대한외과학회지:제 69 권 제 4 호
□ 증 례 □
Vol. 69, No. 4, October, 2005
350 서 론
황달성 간암은 대부분 말기 간세포암이거나 간내담관암 에 의해 담관에 폐쇄를 일으킨 경우이다. 이 중 황달성 간세 포암은 드물게 종양색전이 담관을 막아 황달을 야기시킬 수 있다. 이때 이 상태를 정확히 진단하여 치료하기는 어렵 다. 저자들의 경우에 수술 전 담관 폐쇄를 야기시킨 원인이 간내 담관암으로 여겨졌으나 수술 후 종양색전에 의해 담 관을 폐쇄시킨 간세포암으로 판명된 환자 1예를 치험하였 기에 문헌 고찰과 함께 보고하는 바이다.
증 례
환 자: 52세, 남자
주 소: 내원 3일 전부터 발생한 빈혈 및 황달, 좌하복부 통증을 주소로 응급실을 통하여 입원하였다.
과거력 및 사회력: 당뇨(내원 약 2년 전부터 복용) 가족력: 특이 소견 없음.
이학적 소견 및 활력증후: 내원시 혈압은 120/90 mmHg, 맥박은 98회/분, 호흡수 18회/분, 체온 37.8oC이었으며 빈혈 과 황달 그리고 좌하복 동통이 있었음.
검사소견: WBC: 2,500/ul, Hb: 29.4 gm/dl, Platelet: 82,000/ul HbsAg/Ab (-/-), AntiHC (-)
LFT (AST/ALT: 106 IU/97 IU, Total Bilirubin: 5.2 mg/dl), FBS:295 mg/dl
CA19-9: 1,916 U/ml, AF: 163 ng/ml ICG R 15: 9.7%
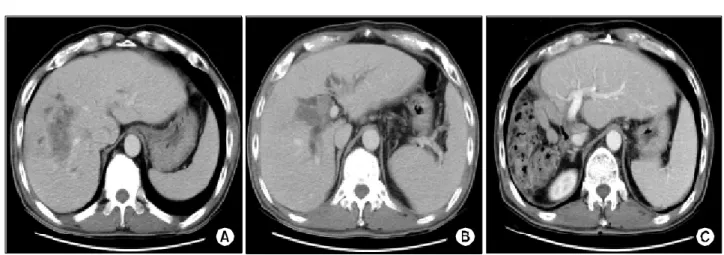
수술소견: 간은 전반적으로 소결절의 간경변을 보였고 우측 간에 약 6×7 cm의 종괴가 있었으며 간문부에는 지름 이 약 2 cm 가량인 종양 색전에 의해 막혀 있었고 주위 담 관에 붙어 있었으나 쉽게 제거가 가능하였다(Fig. 1A, B).
우측 간 동맥으로의 침범이 의심되었고 간 십이지장 인대 주위 림프절이 커진 소견이었다. 수술은 우측 간과 담관 절 제 및 림프절 절제술을 시행하였다(Fig. 1C, 2). 최종 병리조 직 검사상 간세포암으로 확진되었다(Fig. 3A, B).
고 찰
황달을 일으키는 간세포암은 대체적으로 예후가 불량하 지만 그 중 일부는 다른 원인으로 간문부나 간내담관을 폐 쇄하여 황달을 일으키는 경우는 상황이 다르다. 간세포암 으로 황달을 일으키는 경우는 약 19∼40%(1)에 해당하며 이는 주로 간경변이나 광범위 간세포 암의 침윤에 의해 간 기능 악화되어 생기는 경우이지만, 드문 경우에서 간세포 암이 간내담관을 침범하거나 종양색전을 야기하여 황달을 야기한다. Mallory 등(2)이 1947년 간외담관을 침범한 간세 포암을 보고하였고 Lin 등(3)은 1975년 408예의 간세포암 중 8예에서 담관을 침범을 확인하여 이것을 황달성 간세포 암(icteric hepatoma)라고 명명하였다. 이런 황달성 간세포암
간문부 담관 폐쇄에 의한 황달성 간세포암
청주성모병원 외과, 1소화기내과, 2병리과 이 종 률․김 미 성1․신 향 미2
Hepatocellular Carcinoma with Jaundice Caused by the Obstruction of Hepatic Hilum
Jong Riul Lee, M.D., Mi Sung Kim, M.D.1 and Hyang Mi Shin, M.D.2
The most causes of an icteric hepatoma are a late stage hepatocellular carcinoma or intrahepatic cholangiocarcinoma.
A hepatocellular carcinoma, causing an obstrucution of the bile duct, rarely results in jaundice. With a late stage hepa- tocellular carcinoma, the accurate diagnosis and treatment may be difficult. Herein, we report a case of a hepato- cellular carcinoma and obstructive jaundice, due to hilar tumor emboli, with a review of the literature.(J Korean Surg Soc 2005;69:350-352)
Key Words: Icteric hepatoma, Hilar tumor emboli 중심 단어: 황달성 간세포암, 간문부 종양색전 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Departments of General Surgery and 1Internal Medicine,
2Pathology, Cheongju St. Mary's Hospital, Cheongju, Korea
책임저자:이종률, 충북 청주시 상당구 주중동 589-5 ꂕ 360-568, 청주성모병원 외과
Tel: 043-219-8136, Fax: 043-212-5001 E-mail: [email protected]
접수일:2005년 4월 12일, 게재승인일:2005년 6월 14일 본 증례는 2004년 대한외과학회 춘계학술대회 포스터 발표됨.
이종률 외:간문부 담관 폐쇄에 의한 황달성 간세포암 351 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
을 담관폐쇄 과정에 따라 3가지로 분류하였는데(1,4,5) 1형 (type 1)을 간내 담관으로 종양의 협착(tumor encasement)이 일어난 경우, 2형(type 2)을 종양분절(tumor fragment)이나 혈전등에 의한 경우, 3형(type 3)은 종양이나 림프절이 직접 간문부를 폐쇄하는 경우로 하였다. 저자의 경우는 2형에 해 당된다. 진단은 수술 전에 정확히 내려지기가 어려운데 그 이유는 이런 병병의 발생이 적어 간문부 담관암으로 오인 하기 쉽기 때문이다. 초음파 검사, 컴퓨터 단층 촬영으로 간 내 종양의 위치, 담관확장, 담관 폐쇄 부위의 상황을 알 수 있지만 담관 폐쇄 부위를 보다 정확히 규명하기 위해서는 경피경 간담관조영술(PTC), 내시경적 역행성 담췌관조영술 (ERCP)가 필요하다. 그외 자기공명 담췌관조영술(MRCP), 담관내시경 및 담관세포검사(bile duct cytology)도 담관내 종양인지 담관주위를 침범하거나 담관 밖에서 비롯된 것인 Fig. 1. Abdominal CT findings (A) A huge mass in right liver (about 6 cm in diameter) is seen. (B) Another mass in the confluence
of bile duct is seen. (C) Postoperative CT finding: Rt. Hepatectomy whit no residual mass was done.
Fig. 2. Gross finding of Rt. hepatocellular carcinoma in the section of liver. Multinodular confluent neoplasm replaces most of the right liver with variable bile stained and non-bile stained regions.
Fig. 3. Microscopic findings of hepatocellular carcinoma. (A) At low power view, the section shows moderately well differentiated hepatocellular carcinoma whit trabecular pattern. (H&E stain, ×100). (B) At high power view, the section shows nuclear atypicality and bile production by tumor cells (H&E stain, ×400).
A B
352 대한외과학회지:제 69 권 제 4 호 2005
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 지 규명하는 데 도움을 준다. 가장 간별해야 하는 질환으로
는 간문부 담관암을 들 수 있는데 저자들의 경우에도 CA19-9의 혈중농도와 컴퓨터 단층촬영상 간문부 담관암을 의심하여 수술하였지만 수술 중 종양색전이 간문부 담관을 폐쇄시킨 간세포암으로 확인되었다. 그래서 이와 비슷한 경우에는 수술 전 내시경적 역행성 담췌관조영술(ERCP), 담관내시경(choledochoscopy)을 통한 조직검사를 시행하여 감별해야 할 것으로 생각된다. 치료는 간절제술과 종양색 전 제거술 혹은 간외담관 절제술을 시행하는 경우가 가장 좋다. 그러나 절제율은 상당히 낮다. Chen 등은 약 10%의 절제율을 Lau 등은 18%의 절제율을 보고하였다. 이렇게 절 제율이 낮은 이유는 간경변 및 황달에 의해 악화된 간기능 에 기인한다.(6) 최근에는 경피경간 담즙배액술(PTBD) 등 으로 황달을 호전시킨 후 절제율의 향상을 가져왔다.(6) 간 외 담관의 절제는 종양이 육안적으로 담관을 침범한 경우 는 담관절제를 원칙으로 하지만 대부분의 종양색전은 담관 내에서 완전 제거가 가능하므로 이런 경우는 담관 절제가 필요 없다고 하였다.(5-7) 간의 미상엽 절제에 대한 연구는, Nimura 등(8)은 담관종영술상 간세포암이 우축 후분절의 담관에 종양색전 및 침범되었을 경우는 미상엽 절제를 주 장하였다. Kojiro 등(9)은 대부분의 종양색전이 담관벽에 단 단히 붙지 않고 쉽게 분리가 가능하다고 하였으나 Nishio 등(10)은 이 경우가 주로 간외 담관에서 관찰되며 간내 담 관에는 그렇지 않다고 하여 담관조영술상 미상엽의 담관분 지가 보이지 않을 경우 미상엽 절제를 시행하여야 한다고 하였다.
황달성 간세포암은 예후가 나쁘지만 성공적인 간절제술 이 이루어졌을 경우는 일반적인 간세포암과 생존율에서 차 이가 없다.(11)
결 론
황달성 간세포암에서 보다 정확한 술전 진단과 간기능 보유에 대한 정확한 검사 및 기능 보전으로 간절제술을 통 해 생존율의 향상을 기대할 수 있다. 저자의 경우도 우측 간절제술과 간외담관절제술을 시행하였고 수술 약 9개월 후 간내 재발이 있었으나 현재 경동맥 색전술(TAE)로 1년 이 지나도록 생존하고 있다.
REFERENCES
1) Yoshiaki M, Takashi Y, Tetsuya K, Kenichiro U, Masaru S, Masahiko M, et al. Successful diagnosis and resection of icteric type hepatocellular carcinoma. Hepatogastroenterology 2003;50:1634-6.
2) Mallory TB, Castleman B, Parris EE. Case records of the Massachusetts General Hosipital, case 33441. N Engl J Med 1947;237:673-6.
3) Lin TY, Chen KM, Chen YR, Lin WS, Wang TH, Sung JL.
Icteric type hepatoma. Med Chir Dig 1975;88:267-70.
4) Chen MF, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC.
Obstructive jaundice secondary to ruptured hepatocellular car- cinoma into the common bile duct. Cancer 1994;73:1335-40.
5) Lau W, Leung K, Leung TW, Liew CT, Chan MS, Yu SC, et al. A logical approach to hepatocellular carcinoma pre- senting with jaundice. Ann Surg 1997;225:281-5.
6) Masaya S, Junichi K, Masato N, Katsuhiko U, Tsuyohi S, Naokazu H, et al. Hepatocellular carcinoma with biliary tumor thrombi: aggressive operative approach after appropriate preo- perative management. Surgery 2001;129:692-8.
7) Wang HJ, Kim JH, Kim JH, Kim WH, Kim MW. Hepato- cellular carcinoma with tumor thrombi in the bile duct. Hepato- gastroenterology 1999;46:2495-9.
8) Nimura Y. Surgical anatomy of the biliary ducts. In: Rossi P, editor. Medical Radiology Biliary Tract Radiology. Berlin:
Springer-Verlag; 1997. p.21-30.
9) Kojiro M, Kawabata K, kawano Y, Shirai F, Takemoto N, Nakashima T. Hepatocellular carcinoma presenting as intrabile duct tumor growth. A clinicopathological study of 24 cases.
Cancer 1982;49:2144-7.
10) Nishio H, Miyata K, Hanai M, Kato M, Yoneyama F, Koba- yashi Y. Resection of an icteric type hepatoma with tumor thrombi filling the right posterior bile duct. Hepatogastroen- terology 2002;49:1682-5.
11) Shiomi M, Junichi K, Nagino M. Hepatocellular carcinoma with biliary tumor thrombi: aggressive operative approach after appropriate preoperative management. Surgery 2001;129:
692-8.