저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게
l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다:
l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다.
l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다.
저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다.
Disclaimer
저작자표시. 귀하는 원저작자를 표시하여야 합니다.
비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다.
변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
의학석사 학위논문
The effect of systemic steroid on hearing preservation after cochlear implantation via round window approach: A guinea pig model
정원창 접근법을 이용한 와우이식에서의 전신적 스테로이드의 청력 보존 효과:
기니픽 모델
2016년 1월
서울대학교 대학원 의학과 이비인후과전공
장 문 영
A thesis of the Degree of Master
정원창 접근법을 이용한 와우이식에서의 전신적 스테로이드의 청력 보존 효과:
기니픽 모델
The effect of systemic steroid on hearing preservation after cochlear implantation via round window approach: A guinea pig model
January 2016
The Department of Otorhinolaryngology Head and Neck Surgery, Seoul National
University College of Medicine
Mun Young Chang
정원창 접근법을 이용한 와우이식에서의 전신적 스테로이드의 청력 보존 효과:
기니픽 모델
지도교수 이준호
이 논문을 장문영 석사학위논문으로 제출함
2016년 1월
서울대학교 대학원
의학과 이비인후과전공
장 문 영
장문영의 석사학위논문을 인준함
2016년 1월
위 원 장 (인)
부 위 원 장 (인)
위 원 (인)
The effect of systemic steroid on hearing preservation after cochlear implantation via round window approach: A guinea pig model
by
Mun Young Chang
A thesis submitted to the Department of Otorhinolaryngology Head and Neck Surgery in partial fulfillment of the requirement for the Degree
of Master at Seoul National University College of Medicine
January 2016
Approved by Thesis Committee:
Professor Chairman Professor Vice chairman Professor
i
ABSTRACT
This study aimed to evaluate the efficacy of perioperative systemic steroid administration and to compare the effects of its two postoperative administration periods, three days and seven days, for long-term hearing preservation after cochlear implantation via round window approach. Thirty Dunkin-Hartley guinea pigs were randomly segregated into three experimental groups: the control group (n = 10); the 3-day infusion group receiving steroid for postoperative three days (n = 10); and the 7-day infusion group receiving steroid for postoperative seven days (n = 10). All animals, regardless of group, received electrode insertion surgery. A slim straight dummy practice electrode for human (Cochlear Ltd, Lane Cove NSW, Australia) was inserted to a depth of 2.25 mm via a round window. A mini- osmotic pump (10μl/hr, Alzet, USA), filled with dexamethasone sodium phosphate (4mg/ml), was inserted subcutaneously 12 hours prior to electrode insertion, and removed three days or seven days after electrode insertion, depending on the group.
The hearing thresholds (tone pips at 2, 8, 16, 24, 32 kHz) were measured four times—once prior to electrode insertion, and at 1 week, 4 weeks, and 12 weeks after electrode insertion—by an auditory brainstem response. Histologic evaluation of the cochlea
ii
was performed at 12 weeks after electrode insertion. At 4 weeks after electrode insertion, auditory brainstem response threshold shifts in the 7-day infusion group were significantly lower than the control group at all frequencies. The 7-day infusion group kept significantly better hearing preservation compared with the control group after 12 weeks of implantation. The tissue response, including fibrosis and ossification was significantly reduced in the 7-day infusion group compared with the control groups. The outer hair cells of the basal, middle and apical turns and inner hair cells of the basal and middle turns were preserved significantly more in the 7-day infusion group than in the control group. The spiral ganglion cell densities of the basal, middle and apical turns were significantly higher in the 7-day infusion group compared with the control group. Based on our results, it appears that there is an effective postoperative period that is optimal for hearing preservation after electrode insertion. Administration of perioperative systemic steroid during this period could contribute to residual hearing preservation.
--- Keywords: cochlear implantation, hearing preservation, residual hearing, steroid, round window approach
Student number: 2014-21131
iii
CONTENTS
Abstract...i
Contents...iii
List of Tables and Figures...v
Introduction...1
Methods...4
Experimental Design...4
Auditory Brainstem Response Recordings ...5
Electrode Insertion Surgery ...6
Histological Analyses ...6
Calculation of Human Equivalent Dose of delivered steroid...8
Statistical Analyses ...8
Results...9
ABR and Steroid Treatment ...9
Tissue Response and Steroid Group ...10
Hair Cell and Spiral Ganglion Cell Counts...11
iv
Calculation of Human Equivalent Dose of delivered steroid...12
Discussion...13
Conclusion...18
References...19
Abstract in Korean...37
v
LIST OF TABLE AND FIGURES
Table
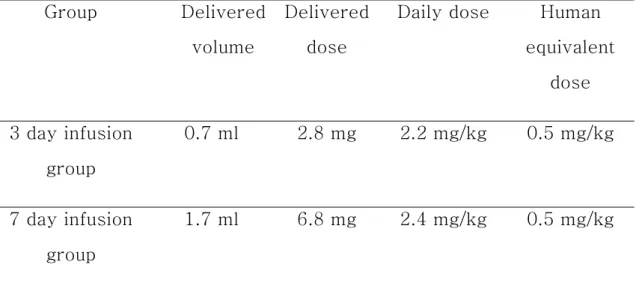
Table 1. Calculation of human equivalent dose of delivered dexamethasone sodium phosphate...28
Figure
Figure 1. Threshold shifts after electrode insertion...29 Figure 2. Tissue response in the lower basal turn at 12 weeks after electrode insertion...31 Figure 3. Tissue response after electrode insertion...32 Figure 4. Hair cell and spiral ganglion cell counts...33 Figure 5. The spiral ganglion cell density of the middle turn at 12 weeks after electrode...35 Figure 6. Threshold shifts occurred at two periods: before and after the one week mark post-electrode insertion...36
1
INTRODUCTION
As the technology of cochlear implants and surgical techniques improve, the indication criteria for cochlear implantation have been extended. Patients with residual hearing at low frequencies are becoming the candidate for cochlear implantation.1 Electric- acoustic stimulation (EAS), which is the use of cochlear implant aided by residual hearing in the same ear, has demonstrated auditory benefits, including speech recognition in the noise circumstance, sound resolution, and music recognition.2 Recently, topics surrounding the preservation of residual hearing regarding cochlear implantation has become increasingly popular. In efforts to preserve residual hearing, surgical techniques and pharmacological treatment must be improved.
As a surgical technique for cochlear implantation, cochleostomy has been widely used. However, despite its wide usage, conventional cochleostomy has some demerits that are caused by acoustic trauma and formation of bone dust during the procedure.1,3,4 Therefore, a cochleostomy based on “soft surgery” and round window approach have been promoted. These techniques have been used widely in clinical practice. However, in animal studies evaluating the hearing preservation,
2
cochleostomy has commonly been used, while a round window approach has never been applied. As acoustic trauma caused by cochleostomy can make additional hearing loss, it can conceal the hearing preservation effect of tested methods.
Steroid, as a form of pharmacological treatment, has been developed. The effect of steroid for the residual hearing preservation has been shown in several previous studies.5-12 There are two ways for delivering steroids into the cochlea: local and systemic delivery. Local delivery was highlighted as it reduces the systemic adverse effects of steroids. However, local delivery has several limitations. First, it takes a long time for the steroids to diffuse sufficiently throughout the round window.11 As local delivery is usually performed in the operating room before cochlear implantation, it may extend the time for general anesthesia. Furthermore, it was reported that the long diffusion period was not reduced in spite of the high concentration of steroids.11 Second, there is doubt that locally delivered steroid could reach the apical turn of the cochlea. It was reported that there was a substantial difference of steroid dose between the basal and apical turns after local delivery of steroids.13 Therefore, although locally delivered steroid could reach the apical turn, there still exists uncertainty that the dose is sufficient enough to prevent hearing loss. Conversely, systemically delivered steroid
3
was reported to reach the cochlea and subsist for several hours.14 Systemic steroid application may be an alternative to local application because of for these reasons.
Previous studies that used the systemic approach only administered the steroid preoperatively,5,11 and to the best of our knowledge, there has not been a report which includes postoperative systemic steroid administration. In addition, there has not been an animal study that evaluated the efficacy of systemic steroid for hearing preservation in cochlear implantation using a round window approach. We aimed to evaluate the effects of perioperative, including postoperative, steroid administration for the preservation of residual hearing in a guinea pig model via round window approach.
4
METHODS
Experimental Design
This study was approved by the Institutional Animal Care and Use Committee of Seoul National University Hospital (12-0379- C2A1). Auditory brainstem response (ABR) recording and surgical procedures were performed under anesthesia using intramuscular administration of ketamine (40 mg/kg) mixed with xylazine (4 mg/kg). Thirty Dunkin-Hartley guinea pigs were randomly segregated into one of three experimental groups: the control group (n = 10); the 3-day infusion group receiving steroid for postoperative three days (n = 10); and the 7-day infusion group receiving steroid for postoperative seven days (n
= 10). Steroid was delivered systemically through a mini- osmotic pump (ALZET®) with an infusion rate of 10.0 µl/hr. This mini-osmotic pump was filled with dexamethasone sodium phosphate (5 mg/ml) 1.6 ml and normal saline 0.4 ml, and it was inserted into the subcutaneous pocket of the back about 12 hours prior to electrode insertion. After a set period—postoperative three days or seven days, depending on the group—the mini- osmotic pump was removed and the volume of remained solution in the pump was measured.
5
Auditory Brainstem Response Recordings
The hearing of the left ear of all animals was estimated by ABRs to tone pips before surgery. ABRs were recorded using subdermal needle electrodes below the both ears and at the vertex. Tone pips of 2, 8, 16, 24 and 32 kHz were presented as the sound stimuli (1562 μm duration, cos shaping, 21 Hz). ABRs were measured employing the Intelligent Hearing System (HIS Inc., Miami, FL, USA) which used IHS high-frequency transducers (HFT9911—20—0035) and IHS high-frequency software (ver. 2.33). The responses were amplified (100,000×), band pass-filtered (100—1500 Hz), and then averaged over stimulus repetitions. Two researchers, without information about the experimental group and animal number, investigated thresholds by decreasing stimuli intensity in 5 dB decrements.
The lowest level that recognizable responses present was determined as threshold. Animals then underwent electrode insertion. Further ABR thresholds were measured at 1, 4 and 12 weeks postoperatively. The threshold shift was calculated by subtracting the preoperative threshold from each of the postoperative thresholds. Therefore, a threshold shift more than zero meant an elevation of threshold.
6
Electrode Insertion Surgery
All animals received electrode insertion surgery at the left side. Analgesic medication, meloxicam (0.2 mg/kg) was administered to all animals before and after surgery. A 4-mm cutting burr was used to perform bullectomy and expose the round window under the operating microscope. An incision was made on the round window membrane. A slim straight dummy practice electrode for humans (Cochlear Ltd, Lane Cove NSW, Australia) was inserted through the round window with a depth of 2.25 mm, and then left in situ. The soft tissue was packed around the electrode to reduce the possibility of electrode migration and perilymph leakage.
Histological Analyses
After the last ABR recording, an overdose of ketamine was administered to animals. Then animals were perfused with 0.9%
saline and 4% (v/v) paraformaldehyde (PFA), and the cochleae were extracted. The harvested cochleae were placed in 4% PFA in PBS overnight and decalcified in 4% (w/v) EDTA (pH 7.4) (Santa Cruz Biotechnology, Santa Cruz, CA) in PBS for more than 2 weeks. After completion of decalcification, the electrodes were removed, and the trimmed cochleae were embedded in paraffin.
7
Sections of 5 μm were taken every 125 μm from the mid- modiolar area through the cochlea. Hematoxylin and eosin (H&E) staining was performed. Histological analyses of the basal, middle and apical turns of the cochlea were performed under the light microscopy (CX31; Olympus, Tokyo, Japan). A tissue response was apparent on the lower basal turn, where the electrode was inserted. There was no apparent tissue response on the apical and middle turns. Microscopic images of 8-10 sequential sections around the region with the most apparent tissue responses in 125-μm steps were converted to JPEG files and saved at the same magnification to measure the tissue responses, such as fibrosis and ossification. The areas of the scala tympani, fibrosis and ossification were measured employing Image J software (National Institute of Health, Bethesda, MD). The percentage of each area in scala tympani was calculated and averaged across 8-10 sequential sections. To count the outer hair cells (OHCs) and inner hair cells (IHCs) of the basal, middle and apical turns, 8-10 sequential sections around the mid- modiolar region were examined. The numbers of OHCs and IHCs were averaged across 8-10 sequential sections. To measure the spiral ganglion cell densities, microscopic images of the basal, middle and apical turns of the mid-modiolar section were examined. All type I cells with a clear nucleus were counted in the Rosenthal’s canal. These were divided by the canal area
8
using Image J software.
Calculation of Human Equivalent Dose of delivered steroid
The volume of delivered dexamethasone sodium phosphate was calculated from the volume of remained solution in the pump after a set period; postoperative three days or seven days. Then, the daily doses of delivered dexamethasone sodium phosphate were calculated. From these results, the human equivalent doses of dexamethasone sodium phosphate were calculated.15
Statistical Analyses
IBM SPSS software version 21.0 was used for statistical analyses. The differences of threshold shifts and histological findings among the experimental groups evaluated using the Kruskall-Wallis test and Bonferroni correction method.
9
RESULTS
ABR and Steroid Treatment
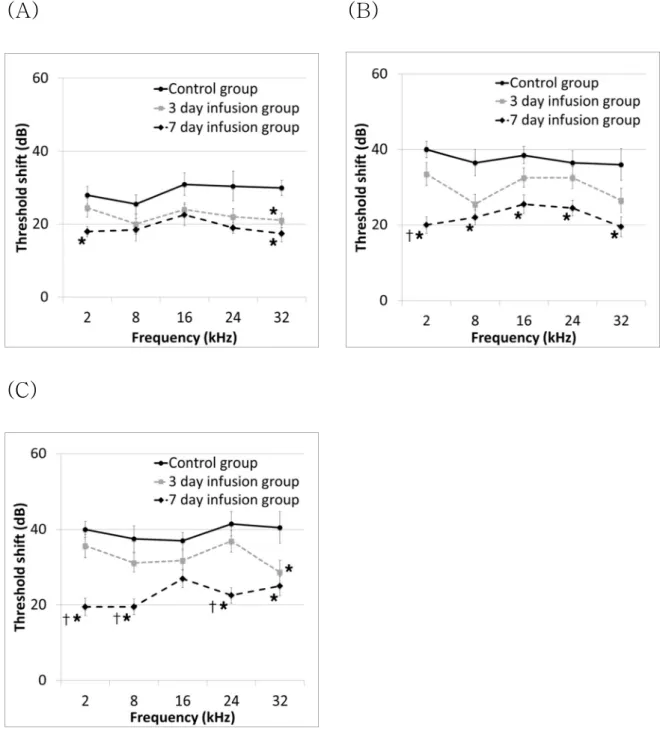
There was no significant difference of ABR threshold among the three groups before electrode insertion. At 1 week after electrode insertion, ABR threshold shifts at 2 and 32 kHz were lower in the 7-day infusion group than the control group with statistical significance (Bonferroni corrected p = 0.009 and 0.006). ABR threshold shift at 32 kHz was lower in the 3-day infusion group than the control group with statistical significance (Bonferroni corrected p = 0.021). At 4 weeks after electrode insertion, ABR threshold shifts at all frequencies were lower in the 7-day infusion group than the control group with statistical significance (Bonferroni corrected p < 0.001, p = 0.006, 0.009, 0.03 and 0.021). ABR threshold shift at 2 kHz was significantly lower in the 7-day infusion group than the 3-day infusion group (Bonferroni corrected p = 0.021). At 12 weeks after surgery, ABR threshold shifts at 2, 8, 24 and 32 kHz were significantly lower in the 7-day infusion group than the control group (Bonferroni corrected p = 0.003, 0.009, 0.003 and 0.003). ABR threshold shift at 32 kHz was statistically significantly lower in the 3-day infusion group than the control group (Bonferroni
10
corrected p = 0.009). ABR threshold shift at 2, 8 and 24 kHz was significantly lower in the 7-day infusion group than the 3-day infusion group (Bonferroni corrected p = 0.003, 0.018 and 0.003) (Fig. 1).
Tissue Response and Steroid Group
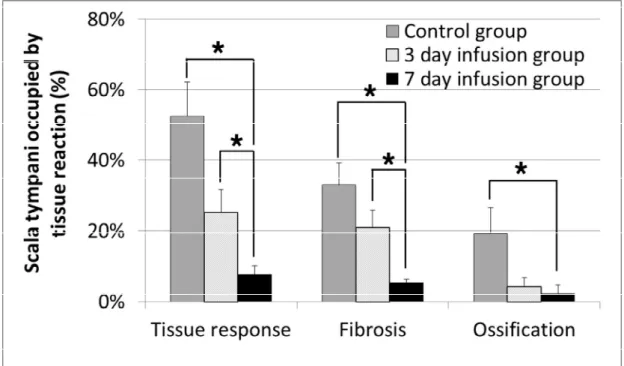
The mean percentages of the tissue response, including fibrosis and ossification in the control (n=8), 3-day infusion (n=10) and 7-day infusion (n=10) groups were evaluated. The tissue response occurred more in the control group (52.5 % ± 27.4%) than in 3-day infusion group ( 25.4 % ± 20.1%) and 7- day infusion gropu (7.6 % ± 7.8%). The tissue response was significantly reduced in the 7-day infusion group compared with the 3-day infusion and control groups (Bonferroni corrected p = 0.006 and 0.003). Fibrosis was also significantly reduced in the 7-day infusion group compared with the 3-day infusion and control groups (Bonferroni corrected p < 0.001). Ossification was significantly reduced in the 7-day infusion group compared with the control group (Bonferroni corrected p = 0.048). The tissue response in the 3-day infusion group did not show a statistically significant difference compared with the control group (Fig. 2 and 3).
11
Hair Cell and Spiral Ganglion Cell Counts
OHC counts of the basal, middle and apical turns were significantly higher in the 7-day infusion group compared with the control group (Bonferroni corrected p < 0.05). OHC counts of the mid and apical turns were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.001). IHC counts of the basal and middle turns were significantly higher in the 7-day infusion group compared with the control group (Bonferroni corrected p <
0.05). IHC counts of the basal turn were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.05). The 3-day infusion group failed to show significantly better results compared with the control group (Fig. 4 (A) and (B)). The spiral ganglion cell densities of the basal, middle and apical turns were significantly higher in the 7-day infusion group compared with the control group (Bonferroni corrected p < 0.05). The spiral ganglion cell densities of the basal and apical turns were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.05). Moreover, the 3-day infusion group failed to show a significantly higher spiral ganglion cell density compared with the control group (Fig. 4 (C) and 5).
12
Calculation of Human Equivalent Dose of delivered steroid
The volumes and daily doses of delivered dexamethasone sodium phosphate were described in Table 1. The calculated human equivalent doses of dexamethasone sodium phosphate were 0.5 and 0.5 mg/kg/day for 3-day and 7-day infusion groups, respectively (Table 1).15
13
DISCUSSION
The otoprotective effects of steroids in cochlear implantation have been proven by several animal studies, while no animal study used systemic steroid administration postoperatively.5,7,11,12,16 If there is a time delay between electrode insertion and irreversible histologic changes, which induces residual hearing loss, otoprotective medications administered postoperatively during this period can block the progression of irreversible histologic changes. There were two experiments that evaluated the time course of histologic changes in the cochlea. In the first experiment that guinea pigs were exposed to intense continuous noise, degeneration of IHC and OHC began 5 days after noise-exposure. Degeneration of spiral ganglion cell was observed 4 weeks after noise-exposure.17,18 In the second experiment that subcutaneous implants were made in rats, fibroblast recruitment and activation started on the 14th day after implantation.19 Although the settings of Fredelius and Patil’
s experiment are not exactly the same as ours, the aforementioned irreversible changes are estimated to occur several days after electrode insertion. As such, it is predicted that if some treatment blocks the pathway that induces the loss
14
of OHC, IHC, and spiral ganglion cell and fibrosis during this period, more OHC, IHC and spiral ganglion cell could survive and fibrosis could be reduced. Therefore, we hypothesized that perioperative, including postoperative, administration of systemic steroid could be beneficial for hearing preservation.
We administered systemic steroid using a mini-osmotic pump.
The delivery rate of the mini-osmotic pump reaches steady state after about 5 hours and keeps constant during the remaining period.20 To make sure that the postoperative delivery rate is constant, the mini-osmotic pump was inserted about 12 hours prior to electrode insertion. Moreover, we wanted to evaluate the effect of systemic steroid according to postoperative administration period. In this study, we made two sets of period for systemic steroid delivery: postoperative three days and seven days. The 7-day infusion group achieved better hearing preservation than the control group, while the 3-day infusion group failed. It could be tempting to predict that a longer duration of steroid administration may be more effective to hearing preservation. However, due to adverse effects of systemic steroid use, unnecessary use of steroids should be prohibited. To investigate the appropriate minimal duration for systemic steroid use, we analyzed the threshold shifts that occurred before and after the one week mark post-electrode insertion. Most of the
15
hearing loss occurred at the first week after electrode insertion in all experimental groups (Fig. 6). This pattern of hearing loss after electrode insertion was consistent with the results of a previous study.11 In addition, although administration of steroid was stopped at 7 days post electrode insertion, the mean threshold shifts of the 7-day infusion group, which occurred from 1 to 12 weeks after electrode insertion, were less than 5 dB at all frequencies, except at 32 kHz; and the mean threshold shift at 32 kHz was 7.5 dB. Therefore, administration of steroids for more than 7 days does not seem to significantly contribute to hearing preservation. Considering the adverse effects of systemic steroid, it is not recommendable to administer steroids for more than 7 days after electrode insertion. Consequently, the optimal period of systemic steroid administration seems to be about 7 days.
Several studies have been performed to investigate the histologic changes that induce hearing loss after cochlear implantation. The loss of OHC, IHC and spiral ganglion cell, as well as intracochlear tissue responses, including fibrosis and ossification, have been reported as the main histologic changes.5,11,21-23 The pathophysiology of these changes after electrode insertion has been reported by several studies. The reactive oxygen species (ROS) and pro-inflammatory and
16
apoptotic cytokines, such as tumor necrosis factor-alpha (TNF- α), were suggested as the main factors. They lead OHC, IHC and spiral ganglion cell to apoptosis or necrosis.6,10,22,24-28 In addition, TNF-α recruits various inflammatory cells and induces inflammatory response.29-32 After these acute reactions, fibrosis and ossification are formed in the cochlea by chronic inflammation and foreign body reaction.11,33 The three outlined otoprotective effects of steroids are as follows: anti-apoptotic, anti-oxidative, and anti-inflammatory effects, which block the effects of ROS and TNF-α.6,10,34-39 Therefore, we expected that steroid administration could protect OHC, IHC, and spiral ganglion cell and prevent tissue responses, such as fibrosis and ossification after electrode insertion. In this study, such changes were evaluated. The 7-day infusion group achieved better results than the control group; however the 3-day infusion group achieved better results only in preventing fibrosis than the control group. These histologic protections in the 7-day infusion group may contribute to hearing preservation. Based on these results, we could suggest that there might be an effective postoperative period that is optimal for hearing preservation after electrode insertion; and better hearing preservation can be achieved by postoperatively administrating steroids for about 7 days or more.
17
To evaluate the safety of systemic steroid administration after electrode insertion, we calculated the human equivalent dose of delivered dexamethasone sodium phosphate for the 7-day infusion group (0.5 mg/kg/day) (Table 1).15 The preoperative administration period was calculated as 6 hours considering the time required to reach a constant delivery rate.20 The dose for a 70 kg adult is 35 mg/day. Considering that methylprednisolone 1000 mg/day (dexamethasone sodium phosphate 187.5 mg/day) is administer to the patient with optic neuropathy,40,41 this dose is not intolerable. Therefore, the systemic steroid dosage suggested from this study maybe applicable to humans.
This study had a few limitations. The level of steroid in the blood and main molecular factors for hearing loss, such as ROS and TNF-α, were not measured in this study. As the delivery rate of the mini-osmotic pump reaches steady state about 5 hours after the pump insertion, the level of steroid in the blood was inferred as constant. However, direct measurement of these factors could make the results of this study more solid. Further studies are needed to confirm the otoprotective effects of perioperative systemic steroid administration.
18
CONCLUSION
In this study, perioperative steroid application, including postoperative seven days, showed significant residual hearing preservation. These effects might be attributed to the protection of OHC, IHC, and spiral ganglion cell, and prevention of tissue responses, such as fibrosis and ossification. Based on our results, it appears that there is an effective postoperative period optimal for hearing preservation after electrode insertion. Administration of steroid during this period could contribute to residual hearing preservation.
19
REFERENCES
1. Havenith S, Lammers MJ, Tange RA, Trabalzini F, della Volpe A, van der Heijden GJ, et al. Hearing preservation surgery:
cochleostomy or round window approach? A systematic review.
Otol Neurotol. 2013;34(4):667-74.
2. Podskarbi-Fayette R, Pilka A, Skarzynski H. Electric stimulation complements functional residual hearing in partial deafness. Acta Otolaryngol. 2010;130(8):888-96.
3. Kylen P, Arlinger S. Drill-generated noise levels in ear surgery. Acta Otolaryngol. 1976;82(5-6):402-9.
4. Seki M, Miyasaka H, Edamatsu H, Watanabe K. Changes in permeability of strial vessels following vibration given to auditory ossicle by drill. Ann Otol Rhinol Laryngol. 2001;110(2):122-6.
5. Connolly TM, Eastwood H, Kel G, Lisnichuk H, Richardson R, O'Leary S. Pre-operative intravenous dexamethasone prevents auditory threshold shift in a guinea pig model of cochlear implantation. Audiol Neurootol. 2011;16(3):137-44.
6. Dinh CT, Haake S, Chen S, Hoang K, Nong E, Eshraghi AA, et al. Dexamethasone protects organ of corti explants against tumor necrosis factor-alpha-induced loss of auditory hair cells
20
and alters the expression levels of apoptosis-related genes.
Neuroscience. 2008;157(2):405-13.
7. Eastwood H, Chang A, Kel G, Sly D, Richardson R, O'Leary SJ. Round window delivery of dexamethasone ameliorates local and remote hearing loss produced by cochlear implantation into the second turn of the guinea pig cochlea. Hear Res.
2010;265(1-2):25-9.
8. Eshraghi AA, Adil E, He J, Graves R, Balkany TJ, Van De Water TR. Local dexamethasone therapy conserves hearing in an animal model of electrode insertion trauma-induced hearing loss.
Otol Neurotol. 2007;28(6):842-9.
9. Eshraghi AA, Dinh CT, Bohorquez J, Angeli S, Abi-Hachem R, Van De Water TR. Local drug delivery to conserve hearing:
mechanisms of action of eluted dexamethasone within the cochlea.
Cochlear Implants Int. 2011;12 Suppl 1:S51-3.
10. Haake SM, Dinh CT, Chen S, Eshraghi AA, Van De Water TR. Dexamethasone protects auditory hair cells against TNFalpha-initiated apoptosis via activation of PI3K/Akt and NFkappaB signaling. Hear Res. 2009;255(1-2):22-32.
11. Lee J, Ismail H, Lee JH, Kel G, O'Leary J, Hampson A, et al.
Effect of both local and systemically administered dexamethasone on long-term hearing and tissue response in a
21
Guinea pig model of cochlear implantation. Audiol Neurootol.
2013;18(6):392-405.
12. Lee MY, Lee JH, Lee HS, Choi JJ, Jang J, Choi H, et al.
Continuous topical drug delivery using osmotic pump in animal cochlear implant model: Continuous steroid delivery is effective for hearing preservation. Acta Otolaryngol. 2015;135(8):791-8.
13. Plontke SK, Biegner T, Kammerer B, Delabar U, Salt AN.
Dexamethasone concentration gradients along scala tympani after application to the round window membrane. Otol Neurotol.
2008;29(3):401-6.
14. Tobita T, Senarita M, Hara A, Kusakari J. Determination of prednisolone in the cochlear tissue. Hear Res. 2002;165(1- 2):30-4.
15. Reagan-Shaw S, Nihal M, Ahmad N. Dose translation from animal to human studies revisited. Faseb j. 2008;22(3):659-61.
16. Rajan GP, Kuthubutheen J, Hedne N, Krishnaswamy J. The role of preoperative, intratympanic glucocorticoids for hearing preservation in cochlear implantation: a prospective clinical study.
Laryngoscope. 2012;122(1):190-5.
17. Fredelius L. Time sequence of degeneration pattern of the organ of Corti after acoustic overstimulation. A transmission
22
electron microscopy study. Acta Otolaryngol. 1988;106(5- 6):373-85.
18. Fredelius L, Rask-Andersen H, Johansson B, Urquiza R, Bagger-Sjoback D, Wersall J. Time sequence of degeneration pattern of the organ of Corti after acoustic overstimulation. A light microscopical and electrophysiological investigation in the guinea pig. Acta Otolaryngol. 1988;106(1-2):81-93.
19. Patil SD, Papadimitrakopoulos F, Burgess DJ.
Dexamethasone-loaded poly(lactic-co-glycolic) acid microspheres/poly(vinyl alcohol) hydrogel composite coatings for inflammation control. Diabetes Technol Ther. 2004;6(6):887-97.
20. Theeuwes F, Yum SI. Principles of the design and operation of generic osmotic pumps for the delivery of semisolid or liquid drug formulations. Ann Biomed Eng. 1976;4(4):343-53.
21. Eshraghi AA, Polak M, He J, Telischi FF, Balkany TJ, Van De Water TR. Pattern of hearing loss in a rat model of cochlear implantation trauma. Otol Neurotol. 2005;26(3):442-7;
discussion 7.
22. Abi-Hachem RN, Zine A, Van De Water TR. The injured cochlea as a target for inflammatory processes, initiation of cell death pathways and application of related otoprotectives strategies. Recent Pat CNS Drug Discov. 2010;5(2):147-63.
23
23. Van De Water TR, Abi Hachem RN, Dinh CT, Bas E, Haake SM, Hoosien G, et al. Conservation of hearing and protection of auditory hair cells against trauma-induced losses by local dexamethasone therapy: molecular and genetic mechanisms.
Cochlear Implants Int. 2010;11 Suppl 1:42-55.
24. Cheng AG, Cunningham LL, Rubel EW. Mechanisms of hair cell death and protection. Curr Opin Otolaryngol Head Neck Surg.
2005;13(6):343-8.
25. Micheau O, Tschopp J. Induction of TNF receptor I- mediated apoptosis via two sequential signaling complexes. Cell.
2003;114(2):181-90.
26. Muppidi JR, Tschopp J, Siegel RM. Life and death decisions: secondary complexes and lipid rafts in TNF receptor family signal transduction. Immunity. 2004;21(4):461-5.
27. Zine A, van de Water TR. The MAPK/JNK signalling pathway offers potential therapeutic targets for the prevention of acquired deafness. Curr Drug Targets CNS Neurol Disord.
2004;3(4):325-32.
28. Zou J, Pyykko I, Sutinen P, Toppila E. Vibration induced hearing loss in guinea pig cochlea: expression of TNF-alpha and VEGF. Hear Res. 2005;202(1-2):13-20.
24
29. Keithley EM, Wang X, Barkdull GC. Tumor necrosis factor alpha can induce recruitment of inflammatory cells to the cochlea.
Otol Neurotol. 2008;29(6):854-9.
30. Ichimiya I, Yoshida K, Hirano T, Suzuki M, Mogi G.
Significance of spiral ligament fibrocytes with cochlear inflammation. Int J Pediatr Otorhinolaryngol. 2000;56(1):45-51.
31. Ichimiya I, Yoshida K, Suzuki M, Mogi G. Expression of adhesion molecules by cultured spiral ligament fibrocytes stimulated with proinflammatory cytokines. Ann Otol Rhinol Laryngol. 2003;112(8):722-8.
32. Satoh H, Firestein GS, Billings PB, Harris JP, Keithley EM.
Tumor necrosis factor-alpha, an initiator, and etanercept, an inhibitor of cochlear inflammation. Laryngoscope.
2002;112(9):1627-34.
33. Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Semin Immunol. 2008;20(2):86-100.
34. Forster C, Kahles T, Kietz S, Drenckhahn D.
Dexamethasone induces the expression of metalloproteinase inhibitor TIMP-1 in the murine cerebral vascular endothelial cell line cEND. J Physiol. 2007;580(Pt.3):937-49.
35. Harkness KA, Adamson P, Sussman JD, Davies-Jones GA,
25
Greenwood J, Woodroofe MN. Dexamethasone regulation of matrix metalloproteinase expression in CNS vascular endothelium.
Brain. 2000;123 ( Pt 4):698-709.
36. Hoang KN, Dinh CT, Bas E, Chen S, Eshraghi AA, Van De Water TR. Dexamethasone treatment of naive organ of Corti explants alters the expression pattern of apoptosis-related genes. Brain Res. 2009;1301:1-8.
37. Meltser I, Tahera Y, Canlon B. Glucocorticoid receptor and mitogen-activated protein kinase activity after restraint stress and acoustic trauma. J Neurotrauma. 2009;26(10):1835-45.
38. Nagashima R, Ogita K. Enhanced biosynthesis of glutathione in the spiral ganglion of the cochlea after in vivo treatment with dexamethasone in mice. Brain Res.
2006;1117(1):101-8.
39. Tailor A, Tomlinson A, Salas A, Panes J, Granger DN, Flower RJ, et al. Dexamethasone inhibition of leucocyte adhesion to rat mesenteric postcapillary venules: role of intercellular adhesion molecule 1 and KC. Gut. 1999;45(5):705-12.
40. Bennett JL, Nickerson M, Costello F, Sergott RC, Calkwood JC, Galetta SL, et al. Re-evaluating the treatment of acute optic neuritis. J Neurol Neurosurg Psychiatry. 2015;86(7):799-808.
26
41. Mustafa S, Pandit L. Approach to diagnosis and management of optic neuropathy. Neurol India. 2014;62(6):599- 605.
27
Table 1. Calculation of human equivalent dose of delivered dexamethasone sodium phosphate.
Group Delivered volume
Delivered dose
Daily dose Human equivalent
dose 3 day infusion
group
0.7 ml 2.8 mg 2.2 mg/kg 0.5 mg/kg
7 day infusion group
1.7 ml 6.8 mg 2.4 mg/kg 0.5 mg/kg
28
(A) (B)
(C)
Figure 1. Threshold shifts after electrode insertion.
Frequency-specific threshold shifts for the control, 3-day and 7-day infusion groups. (A) One week after electrode insertion.
(B) Four weeks after electrode insertion. (C) Twelve weeks after electrode insertion. *Statistically significant difference in
29
the threshold shift compared with the control group (Bonferroni corrected p < 0.05). †Statistically significant difference in the threshold shift compared with the 3-day infusion group (Bonferroni corrected p < 0.05). Error bar means standard error.
30
(A) (B)
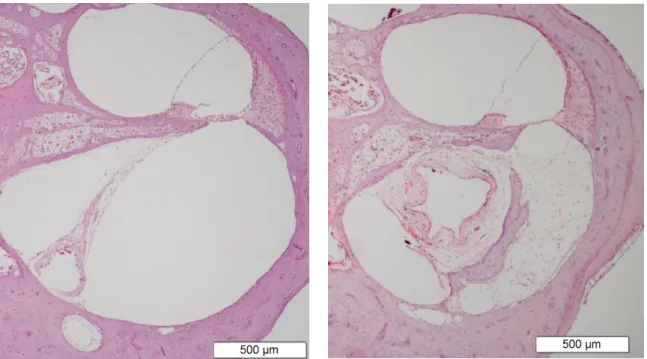
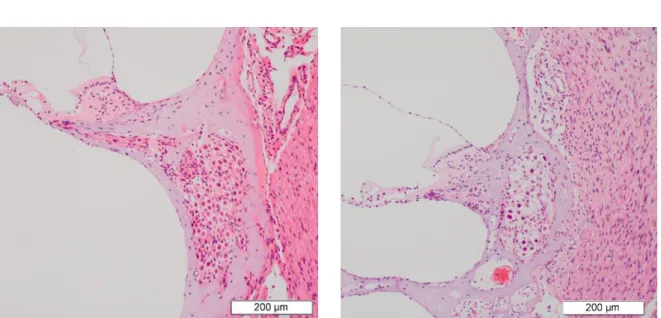
Figure 2. Tissue response in the lower basal turn at 12 weeks after electrode insertion.
Tissue response, including fibrosis and ossification, was reduced in the 7-day infusion group (A) compared with the control group (B).
31
Figure 3. Tissue response after electrode insertion.
Tissue response was significantly reduced in the 7-day infusion group compared with the 3-day infusion and control groups (Bonferroni corrected p = 0.006 and 0.003). Fibrosis was also significantly reduced in the 7-day infusion group compared with the 3-day infusion and control groups (Bonferroni corrected p <
0.001). Ossification was significantly reduced in the 7-day infusion group compared with control group (Bonferroni corrected p = 0.048). *Statistically significant difference between the groups (Bonferroni corrected p < 0.05). Error bar means standard error.
32
(A) (B)
(C)
Figure 4. Hair cell and spiral ganglion cell counts.
(A) OHC counts of the basal, middle and apical turns were significantly higher in the 7-day infusion group compared with the control group (Bonferroni corrected p < 0.05). OHC counts of the mid and apical turns were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.001). (B) IHC counts of the basal and middle turns were significantly higher in the 7-day infusion
33
group compared with the control group (Bonferroni corrected p <
0.05). IHC counts of basal turn were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.05). (C) spiral ganglion cell densities of the basal, middle and apical turns were significantly higher in the 7-day infusion group compared with the control group (Bonferroni corrected p < 0.05). Spiral ganglion cell densities of the basal and apical turns were significantly higher in the 7-day infusion group compared with the 3-day infusion group (Bonferroni corrected p < 0.05). *Statistically significant difference between the groups (Bonferroni corrected p < 0.05).
Error bar means standard error.
OHC, outer hair cell; IHC, inner hair cell.
34
(A) (B)
Figure 5. The spiral ganglion cell density of the middle turn at 12 weeks after electrode.
The spiral ganglion cell density was higher in the 7-day infusion group (A) compared with the control group (B).
35
(A) (B)
(C)
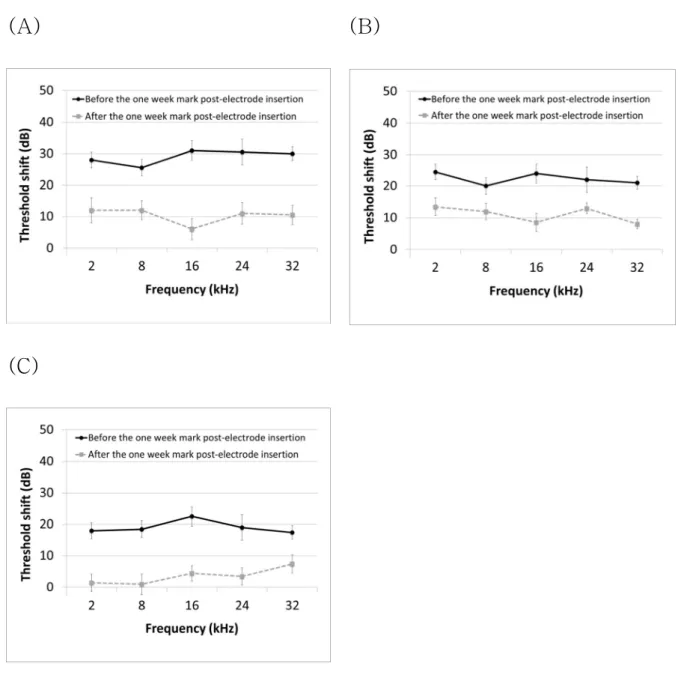
Figure 6. Threshold shifts occurred at two periods: before and after the one week mark post-electrode insertion.
The period after one week mark post-electrode insertion included from the one week post-electrode insertion to 12 weeks post-electrode insertion. Most of the hearing loss occurred before the 1 week mark. In the 7-day infusion group, threshold shifts between 1 week and 12 weeks post-electrode
36
insertion were less than 5 dB at all frequencies, except 32 kHz.
(A) Control group. (B) 3-day infusion group. (C) 7-day infusion group. Error bar means standard error.
37
국문 초록
본 연구는 정원창 접근법을 이용한 와우이식 후 장기 잔청 보존을 위한 수술전후 스테로이드 투여의 효과와 두 가지 술후 스테로이드 투여 기간, 3일과 7일의 효과를 비교하기 위한 연구이다. 총 30마리 의 던킨-하틀리 기니픽을 무작위로 3개의 군으로 배정하였다: 대조 군 (n=10); 술후 3일간 스테로이드 투여군 (n=10), 술후 7일간 스 테로이드 투여군 (n=10). 모든 동물에서 전극 삽입 수술을 시행하였 다. 인체에 사용하는 slim straight dummy practice electrode (Cochlear Ltd, Lane Cove NSW, Australia)를 정원창을 통해 2.25mm 깊이로 삽입하였다. 덱사메타손 (4mg/ml)으로 채운 소형 삼투압 연속약물주입폄프 (10μl/hr, Alzet, USA)를 전극 삽입 12시 간 전에 피하 주머니에 삽입한 후 전극 삽입 3일 혹은 7일 후에 제 거하였다 (3일 투여군과 7일 투여군). 전극 삽입 전, 전극 삽입 1, 4, 12주 후에 청성뇌간반응을 이용하여 청력 역치 (2, 8, 16, 24, 32 kHz)를 측정한다. 전극 삽입 12주 후에 와우의 조직학적 검사를 시 행하였다. 전극 삽입 4주 후, 7일 투여군의 청력 역치 변화는 대조군 보다 유의하게 작았다. 전극 삽입 12주 후까지 7일 투여군은 대조군 보다 좋은 청력을 유지하였다. 조직학적 검사 상 와우 고실계에 삽입 된 전극 주위로 섬유화와 골화가 7일 투여군보다 대조군에서 더 많이 발생하였다. 기저회전, 중간회전, 첨부회전의 외유모세포와 나선신경 절세포, 기저회전, 중간회전의 내유모세포는 대조군보다 7일 투여군에
38
서 유의하게 더 많이 보존되었다. 이 결과를 바탕으로 볼 때, 전극 삽 입 후 잔청 보존을 위한 가역적인 기간이 존재하는 것으로 판단된다.
이 기간 동안 수술전후 전신적인 스테로이드를 투여한다면 잔청 보존 의 효과를 얻을 수 있을 것으로 예상된다.
--- 주요어: 와우이식, 청력 보존, 잔청, 스테로이드. 정원창 접근법
학 번: 2014-21131