 비해 체중부하를 적게 받아 반응이 적을 수 있겠다. 또한, 여 성에서 요 나트륨과 무릎관절염의 관계가 유의하지 않았는데, 이는 남성에 비해 근육량이 적고, 호르몬 등과 같은 다양한 교란변수가 작용한 것으로 생각되어지나, 추 후 나트륨 섭취량과 골관절염의 관계 및 정확한 기전를 밝히는 연구가 필요할 것으로 생각된다.
요 약
연구배경: 비만과 나트륨 과잉섭취는 체내 염증반응을 유발하는 요 소로, 골 및 연골 대사에 직·간접적인 영향이 주는 것으로 알려져 있다. 저자는 비만한 성인의 나트륨 섭취량과 골관절염과의 연관성 을 연구하고자 하였다.
방법: 국민 건강 영양 조사(
2010
~2011
)자료를 이용하여50
세 이상 의 비만한 남녀를 대상으로, 요 나트륨 측정치를 얻어 삼분위로 나 누고, 무릎, 엉덩, 요추관절의 방사선 값이K
-L grade 2
이상이거 나 설문조사에서 관절통을 호소하는 경우를 골관절염으로 정의하 여 이들의 상관 관계를 유병률을 통해 확인하였다.결과: 남자에서 요 나트륨 값이 적을수록(
T1
) 무릎 관절염의 발 생률이 낮았다. (U
[Na
+]/SGU
;25
.6
%,P
=0
.0481
) 그러나 엉덩 관절 및 요추관절에서는 요 나트륨과 연관성이 없었다. 여자의 경 우 모든 관절염에서 요 나트륨과 상관 관계가 없었다. 나이와BMI
를 보정한 모델(Model 1
)과 나이와BMI
, 음주, 흡연, 운동을 보정 한 모델(Model 2
)에서 남자의 경우, 요 나트륨 (U
[Na
+]/SGU
)과 무 릎 관절염 사이의 교차비가 유의한 양의 연관성을 나타내었다. , [U
[Na
+]/SGU
;1
.634
(95
%CI
:1
.076
~2
.484
),U
[Na
+]/SGU 1
.639
(95
%CI
:1
.071
~2
.507
)] 반면, 여자는 요 나트륨과 골관절염 사이 에 유의한 연관성이 없었다결론: 비만한 성인 남자에서 요 나트륨 값의 삼분위 중 가장 낮은 구간에서 무릎 관절염의 유병률은 가장 낮았으며, 이것은 여러 요
소를 보정한 교차비에서도 유의한 양의 연관성을 보였다. 따라서 비만한 남자에서 싱겁게 먹는 식습관은 무릎관절염의 예방에 도움 을 줄 수 있다.
중심단어: 비만, 골관절염, 요 나트륨
REFERENCES
1. Hye-Ryoung, Eun-Jung,kim. Prevalence of Osteoarthritis and Its Affecting Factors among a Korean Population Aged 50 and Over.
Journal of Korean Public Health Nursing. 2013 :27(1); 27-39 2. Chong-Hyeon Yoon. Osteoarthritis Update. The Korean Journal of
Internal Medicine.2012:82(2);170~174
3. HyeSang Lee. Prevalence of Osteoarthritis and Related Risk Factors in the Elderly: Data from the Fifth Korea National Health and Nutrition Examination Survey (KNHANES V), 2010∼2012. J korea Diet Assoc 2014: 20(2): 99-109
4. Sunggun Lee, Tae-Nyun Kim, and Seong-Ho Kim. Sarcopenic Obesity Is More Closely Associated With Knee Osteoarthritis Than Is Nonsarcopenic Obesity. ARTHRITIS & RHEUMATISM. 2012.
December: 64(12); 3947–3954
5. Markus Kleinewietfeld,1,2* Arndt Manzel,3,4 Jens Titze,5,6Heda Kvakan,7,8Nir Yosef,2Ralf A. Linker et al. Sodium Chloride Drives Autoimmune Disease by the Induction of Pathogenic Th17 Cells Nature. Apr 25, 2013; 496(7446): 518–522.
6. Haidong Zhu, MD, PhD, Norman K. Pollock, PhD, Ishita Kotak, MPH, Bernard Gutin, PhD, Xiaoling Wang, MD, PhD, Jigar Bhagatwala, MBBS, MPH, et al. Dietary Sodium, Adiposity, and Inflammation in Healthy Adolescents.official journal of the american academy of pedoatrics.2014.feb:1-8 http://pediatrics.
aappublications.org/content/early/2014/01/28/peds.2013-1794 7. Yamaguchi T, Sugimoto T, Yano S, Yamauchi M, Sowa H, Chen Q.
Plasma lipids and osteop-orosis in postmenopausal women. Endocr J 2002; 49: 211-217
8. Parhami F, Jackson SM, Tintut Y, Le V, Balucan JP, Territo M.
Atherogenic diet and minimally oxidized low density lipoprotein inhibit osteogenic and promote adipogenic differentiation of marrow stromal cells.
J Bone Miner Res
1999; 14: 2067-2078 9. Park, JiyounㆍChoi, MiyounㆍLee, SeonheuiㆍChoi, YoonhoㆍPark,Yookyoung. The Association between Bone Mineral Density, Bone Turnover Markers, and Nutrient Intake in Pre- and Postmeno- pausal Women.
Korean J Nutr
2011; 44 (1): 29 ~ 4010. Ministry of Health and Welfare. korean' sodium intake is still high. [cited 2011 Nom. 20]. Available from: http://www.mw.go.
kr/front_new/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_
ID=0403&CONT_SEQ=279051&page=1
11. Korean Endocrine Society, Korean Society for the Study of Obesity.
Management of Obesity, 2010 Recommendation: Endocrinol Metab 25(4):301-304, December 2010
12. Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 2006;145:247–54.
13. Sang-Guk Lee , Woonhyoung Lee , Oh Hun Kwon , Jeong-
Ho Kim. Association of urinary sodium/creatinine ratio and urinary sodium/specific gravity unit ratio with blood pressure and hypertension: KNHANES 2009–2010 ; Clinica Chimica Acta 424 (2013) 168–173
14. Newman DJ, Pugia MJ, Lott JA, Wallace JF, Hiar AM. Urinary protein and albumin excretion corrected by creatinine and specific gravity. Clin Chim Acta 2000;294:139–55.
15. Moore Jr RR, Hirata-Dulas CA, Kasiske BL. Use of urine specific gravity to improve screening for albuminuria. Kidney Int 1997;52:240–3.
16. Vickery S, Stevens PE, Dalton RN, van Lente F, Lamb EJ. Does the ID-MS traceable MDRD equation work and is it suitable for use with compensated Jaffe and enzymatic creatinine assays? Nephrol Dial Transplant 2006;21:2439–45.
17. Kellgren JH, Lawrence JS. Radiological assessment of osteoarthritis.
Ann Rheum Dis 1957; 16: 494-502.
18. Yoshimura N et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab. 2009;27(5):620-8.
19. Chang Dong Han, Ik Hwan Yang, Woo Suk Lee, Yoo Jung Park and Kwan Kyu Park. Correlation between metabolic syndrome andknee osteoarthritis: data from the Korean National Health and Nutrition Examination Survey (KNHANES). Han et al. BMC Public Health 2013, 13:603
20. Hu PF, Bao JP, Wu LD. The emerging role of adipokines in osteoarthritis: a narrative review. Mol Biol Rep 2011;38:873–8.
21. Hui W, Litherland GJ, Elias MS, Kitson GI, Cawston TE, Rowan AD, et al. Leptin produced by joint white adipose tissue induces cartilage degradation via upregulation and activation of matrix metalloproteinases. Ann Rheumatic Dis 2012;71:455–62.