A traumatic carotid-jugular fistula with or without a pseudoaneurysm is rare, and generally occurs after a penetrating trauma rather than after blunt trauma. A by- pass graft and sacrifice of the involved carotid artery was originally the treatment of choice until the advent of endovascular method. Currently, a traumatic carotid- jugular fistula can be treated using endovascular meth- ods such as ballooning, coiling, stent-graft deployment and stent assisted coil embolization. The authors present two cases of traumatic carotid - jugular fistula that were treated using endovascular methods.
Case Report
Case 1
A 6-year-old boy was admitted to our hospital with the
chief complain of progressive headache, pulsating mass, and a hard thrill immediately below the right mandible angle for a 3 month duration. He had suffered a deep penetrating neck injury 9 months earlier. 3D CTA and DSA revealed an arteriovenous fistula between the right facial artery to the right retromandibular vein, which drained to the right internal jugular vein (Figs. 1A, B).
Endovascular treatment was planned because this method is less invasive than surgery. Among the en- dovascular methods including coil embolization and bal- loon occlusion, common carotid-jugular fistula coil em- bolization was chosen. The fistula could not be located precisely using external carotid angiography due to the high flow arteriovenous shunt. Therefore, the plan was to occlude the fistula through the venous route using a Gugelielmi detachable coil (GDC; Boston Scientific, Natick, MA). Microcatheters (Prowler 14; Cordis Neurovascular systems, Miami, FL) were inserted into the dilated retromandibular vein through the internal and external jugular vein. Two-dimensional, 20 mm×
Endovascular Treatment of Traumatic Carotid- Jugular Fistula: Report of Two Cases1
Han Won Jang, M.D., Woo Mok Byun, M.D., Jae Woon Kim, M.D., Chul Hoon Chang, M.D.2
1Department of Diagnostic Radiology, Yeungnam University College of Medicine
2Department of Neurosurgery, Yeungnam University College of Medicine Received June 20, 2006 ; Accepted November 14, 2006
Address reprint requests to : Woo Mok Byun, M.D., Department of
We report 2 patients with a traumatic carotid- jugular fistula. The first patient suf- fered a deep neck penetrating injury. The external carotid-jugular fistula was demon- strated by 3-dimension CT angiography (3D CTA) and digital subtraction angiography (DSA). The patient was treated with coil embolization. The second patient suffered a gun shot injury to the neck. 3D CTA and DSA revealed a common carotid-jugular fistu- la and a pseudoaneurysm. The common carotid-jugular fistula was treated with coil embolization in the fistula and the pseudoaneurysm was treated with stent assisted coil embolization .
Index words :Fistula, arteriovenous Neck, injuries
Carotid arteries, interventional procedures
After the blood flow through the fistula had decreased, a total of eleven Tornado platinum coils (A Cook Group Company, Bloomington, IN) were deployed. The total length of the inserted coils was 120 cm. After emboliza- tion, a small amount of the blood flow through the arte- riovenous shunt was remained but the right intracere- bral vascular structures were well visualized (Fig. 1C).
Embolization was stopped due to the expected sponta- neous regression of the fistula. After 3 months, the right carotid angiogram revealed an increased arteriovenous shunt from the right facial artery to the internal jugular vein (Fig. 1D). Therefore, an attempt was made to em-
bolize the arteriovenous fistula through the arterial ap- proach. The microcatheter was inserted into the dilated fistula through the facial artery and embolized with GDCs (18 mm×30 cm, 20 mm×30 cm) and Tornado platinum coils (Total length 54 cm) until the abnormal venous drainage had disappeared (Fig. 1E). There was no evidence of a fistula during the 12-month follow up.
Case 2
A 22-year-old man was admitted due to neck swelling from a gun shot injury. He had no neurologic deficits.
3D CTA and DSA revealed a high flow fistula between
─ 110 ─
A B C
D E
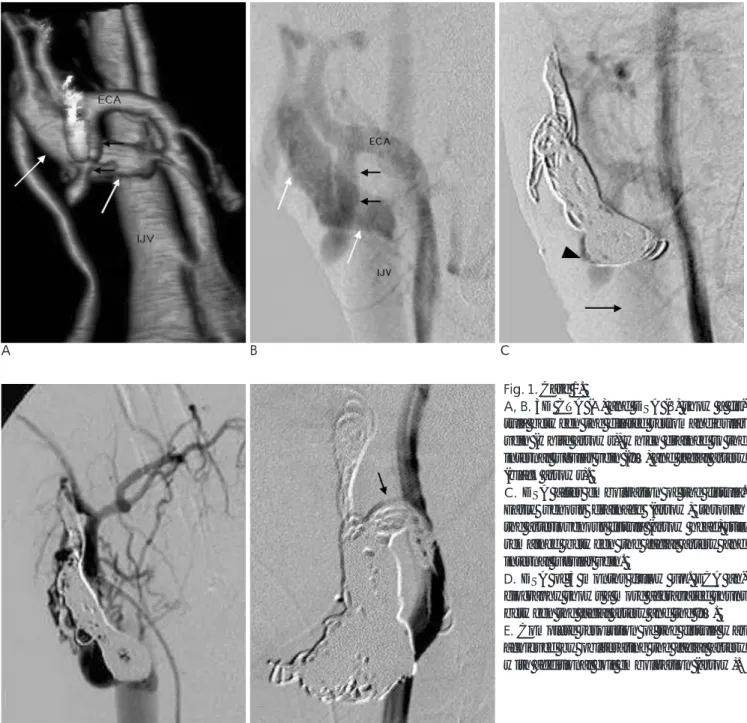
Fig. 1. Case 1.
A, B. 3D CTA (A) and DSA (B) show a fis- tula between the dilated retromandibular vein (white arrows), which drained to the internal jugular vein (IJV) and facial artery (black arrows).
C. DSA after embolization of the fistula.
Early venous drainage (arrow) through the arteriovenous fistula (arrow head) still remained between the facial artery and internal jugular vein.
D. DSA of 3 months follow up. ECA an- giography shows a more aggravated shunt between the facial artery and the IJV.
E. Complete resolution of the fistula was achieved by obliterating the facial artery with additional coil embolization (arrow).
the distal common carotid artery and the internal jugu- lar vein (Figs. 2A, B) and a pseudoaneurysm in the distal common carotid artery immediately above the fistula site (Fig. 2C). The plan was to embolize the fistula and then perform surgery. Using the venous approach, the fistula was treated successfully with four GDCs (Total length 115 cm). However, the surgery failed due to se- vere adhesion adjacent to the common carotid artery.
Stent assisted coil embolization was then performed in- stead of a graft stent due to the uncertain long-term pa- tency and freedom from a restenosis of the graft stent.
First, a microcatheter was placed in the pseudoa- neurysm and then 8 mm×3 cm sized Easy Wallstent (Boston Scientific/Schneider, Minneapolis, MN) was de- ployed. A total of four GDCs (Total length 35 cm) were inserted into the pseudoaneurysm through the micro- catheter until dense coil packing had been achieved (Fig.
2D). After the procedure, the pseudoaneurysm and fis- tula disappeared and the left internal carotid artery flow was well preserved until the 12-month follow up.
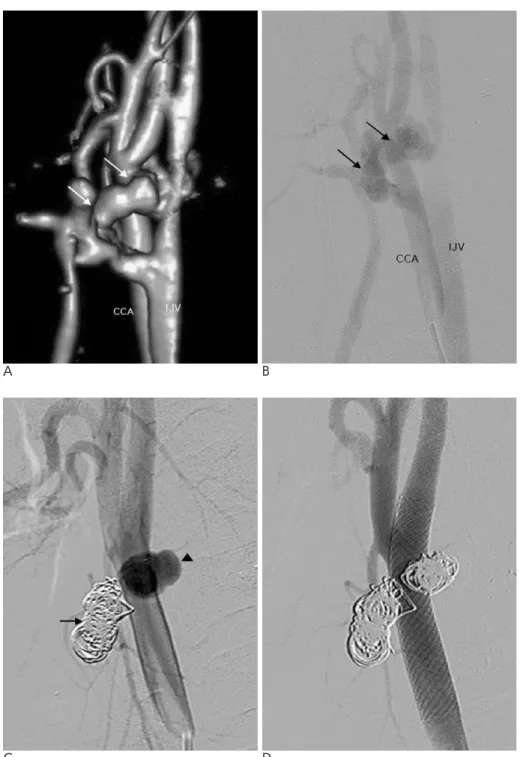
A B
Fig. 2. Case 2. A, B. 3D CTA (A) and DSA (B) reveal a fistula (arrows) be- tween the distal common carotid artery and IJV.
C. DSA after coil embolization of fistu- la. The fistula was obliterated by coil embolization (arrow), but the pseudoa- neurysm still remained (arrowhead).
D. DSA after the stent assisted coil em- bolization shows complete obliteration of the pseudoaneurysm.
Discussion
Penetrating objects such as a bullet or knife passing through or near the neurovascular bundles of the neck can easily damage the blood vessels (1). These injuries can cause acute hemorrhage, complete major vessel ob- struction and the formation of a traumatic aneurysm or arteriovenous fistula (2). If left untreated, the pseudoa- neurysm can cause compressive symptoms and embolic phenomena, and a carotid-jugular fistula usually en- larges and causes severe high output heart failure and obstructive symptoms (3). Conventional angiography is traditionally used to diagnose the injured vessel.
However, a rapid and noninvasive diagnosis of major vessel injuries can be made using helical CT angiogra- phy with a high sensitivity and specificity (4). The aim of a carotid-jugular fistula including a pseudoaneurysm is to occlude the fistula and pseudoaneurysm whilst pre- serving the parent artery. Traditionally, surgery by an excision of the fistula with vascular reconstruction was the treatment of choice for carotid-jugular fistula and pseudoaneurysm. Recently, the development of new de- vices and techniques has enabled the use of endovascu- lar treatments for surgery. These endovascular methods include balloon occlusion (5) and coil embolization for a fistula (6), stent assisted coil embolization for a pseudoa- neurysm and stent-graft insertion either for a fistula and pseudoaneurysm (3, 7-10). These methods have their own advantages and disadvantages. Surgery is a definite method for achieving proximal vascular control of the common carotid artery by isolating the parent artery from the fistula or pseudoaneurysm. However, the pro- cedure carries potential risks, such as cranial nerve in- jury and sternostomy (10). Stent assisted coil emboliza- tion for the treatment of a pseudoaneurysm allows a good packing density compared with simple coiling be- cause the stent prevents the migration or bulging of coils into the parent vessel lumen. On the other hand, there is potential risk of recanalization of the sac due to incom- plete exclusion by the vessel lumen (10). In the case of a carotid-jugular fistula combined with a pseudoa- neurysm, a stent-graft is a promising technology for obliterating a fistula and pseudoaneurysm, and preserv- ing the parent artery with relatively safely (8). However, the long term patency and freedom from a restenosis of
the stent-graft are still unknown. Hence, close observa- tion is needed (9). In the case of an external carotid-jugu- lar fistula, the treatment options are limited to surgery, simple coiling and ballooning. In our case, the external carotid-jugular fistula was treated successfully using de- tachable coils and multiple fibered coils. In our case of a common carotid-jugular fistula combined with a pseudoaneurysm, the common-carotid jugular fistula was obliterated using detachable coils and then the pseudoaneurysm was excluded by stent assisted coil embolization. Both patients suffered no recurrence dur- ing a 12 months follow up.
In conclusion, coil embolization or stent assisted coil embolization can be considered the first line treatment for a traumatic carotid -jugular fistula with or without a pseudoaneurysm.
References
1. Amirjamshidi A, Abbassioun K, Rahmat H. Traumatic aneurysm and arteriovenous fistulas of the extracranial vessels in war in- juries. Surg Neurol 2000;53:136-145
2. Tew JM Jr, Johnson JK, Tomsick TA. Traumatic lesions of the carotid artery. In Smith RR, ed. Stroke and the extracranial vessels.
New York, NY: Raben Press; 1984;307-319
3. Self ML, Mangram A, Jefferson H, Slonim S, Dunn E, Kollmeyer K. Percutaneous stent-graft repair of a traumatic common carotid- internal jugular fistula and pseudoaneurysm in a patient with cer- vical spine fractures. J Trauma 2004;57:1331-1334
4. Mu¨nera F, Soto JA, Palacio D, Velez SM, Medina E. Diagnosis of arterial injuries caused by penetrating trauma to the neck: compar- ison of helical CT angiography and conventional angiography.
Radiology 2000;216:356-362
5. Gobin YP, Garcia de la Fuente JA, Herbreteau D, Houdart E, Merland JJ. Endovascular treatment of external carotid-jugular fis- tula in the parotid region. Neurosurgery 1993;33:812-816
6. Jansen O, Do¨rfler A, Forsting M, Hartmann M, von Kummer R, Tronnier V, et al. Endovascular therapy of arteriovenous fistula with electrolytically detachable coils. Neuroradiology 1999;41:951- 957
7. Ramsay DW, McAuliffe W. Traumatic pseudoaneurysm and high flow arteriorvenous fistula involving internal jugular vein and common carotid artery. Treatment with covered stent and em- bolization. Australas Radiol 2003;47:177-180
8. Ahn JY, Chung YS, Lee BH, Choi SW, Kim OJ. Stent-graft place- ment in a traumatic internal carotid-internal jugular fistula and pseudoaneurysm. J Clin Neurosci 2004;11:636-639
9. Wyers MC, Powell RJ. Management of carotid injuries in a hostile neck using endovascular grafts. J Vasc Surg 2004;39:1335-1339 10. Patel JV, Rossbach MM, Cleveland TJ, Gaines PA, Beard JD.
Endovascular stent-graft repair of traumatic carotid artery pseudoaneurysm. Clin Radio 2002;57:308-311
─ 112 ─
대한영상의학회지 2007;56:109-113
외상성 경동맥-경정맥 누공의 혈관 내 치료: 2 증례 보고1
1영남대학교 의과대학 진단방사선과학교실
2영남대학교 의과대학 신경외과학교실
장한원・변우목・김재운・장철훈2
혈관 내 치료를 시행한 외상성 경동맥 - 경정맥 누공환자 두 증례를 보고하고자 한다. 첫 번째 환자는 경부 심 부 관통상을 가졌으며 삼차원 전산화단층혈관조영술과 디지털감산혈관조영술에서 외경동맥 - 목정맥 누공이 보였 고 코일 색전술로 치료하였다. 두 번째 환자는 경부 총상환자로 삼차원 전산화단층혈관조영술과 디지털감산혈관조 영술에서 총경동맥 - 목정맥 누공과 가성동맥류가 동반되었으며 누공은 코일 색전술로 치료하였고 가성동맥류는 스텐트 보조 코일색전술을 시행하였다.