서 론
말기 콩팥병(end stage renal disease) 환자들은 심혈관질환의 유병 률(mobidity) 및 사망률(mortality)이 높다고 알려져 있다.1) 또한 고령 화 속도가 빨라지면서 당뇨병, 고혈압과 더불어 콩팥병 유병률이 증
가할 것으로 예상되는 가운데 대한신장학회에서 2006년부터 만성 신부전(chronic renal failure)이라는 진단명 대신 만성 콩팥병(chronic kidney disease)을 사용하도록 권고하였다. 이는 일반인의 신장질환 에 대한 인식을 변화시켜 질병을 조기에 발견하여 신기능 저하의 진 행을 예방하고자 하는 것이다.2-4)
Original Article
한국 성인 남녀에서 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율과 만성 콩팥병 유병률의 관련성:
제5차 국민건강영양조사
이혜경, 심경원*, 이홍수, 이상화, 전혜진, 변아리, 김정화, 노향란
이화여자대학교 의과대학 이대목동병원 가정의학교실
The Relationship of the Triglyceride to High Density Lipoprotein Cholesterol Ratio with the Prevalence of Chronic Kidney Disease in Korean Adults: The Fifth Korean National Health and Nutrition Examination Survey
Hea Kyung Lee, Kyung Won Shim*, Hong Soo Lee, Sang Wha Lee, Hyejin Chun, A Ri Byun, Jung Hwa Kim, Hyang Ran Rho
Department of Family Medicine, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, KoreaBackground: This study aimed to determine the relationship between the triglyceride (TG) to high density lipoprotein cholesterol (HDL-C) ratio and the prevalence of chronic kidney disease in Koreans.
Methods: This cross-sectional study is based on 4,925 subjects who participated in the 5th Korea National Health and Nutrition Examination Survey.
Chronic kidney disease was defined as estimated glomerular filtration rate <60 mL/min/1.73 m
2, calculated by the Modification of Diet in Renal Disease equation, which is 1.863×(serum creatinine
-1.154)×(age
-0.203)×0.742 (if female). The TG/HDL-C ratio was divided equally into quartiles and the prevalence of chronic kidney disease was analyzed based on the quartiles.
Results: The results showed a positive correlation between an increasing tendency of the odds ratio (OR) for the prevalence rate of chronic kidney disease (95% confidence interval) and an increase in the TG/HDL-C ratio in an unadjusted model for Korean adults (P for trend<0.001). For men, the OR did not tend to increase. However, in women, the tendency for an increased prevalence rate of chronic kidney disease was clear, even with adjustment for external factors such as age, waist circumference, hypertension, diabetes mellitus, smoking, drinking, and routine activities (P for trend<0.05).
Conclusion: These findings indicate that the TG/HDL-C ratio is significantly associated with the prevalence of chronic kidney disease in Korean women (P<0.05).
Keywords: Koreans; Chronic Kidney Diseases; Dyslipidemia; Women
http://dx.doi.org/10.21215/kjfp.2016.6.3.191 pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2016;6(3):191-198KJFP
Korean Journal of Family PracticeReceived February 17, 2016 Accepted March 31, 2016 Corresponding author Kyung Won Shim
Tel: +82-2-2650-5165, Fax: +82-2-2654-2439 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Hea Kyung Lee, et al. TG/HDL-C Ratio with the Prevalence of Chronic Kidney Disease
Korean Journal of Family Practice
KJFP
지질 단백질 대사장애가 만성 콩팥병의 원인으로서 가능성이 제 기되고 있으며5,6) 만성 콩팥병 stage 3에서는 중성지방(triglycerides, TG) 상승 및 고밀도 지단백 콜레스테롤(high density lipoprotein cho- lesterol, HDL-C)이 감소하는 경향이 있다.5-8) 즉, 만성 콩팥병 환자에 서 혈중 apolipoprotein A-1, HDL-C 수치가 낮아지고 초 저밀도 지단 백 콜레스테롤(very low-density lipoprotein cholesterol)과 chylomi- crons의 분해가 억제되며 산화 스트레스로 저밀도 지단백 콜레스테 롤(low-density lipoprotein cholesterol, LDL-C)을 포함한 지단백을 산 화시킴으로써 만성 콩팥병에서 기인하는 이상지질혈증이 발생한 다.9) 이미 HDL-C에 대한 TG의 비율과 인슐린 저항성 및 동맥경화증 의 관련성은 밝혀져 있으며10,11) 최근 HDL-C에 대한 TG의 비율이 다 른 지질단백질 수치, 즉 LDL-C, TG 수치보다 심혈관질환 발생률 예 측에 효과적이라는 논문들이 발표되었다.12,13) 그러나 2013 American College of Cardiology/American Heart Association (ACC/AHA) Guide- line on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults에서는 투석을 하는 말기 신장 질환자 에서 statin 치료에 대한 근거가 아직 부족하며 앞으로 추가적인 연구 가 필요하여14) 적극적 치료를 유보하였다.
이번 연구의 목적은 한국 성인 남녀를 대상으로 HDL-C에 대한 TG의 비율이 만성 콩팥병 유병률 증가에 대한 독립적 위험요인인지 를 확인해 보고자 한다.
방 법
1. 연구대상
제5기(2010–2012년) 국민건강영양조사(Korean National Health and Nutrition Examination Survey, KNHANES)를 이용하였고 이는 단면연구로 192개 표본 조사구를 추출하여 3,800가구의 만 1세 이상 가구원 전체를 대상으로 하였으며 대한민국에 거주하는 국민으로 양로원, 군대, 교도소 등에 입소한 자와 외국인 등은 제외되었다.
이번 연구는 제5기 KNHANES에서 성인(만 19세 이상) 남녀 중 건 강설문조사, 검진조사, 영양조사로 나누어 시행된 조사에 모두 참여 한 인원만을 대상으로 하였다. KNHANES의 건강 설문조사, 검진조 사, 영양조사에 모두 참여한 인원은 6,801명이었으며 이 중에서 19세 이상 인구는 5,272명이었다. 분석의 핵심변수인 HDL-C와 TG의 값 이 없는 결측자 347명을 제외하고 총 4,925명을 대상으로 하였다.
2. 연구내용 및 방법
건강설문조사의 교육 및 경제활동, 이환, 의료이용 항목, 영양조사 의 전체항목은 면접방법으로 조사하였고, 건강설문조사 항목 중 흡
연, 음주 등 건강행태영역은 자기기입식으로 조사하였다. 검진조사 는 신체계측, 혈압 및 맥박 측정, 혈액 검사가 포함되며 직접 계측, 관 찰, 검체 분석 등의 방법으로 수행하였다.
채혈은 지질 단백질 수치의 정확성을 위하여 최소 8시간 이상의 금식을 유지하여 시행하였고 채혈 후 이동검진차량에서 전처리 후 검사 결과의 재현성(정밀도) 및 정확성(참값 근접성)을 위해 모든 검체 를 중앙분석실로 운송하여 검체 채취 후 24시간 안에 분석하였다. 소 변의 채취는 소변 컵을 주어 중간 요를 20–30 mL 정도의 임의 요(ran- dom urine)를 받았으며 가능하면 아침 첫 요를 채취하도록 하였다.
3. 만성 콩팥병, 당뇨, 고혈압, 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율의 정의
만성 콩팥병은 Kidney Disease: Improving Global Outcomes (KDI- GO) 2012 Guideline을 바탕으로 estimated glomerular filtration rate (eGFR) 60 mL/min/1.73 m2 미만으로 정의하였으며 eGFR은 Modifica- tion of Diet in Renal Disease (MDRD) equation: 1.863×(serum creatinine-1.154)×(age-0.203)×0.742 (if female)로 계산하였다. 고혈압은 Joint National Committee 8 High Blood Pressure Guideline에 따라 수축기/
이완기 140/90 mmHg 이상 또는 건강설문조사에서 유병력이 있거나 현재 유병인 경우로 정의하였으며, 당뇨병은 2015 American Diabetes Association (ADA) Diabetes Guidelines에 따라 공복혈당(fasting plas- ma glucose, FPG) 126 mg/dL 이상 또는 유병력이 있거나 현재 유병인 경우로 정의하였다. 흡연은 과거 혹은 현재 흡연인 경우로 하였으며 음주는 월 1회 이상 음주하는 경우로, 신체활동은 1주에 중증도 신 체활동 30분 이상씩 5일 이상 또는 격렬한 신체활동 20분 이상씩 3일 이상으로 각각 정의하였다.
HDL-C에 대한 TG의 비율은 TG를 HDL-C로 나누었으며 참여자 를 인원수로 균등 분배하여 HDL-C에 대한 TG 비율의 각 4분위 수 치로 정하였다. 즉 전체에서 HDL-C에 대한 TG의 비율 4분위는 Q1
<1.314 (1,229명), Q2 1.314–2.150 (1,233명), Q3 2.150–3.567 (1,231명), Q4
>3.567 (1,232명)로 나누었으며 남성에서는 Q1 <1.667 (491명), Q2 1.667–2.593 (491명), Q3 2.593–4.288 (492명), Q4 >4.288 (492명) 수치를 기준으로 4분위 하였다. 여성에서는 HDL-C에 대한 TG의 비율을 Q1 <1.165 (739명), Q2 1.165–1.879 (740명), Q3 1.879–3.098 (740명), Q4
>3.098 (740명)로 4분위 수치를 정하였다.
4. 통계분석
모든 분석은 SAS ver. 9.4 (SAS Institute, Cary, NC, USA)를 이용하였 으며 유의성은 P<0.05로 정하였다. 임상적 특징을 비교하기 위하여 연속형 변수는 mean±standard error of mean, 범주형 변수는 n (%)으
이혜경 외. TG/HDL-C 비율과 만성 콩팥병 유병률의 관련성 Korean Journal of Family Practice
KJFP
로 기재하였으며 그룹 간 차이 검정은 연속형 변수는 simple linear regression, 범주형 변수는 Rao-Scott chi-square test 방법을 이용하였 다. 그리고 HDL-C에 대한 TG의 비율에 따른 각 4분위 그룹과 만성 콩팥병 유병률 간의 연관성 분석은 survey logistic regression 이용하 였다. 만성 콩팥병의 위험 요인인 나이, 고혈압, 당뇨, 산화스트레스,
비만15,16)을 보정하기 위하여 나이, 고혈압, 당뇨, 흡연, 음주, 운동, 허
리둘레(waist circumference, WC)를 혼란변수로 설정하였다. 혼란변 수 중 비만의 평가 지표로 신체질량지수(body mass index, BMI)가 아 닌 심혈관 질환 위험도 평가에 예민한 WC를 선택하였다.17)
결 과
1. 일반사항
Table 1에서 남자 1,966명(40.0%), 여자 2,959명(60.0%)으로 구성된 4,925명의 연구대상자에 대한 임상적, 역학적 특징을 제시하였다. 평 균 연령은 남자 45.62±0.5세, 여자 46.69±0.47세였고 TG는 남성에서 148.80±2.93 mg/dL로 여자보다 유의하게(P<0.001) 높았으며 HDL-C 는 47.56±0.36 mg/dL로 남성이 여성보다 유의하게(P<0.001) 낮았다.
eGFR은 여성이 96.47±0.53 mL/min/1.73 m2으로 남성보다 유의하게 (P<0.001) 높았으며 흡연율 및 음주율은 남성과 여성에서 의미 있는 (각각 P<0.001) 차이가 있었다. LDL-C, 총 콜레스테롤, HbA1c, 만성 콩 팥병 유병률, 당뇨병 유병률은 남녀에서 유의한 차이가 없었다.
Table 1. Baseline characteristics of the study subjects (n=4,925)
Characteristic Men Women P-value†
Participants 1,966 (40.0) 2,959 (60.0)
Age (y) 45.62±0.50 46.69±0.47 0.047*
BMI (kg/m2) 24.12±0.11 23.41±0.12 <0.001*
WC (cm) 83.93±0.31 78.12±0.34 <0.001*
SBP (mmHg) 120.30±0.48 115.58±0.53 <0.001*
DBP (mmHg) 78.46±0.37 73.52±0.28 <0.001*
FPG (mg/dL) 98.58±0.54 96.50±0.64 0.006*
TG (mg/dL) 148.80±2.93 116.58±3.05 <0.001*
HDL-C (mg/dL) 47.56±0.36 52.82±0.32 <0.001*
LDL-C (mg/dL) 114.19±0.94 114.80±0.77 0.627
Cholesterol (mg/dL) 188.10±1.11 189.60±0.94 0.291
HbA1c (%) 5.69 5.71 0.479
Creatinine (mg/dL) 0.98±0.00 0.73±0.00 <0.001* eGFR (mL/min/1.73 m2) 91.87±0.48 96.47±0.53 <0.001*
CKD‡ 91 (2.7) 108 (3.3) 0.239
Hypertension 718 (30.8) 887 (25.5) 0.002*
Diabetes mellitus 259 (9.5) 259 (7.9) 0.072
Smoking 1,489 (77.9) 265 (12.3) <0.001*
Alcohol 1,295 (73.2) 1,014 (39.4) <0.001*
Regular exercise 363 (21.5) 385 (13.5) <0.001* Values are presented as number (%) or mean±standard deviation.
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure;
DBP, diastolic blood pressure; FPG, fasting plasma glucose; TG, triglycerides;
HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cho- lesterol; eGFR, estimated glomerular filtration rate, CKD, chronic kidney disease.
*P<0.05. †This was calculated by simple linear regression and Rao-Scott chi- square test that were used for the analysis of continuous and categorical vari- ables, respectively. ‡From Modification of Diet in Renal Disease equation: 186.3×
(serum creatinine-1.154)×(age-0.203)×0.742 (if female), eGFR of < 60 mL/min/1.73 m2 and/or the presence of proteinuria (defined as urinary protein ≥1+ on dip- stick testing).
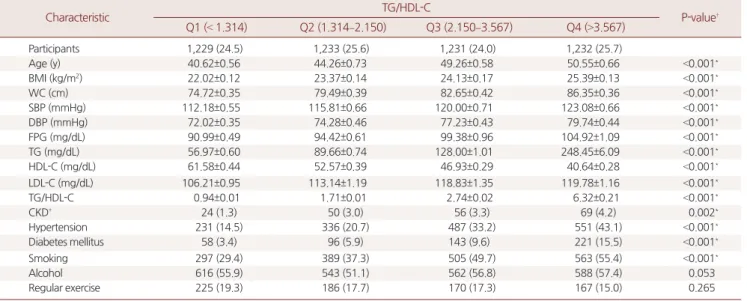
Table 2. Mean values or frequencies of relevant factors according to the quartiles of TG/HDL-C
Characteristic TG/HDL-C
P-value† Q1 (< 1.314) Q2 (1.314–2.150) Q3 (2.150–3.567) Q4 (>3.567)
Participants 1,229 (24.5) 1,233 (25.6) 1,231 (24.0) 1,232 (25.7)
Age (y) 40.62±0.56 44.26±0.73 49.26±0.58 50.55±0.66 <0.001*
BMI (kg/m2) 22.02±0.12 23.37±0.14 24.13±0.17 25.39±0.13 <0.001*
WC (cm) 74.72±0.35 79.49±0.39 82.65±0.42 86.35±0.36 <0.001*
SBP (mmHg) 112.18±0.55 115.81±0.66 120.00±0.71 123.08±0.66 <0.001*
DBP (mmHg) 72.02±0.35 74.28±0.46 77.23±0.43 79.74±0.44 <0.001*
FPG (mg/dL) 90.99±0.49 94.42±0.61 99.38±0.96 104.92±1.09 <0.001*
TG (mg/dL) 56.97±0.60 89.66±0.74 128.00±1.01 248.45±6.09 <0.001*
HDL-C (mg/dL) 61.58±0.44 52.57±0.39 46.93±0.29 40.64±0.28 <0.001*
LDL-C (mg/dL) 106.21±0.95 113.14±1.19 118.83±1.35 119.78±1.16 <0.001*
TG/HDL-C 0.94±0.01 1.71±0.01 2.74±0.02 6.32±0.21 <0.001*
CKD‡ 24 (1.3) 50 (3.0) 56 (3.3) 69 (4.2) 0.002*
Hypertension 231 (14.5) 336 (20.7) 487 (33.2) 551 (43.1) <0.001*
Diabetes mellitus 58 (3.4) 96 (5.9) 143 (9.6) 221 (15.5) <0.001*
Smoking 297 (29.4) 389 (37.3) 505 (49.7) 563 (55.4) <0.001*
Alcohol 616 (55.9) 543 (51.1) 562 (56.8) 588 (57.4) 0.053
Regular exercise 225 (19.3) 186 (17.7) 170 (17.3) 167 (15.0) 0.265
Values are presented as number (%) or mean±standard deviation.
TG, triglycerides; HDL-C, high density lipoprotein cholesterol; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pres- sure; FPG, fasting plasma glucose; LDL-C, low density lipoprotein cholesterol; CKD, chronic kidney disease.
*P<0.05. †This was calculated by simple linear regression and Rao-Scott chi-square test that were used for the analysis of continuous and categorical variables, respec- tively. ‡From Modification of Diet in Renal Disease equation: 186.3×(serum creatinine-1.154)×(age-0.203)×0.742 (if female), estimated glomerular filtration rate of <60 mL/
min/1.73 m2 and/or the presence of proteinuria (defined as urinary protein ≥1+ on dipstick testing).
Hea Kyung Lee, et al. TG/HDL-C Ratio with the Prevalence of Chronic Kidney Disease
Korean Journal of Family Practice
KJFP
2. 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율에 따른 4분위 그룹
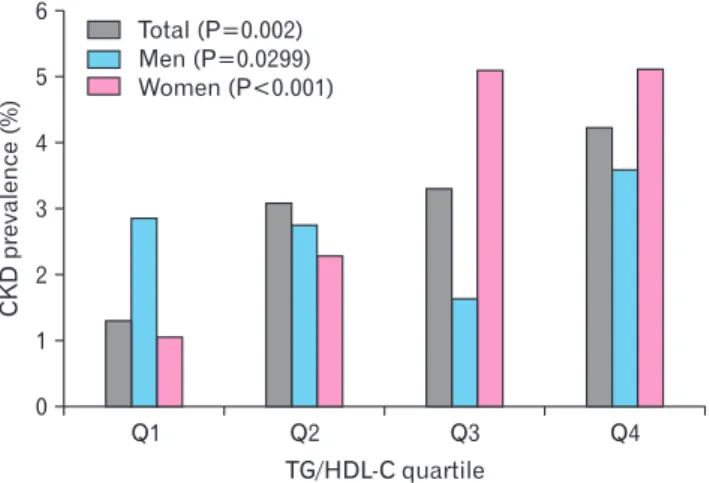
Table 2는 남녀 전체를 HDL-C에 대한 TG의 비율을 기준으로 네 그룹으로 나누어 임상적, 역학적 특징을 보았다. HDL-C에 대한 TG 의 비율이 증가할수록 나이(age), BMI, WC, 수축기 혈압, 이완기 혈압, FPG, TG, LDL-C가 유의하게(모두 P<0.001) 증가하였다. 만성 콩팥병 의 유병률은 HDL-C에 대한 TG의 비율이 증가할수록 유의하게 (P=0.002) 증가하였으며 이는 Figure 1에서도 의미 있는 증가 경향을 확인할 수 있었다. Table 3은 남녀 전체에서 HDL-C에 대한 TG의 비 율이 증가함에 따른 만성 콩팥병 유병률 odd ratio (OR) (95% confi- dence interval [CI]) 값을 survey logistic regression 이용하여 분석하였
다. Unadjusted 모델에서 만성 콩팥병 유병률의 OR이 순차적으로 증 가하는 경향(P for trend<0.001)으로 HDL-C에 대한 TG의 비율이 가 장 높은 군에서 만성 콩팥병 유병률이 3.35배(95% CI, 1.88–5.97) 증가 하는 것으로 확인되었다. 하지만 나이를 보정한 Model 1과 고혈압, 당 뇨, WC, 흡연, 음주, 신체활동을 보정한 Model 2 각각에서는 유의한 차이가 없었다.
3. 남녀 각각에서 본 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율에 따른 4분위 그룹
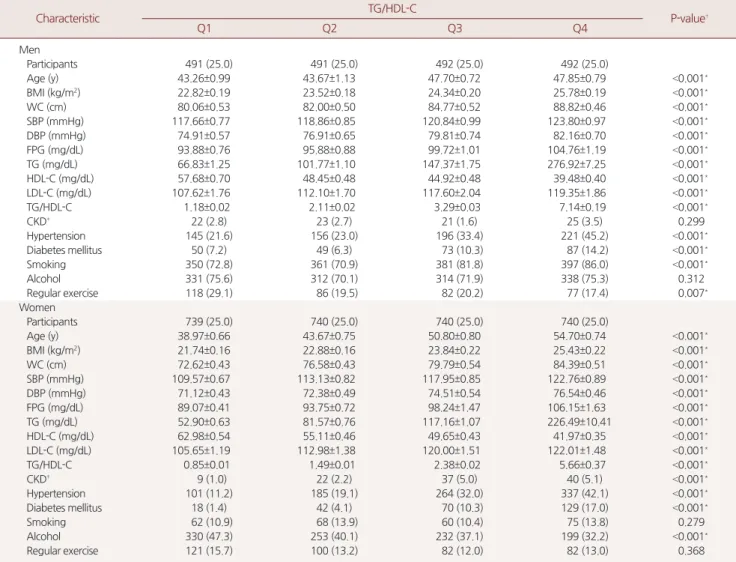
추가적으로 남녀를 각각 나누어 HDL-C에 대한 TG의 비율이 증 가함에 따른 임상적, 역학적 특징을 보았다. Table 4에서 보면 남성에 서 HDL-C에 대한 TG의 비율이 증가함에 따라 나이, BMI, WC, 수축 기 혈압, 이완기 혈압, FPG, TG, LDL-C가 유의하게(모두 P<0.001) 증 가하였다. 여성의 경우도 HDL-C에 대한 TG의 비율이 증가함에 따 라 나이, BMI, WC, 수축기 혈압, 이완기 혈압, FPG, TG, LDL-C가 유 의하게(모두 P<0.001) 증가하였다. 만성 콩팥병 유병률의 경우에는 여성에서만 HDL-C에 대한 TG의 비율이 증가할수록 유의하게 증가 하였다(P<0.001).
Table 5는 남녀 각각에서 HDL-C에 대한 TG의 비율이 증가함에 따른 만성 콩팥병 유병률을 survey logistic regression 이용하여 그 OR (95% CI) 값을 분석한 것으로 남성의 경우 모든 Model에서 HDL-C에 대한 TG의 비율 상승에 따른 만성 콩팥병 유병률 OR이 의미 있는 차이를 보이지 않았다. 그러나 여성의 경우 만성 콩팥병의 위험 OR 값이 3분위에서 5.00배(95% CI, 2.14–11.70), 4분위에서 5.03배(95% CI, 2.13–11.87)로 순차적으로 높아짐을 확인하였다(P for trend<0.05).
고 찰
이번 연구에서 우리는 HDL-C에 대한 TG의 비율이 만성 콩팥병 발생의 독립적 위험 요인일 수 있다는 가정하에 19세 이상의 한국 성 인 남녀를 대상으로 HDL-C에 대한 TG의 비율 상승에 따른 만성 콩
Table 3. Multivariate adjusted odds ratio and 95% confidence interval for the CKD according to the quartiles of TG/HDL-C
Total TG/HDL-C
P for trend† Q1 (< 1.314) Q2 (1.314–2.150) Q3 (2.150–3.567) Q4 (>3.567)
Unadjusted odds ratio Reference 2.41 (1.36 –4.29)* 2.58 (1.40–4.76)* 3.35 (1.88–5.97)* <0.001*
Model 1 1.91 (1.07–3.43)* 1.60 (0.85–3.04) 2.11 (1.15–3.87)* 0.054
Model 2 1.99 (1.07–3.68)* 1.88 (0.94–3.76) 1.75 (0.88–3.49) 0.325
Model 1: adjusted for age. Model 2: adjusted for waist circumstance, hypertension, diabetes, smoking, alcohol, regular exercise habit.
CKD, chronic kidney disease; TG, triglycerides; HDL-C, high density lipoprotein cholesterol.
*P<0.05. †This was calculated by survey logistic procedure.
Q1 Q2 Q3 Q4
6 5 4 3 2 1
CKDprevalence(%)
TG/HDL-C quartile 0
Total (P=0.002) Men (P=0.0299) Women (P<0.001)
Figure 1. The prevalence of CKD in participants with different TG/HDL- C. TG/HDL-C ratio was divided into quartiles in men and women, men, women and prevalence of chronic kidney disease was analyzed based on quartiles of TG/HDL-C ratio. P-value was calculated by simple linear regression and Rao-Scott chi-square test that were used for the analysis of continuous and categorical variables, respectively. Total: Q1
<1.314 (n=1,229), Q2 1.314–2.150 (n=1,233), Q3 2.150–3.567 (n=1,231), Q4 >3.567 (n=1,232); Men: Q1 <1.667 (n=491), Q2 1.667–2.593 (n=491), Q3 2.593–4.288 (n=492), Q4 >4.288 (n=492);
Women: Q1 <1.165 (n=739), Q2 1.165–1.879 (n=740), Q3 1.879–
3.098 (n=740), Q4 >3.098 (n=740). CKD, chronic kidney disease; TG, triglycerides; HDL-C, high density lipoprotein cholesterol.
이혜경 외. TG/HDL-C 비율과 만성 콩팥병 유병률의 관련성 Korean Journal of Family Practice
KJFP
Table 4. Mean values or frequencies of relevant factors according to the quartiles of TG/HDL-C both men and women respectively
Characteristic TG/HDL-C
P-value†
Q1 Q2 Q3 Q4
Men
Participants 491 (25.0) 491 (25.0) 492 (25.0) 492 (25.0)
Age (y) 43.26±0.99 43.67±1.13 47.70±0.72 47.85±0.79 <0.001*
BMI (kg/m2) 22.82±0.19 23.52±0.18 24.34±0.20 25.78±0.19 <0.001*
WC (cm) 80.06±0.53 82.00±0.50 84.77±0.52 88.82±0.46 <0.001*
SBP (mmHg) 117.66±0.77 118.86±0.85 120.84±0.99 123.80±0.97 <0.001*
DBP (mmHg) 74.91±0.57 76.91±0.65 79.81±0.74 82.16±0.70 <0.001*
FPG (mg/dL) 93.88±0.76 95.88±0.88 99.72±1.01 104.76±1.19 <0.001*
TG (mg/dL) 66.83±1.25 101.77±1.10 147.37±1.75 276.92±7.25 <0.001*
HDL-C (mg/dL) 57.68±0.70 48.45±0.48 44.92±0.48 39.48±0.40 <0.001*
LDL-C (mg/dL) 107.62±1.76 112.10±1.70 117.60±2.04 119.35±1.86 <0.001*
TG/HDL-C 1.18±0.02 2.11±0.02 3.29±0.03 7.14±0.19 <0.001*
CKD‡ 22 (2.8) 23 (2.7) 21 (1.6) 25 (3.5) 0.299
Hypertension 145 (21.6) 156 (23.0) 196 (33.4) 221 (45.2) <0.001*
Diabetes mellitus 50 (7.2) 49 (6.3) 73 (10.3) 87 (14.2) <0.001*
Smoking 350 (72.8) 361 (70.9) 381 (81.8) 397 (86.0) <0.001*
Alcohol 331 (75.6) 312 (70.1) 314 (71.9) 338 (75.3) 0.312
Regular exercise 118 (29.1) 86 (19.5) 82 (20.2) 77 (17.4) 0.007*
Women
Participants 739 (25.0) 740 (25.0) 740 (25.0) 740 (25.0)
Age (y) 38.97±0.66 43.67±0.75 50.80±0.80 54.70±0.74 <0.001*
BMI (kg/m2) 21.74±0.16 22.88±0.16 23.84±0.22 25.43±0.22 <0.001*
WC (cm) 72.62±0.43 76.58±0.43 79.79±0.54 84.39±0.51 <0.001*
SBP (mmHg) 109.57±0.67 113.13±0.82 117.95±0.85 122.76±0.89 <0.001*
DBP (mmHg) 71.12±0.43 72.38±0.49 74.51±0.54 76.54±0.46 <0.001*
FPG (mg/dL) 89.07±0.41 93.75±0.72 98.24±1.47 106.15±1.63 <0.001*
TG (mg/dL) 52.90±0.63 81.57±0.76 117.16±1.07 226.49±10.41 <0.001*
HDL-C (mg/dL) 62.98±0.54 55.11±0.46 49.65±0.43 41.97±0.35 <0.001*
LDL-C (mg/dL) 105.65±1.19 112.98±1.38 120.00±1.51 122.01±1.48 <0.001*
TG/HDL-C 0.85±0.01 1.49±0.01 2.38±0.02 5.66±0.37 <0.001*
CKD‡ 9 (1.0) 22 (2.2) 37 (5.0) 40 (5.1) <0.001*
Hypertension 101 (11.2) 185 (19.1) 264 (32.0) 337 (42.1) <0.001*
Diabetes mellitus 18 (1.4) 42 (4.1) 70 (10.3) 129 (17.0) <0.001*
Smoking 62 (10.9) 68 (13.9) 60 (10.4) 75 (13.8) 0.279
Alcohol 330 (47.3) 253 (40.1) 232 (37.1) 199 (32.2) <0.001*
Regular exercise 121 (15.7) 100 (13.2) 82 (12.0) 82 (13.0) 0.368
Values are presented as number (%) or mean±standard deviation. Men: Q1 <1.667, Q2 1.667–2.593, Q3 2.593–4.288, Q4 >4.288; Women: Q1 <1.165, Q2 1.165–
1.879, Q3 1.879–3.098, Q4 >3.098.
TG, triglycerides; HDL-C, high density lipoprotein cholesterol; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pres- sure; FPG, fasting plasma glucose; LDL-C, low density lipoprotein cholesterol; CKD, chronic kidney disease.
*P<0.05. †This was calculated by simple linear regression and Rao-Scott chi-square test that were used for the analysis of continuous and categorical variables, respec- tively. ‡From Modification of Diet in Renal Disease equation: 186.3×(serum creatinine-1.154)×(age-0.203)×0.742 (if female), estimated glomerular filtration rate of <60 mL/
min/1.73 m2 and/or the presence of proteinuria (defined as urinary protein ≥1+ on dipstick testing).
Table 5. Multivariate adjusted odds ratio and 95% confidence interval for the CKD according to the quartiles of TG/HDL-C both men and women respectively
Characteristic TG/HDL-C
P for trend†
Q1 Q2 Q3 Q4
Men
Unadjusted odds ratio Reference 0.96 (0.43–2.12) 0.57 (0.28–1.17) 1.27 (0.61–2.61) 0.750
Model 1 0.99 (0.44–2.25) 0.58 (0.29–1.16) 1.46 (0.71–3.02) 0.514
Model 2 0.69 (0.29–1.63) 0.36 (0.14–0.92)* 0.51 (0.19–1.35) 0.142
Women
Unadjusted odds ratio Reference 2.17 (0.84–5.55) 5.00 (2.14–11.70)* 5.03 (2.13–11.87)* <0.001*
Model 1 1.67 (0.63–4.44) 2.63 (1.01–6.83)* 2.33 (0.90–6.06) 0.045*
Model 2 2.40 (0.83–6.96) 3.83 (1.47–10.02)* 3.05 (1.10–8.47)* 0.014*
Men: Q1 <1.667, Q2 1.667–2.593, Q3 2.593–4.288, Q4 >4.288; Women: Q1 <1.165, Q2 1.165–1.879, Q3 1.879–3.098, Q4 >3.098. Model 1: adjusted for age.
Model 2: adjusted for waist circumstance, hypertension, diabetes, smoking, alcohol, regular exercise habit.
CKD, chronic kidney disease; TG, triglycerides; HDL-C, high density lipoprotein cholesterol.
*P<0.05. †This was calculated by survey logistic procedure.
Hea Kyung Lee, et al. TG/HDL-C Ratio with the Prevalence of Chronic Kidney Disease
Korean Journal of Family Practice
KJFP
팥병 유병률을 확인해 보았다. 그 결과는 여성에서만 HDL-C에 대한 TG의 비율 상승 시 만성 콩팥병 유병률이 약 2–5배 유의하게 증가한 다는 것을 확인하였다(P for trend<0.05).
만성 콩팥병과 이상지질혈증의 선후관계에 대해서는 아직 논란
중이다.18-20) 만성 콩팥병 환자에서 질병 자체가 지질대사이상을 유도
한다는 것이 일반적으로 알려진 이론이었으나 최근에는 지질대사 이상 자체가 콩팥병 진행을 야기한다는 논문도 발표되었다.21,22) 만 성 콩팥병의 위험요인은 심혈관 질환(cardiovascular disease)의 위험 요인인 고혈압, 당뇨, 만성 염증, 산화 스트레스, 비만을 공유한다.23) 이는 사구체 혈관사이세포(glomerular mesangial cell)와 혈관 평활근 세포(vascular smooth muscle cell)의 분자적 구조가 비슷하기 때문에 동일한 위험 요인에 의해 사구체 경화증(glomerulosclerosis)과 죽상 동맥경화(atherosclerosis)가 진행되는 것으로 보인다.23-25) 한편 HDL-C 에 대한 TG의 비율 증가는 LDL-C의 구성성분인 small dense LDL-C particles 증가와 관련이 있다.26) 이 small dense LDL-C는 인슐린 저항 성과 상관관계가 있으며10,13) 인슐린 저항성은 당뇨병이 없는 사람에 서 신장기능이상의 진행에 위험요인으로 작용한다.27) 또한 당뇨가 없으며 과체중인 사람에서 HDL-C에 대한 TG의 비율이 인슐린 저 항성을 반영한다는 것이 알려져 있다.10) 따라서 HDL-C에 대한 TG의 비율 증가는 만성 콩팥병의 위험요인이 될 수 있는 것으로 해석할 수 있다.
Kang 등23)은 2005년 KNHNES 자료를 이용하여 남녀를 구분하지 않고 19세 이상의 성인을 대상으로 HDL-C에 대한 TG의 비율이 증 가할수록 만성 콩팥병의 유병률이 유의하게(P<0.05) 증가함을 확인 하였다. 기존 연구와 다르게 이번 연구는 남녀를 각각 나누어 HDL-C에 대한 TG의 비율 증가에 따른 만성 콩팥병 유병률을 확인 하였으며 여성에서만 의미 있는 결과를 보였다. Kim 등28)은 2007–
2008년 KNHNES 자료로 총콜레스테롤/HDL-C, TG/HDL-C, LDL- C/HDL-C, 비HDL-C/HDL-C 중 오직 HDL-C에 대한 TG의 비율이 남녀 모두에서 만성 콩팥병 유병률과의 관련성을 확인하였다. 이번 연구에서는 혼란변수인 비만의 지표로 WC만 보정하였으나 Kim 등28) 은 BMI와 WC를 모두 보정하였다. 또한 남성에서도 유의한 관련성을 보였다는 점에서 본 연구와 차이를 보였다. Tsuruya 등29)은 일본의 20 세 이상 성인 216,007명을 대상으로 남녀를 각각 나누어 HDL-C에 대한 TG의 비율이 증가함에 따라 eGFR이 감소하고, 만성 콩팥병 유 병률과 dipstick test로 확인한 단백뇨(urinary protein ≥1+)의 빈도가 유의하게(모두 P<0.001) 증가함을 확인하였다. 이 연구에서는 뇌졸 중 과거력, 심장질환, 이상지질혈증 약물 복용 중인 자를 혼란변수로 고려하였다는 점에서 본 연구와 연구대상자 및 방법 설정에 차이점 이 있다.
앞에서 언급하였듯 HDL-C에 대한 TG의 비율 상승이 인슐린 저 항성과 관련이 있으며 인슐린 저항성에 영향을 주는 HDL-C에 대한 TG 비율의 cut off points 확인을 위한 연구들이 있다. Mostafa 등30)은 대상을 인종 별로 나누었으며 백인 남성, 백인 여성에서 각각 3.8과 2.0 (TG/HDL-C), 남아시아인(India, Pakistani, Bangladeshi)에서 남성 은 2.8, 여성은 2.5로 HDL-C에 대한 TG 비율의 cut off points를 각각 정하였다. McLaughlin 등10)은 BMI 25 kg/m2 이상인 사람을 대상으로 인슐린 저항성에 영향을 주는 HDL-C에 대한 TG 비율의 cut off point로 3.0 (TG/HDL-C)을 제시하였다. 이처럼 아직 임상적으로 통 용할 만큼의 정확한 HDL-C에 대한 TG의 비율의 cut off points가 정 해지지 않았으므로 이번 논문에서는 HDL-C에 대한 TG의 비율을 나눈 기준을 참여자 인원의 균등 분배로 정하였다. 이러한 이유로 본 연구에서 남성의 HDL-C에 대한 TG의 비율과 만성 콩팥병 유병 률이 연관성 없게 나온 것으로 보인다. Table 5에서 남성의 OR 값 추 이를 보면 이전 연구에서 제시한 HDL-C에 대한 TG의 비율 cut off points인 2.8과 3.0 (TG/HDL-C)이 속한 Q3을 기준으로 U자 모양을 확인할 수 있다.
Table 5에서 여성 Model 1, 2의 OR 값 추이를 보면 P for trend<0.05 이나 Q4에서 Q3보다 감소하는 경향을 보이며 이는 여성의 HDL-C 에 대한 TG의 비율 cut off points가 Q3에 속해 있으며 비만 혼란변수 로 BMI를 포함하지 않아서 오는 결과로 보인다. 또한 Tsuruya 등29)의 연구와 비교하였을 때 본 연구의 Q3 범위가 넓게 설정되었으며 4분 위 기준 수치가 다른 데서 오는 차이로 보인다.
이번 연구의 제한점은 첫째, HDL-C 및 TG 혈중 수치에 영향을 줄 수 있는 이상지질혈증 약물 복용자를 고려하지 않고 만성 콩팥병 유 병률 OR 값을 확인하였다는 점에서 선택편의를 배제할 수 없었다.
둘째, KNHANES 조사의 특성상 방문 검사를 하므로 아침 첫 소변 으로 채취할 수 없었다는 한계가 있으며 셋째, 이번 연구는 단면연구 로 HDL-C에 대한 TG의 비율 상승에 따른 만성 콩팥병 유병률 선후 관계를 밝히기 어렵다는 점이다. 그러나 이 연구는 전국민을 목표 모 집단으로 한 대규모 연구이며 계층별 표준화 집락 추출을 통한 제5 기 KNHANES를 이용하여 분석한 것으로 그 결과를 일반화할 수 있 다는 장점이 있다. 또한 다른 인종을 대상으로 한 기존 연구에 비해 우리나라 사람들을 대상으로 하여 한국인에서도 기존 연구와 같은 경향의 결론을 다시 한번 확인하였다는 점에 임상적 의의가 있다. 앞 으로 대규모 코호트 연구를 통하여 이상지질혈증과 만성 콩팥병의 선후관계를 확인하고 최적의 HDL-C에 대한 TG의 비율 cut off point 를 찾는 추가 연구가 동반되어야 할 것이다.
이혜경 외. TG/HDL-C 비율과 만성 콩팥병 유병률의 관련성 Korean Journal of Family Practice
KJFP
요 약
연구배경:
지질 단백질 대사장애가 만성 콩팥병의 원인으로서 가 능성이 제기되고 있는 가운데 이번 연구의 목적은 한국 성인 남녀를 대상으로 이상지질혈증의 지표인 고밀도 지단백 콜레스테롤에 대 한 중성지방의 비율과 만성 콩팥병 유병률의 연관성에 대해 알아보 고자 한다.방법:
제5기(2010–2012년) 국민건강영양조사에 참여한 인원 중 4,925명을 대상으로 한 단면연구이다. 만성 콩팥병은 estimated glo- merular filtration rate 60 mL/min/1.73 m2 미만으로 정의하였으며 Modification of Diet in Renal Disease equation: 1.863×(serum creatinine-1.154)×(age-0.203)×0.742 (if female)로 계산하였다. 고밀도 지단 백 콜레스테롤에 대한 중성지방의 비율은 중성지방(mg/dL)을 고밀 도 지단백 콜레스테롤(mg/dL)으로 나누었으며 참여자 수를 기준으 로 균등 분배하여 고밀도 지단백 콜레스테롤에 대한 중성지방 비율 의 4분위 기준 수치를 정하였다.결과:
남녀 전체에서 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율이 증가함에 따른 만성 콩팥병 유병률 odd ratio (OR)와 95%confidence interval 값은 unadjusted 모델에서 고밀도 지단백 콜레스 테롤에 대한 중성지방의 비율이 증가할수록 순차적으로 증가하는 경향을 보였다(P for trend<0.001). 그러나 남성의 경우 모든 모델에서 고밀도 지단백 콜레스테롤에 대한 중성지방의 비율이 증가할수록 만성 콩팥병 유병률 OR이 순차적으로 증가하지 않았다. 반면 여성 의 경우 HDL-C에 대한 TG의 비율 상승 시 만성 콩팥병 유병률이 약 2–5배 유의하게 증가하였다(P for trend<0.05).
결론:
여성에서만 고밀도 지단백 콜레스테롤에 대한 중성지방의 비 율이 상승할수록 만성 콩팥병 유병률이 유의하게 증가하였다 (P<0.05).중심단어:
한국인; 만성콩팥병; 이상지질혈증; 여성 REFERENCES1. Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al.
Blood pressure and end-stage renal disease in men. N Engl J Med 1996; 334:
13-8.
2. James MT, Hemmelgarn BR, Tonelli M. Early recognition and prevention of chronic kidney disease. Lancet 2010; 375: 1296-309.
3. Levey AS, Coresh J. Chronic kidney disease. Lancet 2012; 379: 165-80.
4. El Nahas M. The global challenge of chronic kidney disease. Kidney Int 2005; 68: 2918-29.
5. Ritz E, Wanner C. Lipid changes and statins in chronic renal insufficiency. J
Am Soc Nephrol 2006; 17: S226-30.
6. Vaziri ND. Dyslipidemia of chronic renal failure: the nature, mechanisms, and potential consequences. Am J Physiol Renal Physiol 2006; 290: F262- 72.
7. Shlipak MG, Fried LF, Cushman M, Manolio TA, Peterson D, Stehman- Breen C, et al. Cardiovascular mortality risk in chronic kidney disease: com- parison of traditional and novel risk factors. JAMA 2005; 293: 1737-45.
8. Parikh NI, Hwang SJ, Larson MG, Meigs JB, Levy D, Fox CS. Cardiovascular disease risk factors in chronic kidney disease: overall burden and rates of treatment and control. Arch Intern Med 2006; 166: 1884-91.
9. Vaziri ND, Norris K. Lipid disorders and their relevance to outcomes in chronic kidney disease. Blood Purif 2011; 31: 189-96.
10. McLaughlin T, Abbasi F, Cheal K, Chu J, Lamendola C, Reaven G. Use of metabolic markers to identify overweight individuals who are insulin resis- tant. Ann Intern Med 2003; 139: 802-9.
11. Bittner V, Johnson BD, Zineh I, Rogers WJ, Vido D, Marroquin OC, et al. The triglyceride/high-density lipoprotein cholesterol ratio predicts all-cause mortality in women with suspected myocardial ischemia: a report from the Women's Ischemia Syndrome Evaluation (WISE). Am Heart J 2009; 157:
548-55.
12. Jeppesen J, Hein HO, Suadicani P, Gyntelberg F. Relation of high TG-low HDL cholesterol and LDL cholesterol to the incidence of ischemic heart disease. An 8-year follow-up in the Copenhagen male study. Arterioscler Thromb Vasc Biol 1997; 17: 1114-20.
13. Salazar MR, Carbajal HA, Espeche WG, Leiva Sisnieguez CE, Balbin E, Dul- becco CA, et al. Relation among the plasma triglyceride/high-density lipo- protein cholesterol concentration ratio, insulin resistance, and associated cardio-metabolic risk factors in men and women. Am J Cardiol 2012; 109:
1749-53.
14. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the Amer- ican College of Cardiology/American Heart Association task force on prac- tice guidelines. J Am Coll Cardiol 2014; 63: 2889-934.
15. Yoon YS, Park HS, Yun KE, Kim SB. Obesity and metabolic syndrome-relat- ed chronic kidney disease in nondiabetic, nonhypertensive adults. Metabo- lism 2009; 58: 1737-42.
16. Fox ER, Benjamin EJ, Sarpong DF, Nagarajarao H, Taylor JK, Steffes MW, et al. The relation of C-reactive protein to chronic kidney disease in African Americans: the Jackson heart study. BMC Nephrol 2010; 11: 1.
17. Kramer H, Shoham D, McClure LA, Durazo-Arvizu R, Howard G, Judd S, et al. Association of waist circumference and body mass index with all-cause mortality in CKD: The REGARDS (Reasons for Geographic and Racial Differences in Stroke) study. Am J Kidney Dis 2011; 58: 177-85.
18. Sandhu S, Wiebe N, Fried LF, Tonelli M. Statins for improving renal out- comes: a meta-analysis. J Am Soc Nephrol 2006; 17: 2006-16.
19. Strippoli GF, Navaneethan SD, Johnson DW, Perkovic V, Pellegrini F, Nico- lucci A, et al. Effects of statins in patients with chronic kidney disease: meta- analysis and meta-regression of randomised controlled trials. BMJ 2008;
336: 645-51.
20. Chawla V, Greene T, Beck GJ, Kusek JW, Collins AJ, Sarnak MJ, et al. Hyper- lipidemia and long-term outcomes in nondiabetic chronic kidney disease.
Clin J Am Soc Nephrol 2010; 5: 1582-7.
Hea Kyung Lee, et al. TG/HDL-C Ratio with the Prevalence of Chronic Kidney Disease
Korean Journal of Family Practice
KJFP
21. Schaeffner ES, Kurth T, Curhan GC, Glynn RJ, Rexrode KM, Baigent C, et al.
Cholesterol and the risk of renal dysfunction in apparently healthy men. J Am Soc Nephrol 2003; 14: 2084-91.
22. Chen SC, Hung CC, Kuo MC, Lee JJ, Chiu YW, Chang JM, et al. Association of dyslipidemia with renal outcomes in chronic kidney disease. PLoS One 2013; 8: e55643.
23. Kang HT, Shim JY, Lee YJ, Lee JE, Linton JA, Kim JK, et al. Association be- tween the ratio of triglycerides to high-density lipoprotein cholesterol and chronic kidney disease in Korean adults: the 2005 Korean National Health and Nutrition Examination Survey. Kidney Blood Press Res 2011; 34: 173-9.
24. Klahr S, Schreiner G, Ichikawa I. The progression of renal disease. N Engl J Med 1988; 318: 1657-66.
25. Diamond JR, Karnovsky MJ. Focal and segmental glomerulosclerosis: anal- ogies to atherosclerosis. Kidney Int 1988; 33: 917-24.
26. Boizel R, Benhamou PY, Lardy B, Laporte F, Foulon T, Halimi S. Ratio of tri- glycerides to HDL cholesterol is an indicator of LDL particle size in patients
with type 2 diabetes and normal HDL cholesterol levels. Diabetes Care 2000; 23: 1679-85.
27. Kobayashi H, Tokudome G, Hara Y, Sugano N, Endo S, Suetsugu Y, et al. In- sulin resistance is a risk factor for the progression of chronic kidney disease.
Clin Nephrol 2009; 71: 643-51.
28. Kim JY, Kang HT, Lee HR, Lee YJ, Shim JY. Comparison of lipid-related ra- tios for prediction of chronic kidney disease stage 3 or more in Korean adults. J Korean Med Sci 2012; 27: 1524-9.
29. Tsuruya K, Yoshida H, Nagata M, Kitazono T, Hirakata H, Iseki K, et al. As- sociation of the triglycerides to high-density lipoprotein cholesterol ratio with the risk of chronic kidney disease: analysis in a large Japanese popula- tion. Atherosclerosis 2014; 233: 260-7.
30. Mostafa S, Davies MJ, Morris DH, Yates T, Srinivasan BT, Webb D, et al. The association of the triglyceride-to-HDL cholesterol ratio with insulin resis- tance in White European and South Asian men and women. PLoS One 2012; 7: e50931.