Clinical Experience of Ultrasound-Guided, Vacuum-Assisted Breast Biopsy for Mammographic Microcalcifications:
Combination with Wire Localization
SeungSang Ko, Man Sik Shin, Ki Won Chun, Kang Young Rhee, Heeboong Park Department of Surgery, Park Surgical Clinic, Suwon, Korea
Received July 9, 2018 Revised August 16, 2018 Accepted October 1, 2018
Purpose: This study examined the usefulness of ultrasound-guided vacuum-assisted breast biopsy (Sono-guided VABB) for mammographic microcalcification.
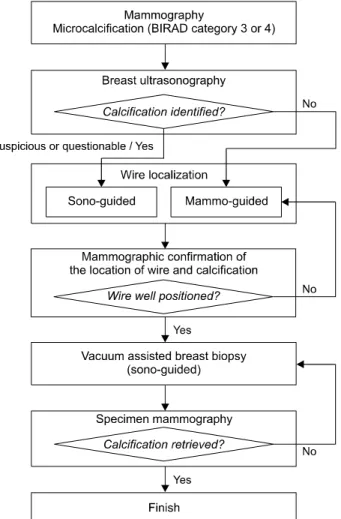
Methods: A total of 1,399 lesions of 1,364 patients with BI-RADS Category 4 Mammo- graphic microcalcification were included. Most microcalcifications were not observed on ul- trasound (99.4%). Sono-guided (or Mammo-guided) J-wire localization was first performed for the suspicious microcalcification area, and the location of the J-wire and calcification was determined with mammography in most cases (98.5%). Sono-guided VABB was per- formed after removing the J-wire without a stereotactic device. On the other hand, Sono-guided VABB was performed directly without J-wire localization when micro- calcification lesions were identified by mass on ultrasonography (21 cases, 1.5%). In all cas- es, calcification was confirmed by specimen mammography and the pathology was performed. A follow-up examination was performed to confirm the presence of com- plications.
Results: In 1,399 cases, 188 cases (13.4%) were diagnosed as a malignancy (153 cases of ductal carcinoma in situ, 32 cases of IDC and 3 cases of other cases). The remaining 1,211 cases (86.6%) were diagnosed as benign. There were no significant complications during fol- low up after VABB.
Conclusion: Sono-guided VABB can be used effectively if combined with wire localization, even if mammographic microcalcification lesions are not fully identified by ultrasonography.
Keywords: Mammography, Calcification, Ultrasonography, Image-guided biopsy Correspondence to:
Heeboong Park
Department of Surgery, Park Surgical Clinic, 203, Geowerk, 7 Hyowon-ro 256-gil, Gwonseon-gu, Suwon 16571, Korea
Tel: +82-31-233-5571 Fax: +82-31-233-5955 E-mail: [email protected]
INTRODUCTION
Well-qualified mammography has the best sensi- tivity for early detection of nonpalpable breast can- cer, but the specificity is low, and about 10% of breast cancers are not found in mammography.(1) Biopsy is usually required to make definite diagnosis of nonpalpable lesions detected by mammography.
But, most of the microcalcifications on mammog- raphy are not or are barely visible on ultrasound
imaging. Therefore, excisional biopsy or vacuum as- sisted core biopsy under stereotactic or mammog- raphy-guided wire localization is usually performed for those lesions.(2-7)
Ultrasonography is limited for detecting micro- calcifications, which is due to low contrast reso- lution; however, ultrasonography detects micro- calcifications associated with other findings, such as mass or ductal changes.(8-10) In general, patients prefer ultrasound-guided (Sono-guided) procedures J Surg Ultrasound 2018;5:53-60
https://doi.org/10.46268/jsu.2018.5.2.53 JSUJournal of Surgical Ultrasound
Fig. 1. Flowchart of patients undergoing Sono-guided VABB with J-wire localization in our clinic.
to mammography-guided (Mammo-guided) proce- dures, as patients tend to be more comfortable with the supine position, breast is not compressed, and the procedure is less time-consuming. In addition, no ionizing radiation is used, the needle insertion site is more flexible, and real-time observations can be made.(11,12) For these reasons, Sono-guided core needle biopsy (CNBx) or vacuum-assisted breast bi- opsy (VABB) are most frequently used for micro- calcifications identified on ultrasonography.(9,13-18) Although the combination of a VABB and a prone-type biopsy table with stereotactic attach- ment is preferred biopsy procedure, such devices are quite expensive and sophisticated. Most small hospi- tals and private clinics are unable to these devices, especially those in which medical expenses are strictly regulated by the government such as Korea and Japan. Another way to perform stereotactic bi- opsies without a stereotactic prone table is to use a Sono- or Mammo-guided J-wire localization instead.
However, only a limited number of reports with a small number of patients have been published re- garding the results of using this method with VABB.(9,12) Therefore, the value of Sono-guided VABB for mammographic calcification has not been validated yet. We reported our initial experience us- ing this procedure on 2005.(19) This article reports our 14-year experience with about 1,400 cases.
METHODS
A total of 1,364 patients were classified under Breast Imaging Reporting and Data System (BI-RADS) category 4 between January 2004 and March 2018 at our clinic (Park Surgical Clinic, Suwon, Korea). Microcalcifications were classified on mammograms immediately by Surgeons. The Mammographic calcification was categorized as probably benign (BI-RADS 3), suspicious (BI-RADS 4) or highly suggestive of malignancy (BI-RADS 5)
despite of subcategorization of BI-RADS 4 (4a, 4b, 4c). Category 4 subdivisions does not used in our study. All these category 4 cases were recommended for biopsy.
We evaluated whether suspicious microcalci- fications were visible by ultrasonography and feasible to biopsy under Sono-guidance. The biopsy proce- dures were described previously (Fig. 1).(19) All pa- tients were biopsied with Sono-guided VABB in a su- pine position without stereotactic device. In case of the microcalcifications were clearly visible on ultra- sonography, Sono-guided VABB was performed di- rectly without wire-localization. However, most of the microcalcifications were just suspicious or were
not clearly identified in the ultrasonography. In most of these cases, the J-wire was inserted after local anesthesia with 2% lidocaine under ultrasound guidance. The location of the wire was positioned at the suspicious site of microcalcification. The location of the wire was confirmed to be on the target by the mammography. An image with the two spot images was utilized to localize the precise position of the microcalcification and J-wire. If the position of the wire is different from the calcification position, an- other J-wire was inserted several times more after local anesthesia to determine the position (average 1.4 times, 1-5 times).
When the wires were well positioned corelated with location of calcification, the VABB probe was inserted along the hyperechogenic shadow(s) of J-wire on ul- trasound image, and VABB was performed after re- move the J-wire(s). The VABB was performed under Sono-guided handheld technique. All the tissues ob- tained by VABB were examined by specimen mam- mography to confirm microcalcification. The VABB probe was not removed until calcification was retrieved. If calcification was not retrieved, VABB was repeated to the surrounding area. After biopsy, hemostasis was conducted by compressing the breast with hand for 5-10 min and elastic bandage was applied.
Many experienced surgeons did this method for 14 years, but the corresponding author, who is a presi- dent of this clinic did this procedure in most cases.
We usually spent about 30 minutes to complete a bi- opsy procedure. The presence of microcalcification was confirmed radiographically by taking an X-ray image of the obtained biopsy materials. Biopsy fail- ure was defined as technical failure of targeting or sampling of microcalcifications because of absence of calcification on specimen mammography.
If the pathological diagnosis was atypical ductal hyperplasia (ADH), generally no further surgical bi- opsy was performed except for large diffuse lesions.
Follow-up examination was performed after 3 and 6 months. If a diagnosis of cancer was made, definitive surgery was performed.
Oral informed consent was obtained from all biop- sied patients.
The localization J-wire needle was a 20 G, 7.5 cm Homer MammalokⓇ (Medical Device Technologies, PA, USA) and 7.5 cm CalocⓇ (Medical Park Inc., Yongin-si, Gyeonggi-do, Korea). In early days of the study we used MammalokⓇ, but we are currently us- ing the CalocⓇ only recently. The ultrasound equip- ment used a high-resolution close-range ultrasound (Philips Ultrasound, USA) with a 5-12 MHz linear transducer. VABB equipment used MammotomeⓇ (Devicor Medical Products, Cincinnati, OH, USA) un- til June 2014 (908 cases), and since then BexcoreⓇ (Medical Park, Yongin-si, Gyeonggi-do, Korea) has been used (491 cases) only.
RESULTS
The average age of patients from whom the tissues were actually obtained was 44.5 years (range 20-75 years). 740 lesions (52.9%) in left breasts, 659 le- sions (47.1%) in right breast.
In only 8 out of 1,399 lesions, calcification was well observed within associated mass or dilated ducts. In most cases (1,391 cases), calcification was not ob- served at ultrasound image (just suspicious micro- calcification lesion in 804 cases).
In most cases (1,358 cases), J-wire were inserted under Sono-guided initially (Fig. 2), and 28 cases were converted to Mammo-guided because the posi- tion of wire did not match the position of calcification.
However, in 41 cases in which microcalcification was not identified in ultrasonography and not suitable for Sono-guided localization, J-wire was inserted under Mammo-guided from the beginning (Fig. 3, 4). The average number of J-wire insertion to acquire mi- crocalcification in the VABB specimen per biopsy was
Fig. 2. Fibrocystic change with cal- cifications in a 37-year-old woman.
Fig. 3. 36-year-old female patient who underwent screening mammo- graphy.
Fig. 4. Fibrocystic change with cal- cifications in a 41-year-old woman.
Table 1. Pathological Diagnoses
Diagnosis Cases (%)
Benign, n=1211 (86.6%)
Fibrocystic disease 991 (70.8)
Fibroadenoma 105 (7.5)
Mucocele like tumor 46 (3.3) Intraductal papilloma 25 (1.8) Atypical ductal hyperplasia 14 (1.0)
Duct ectasia 12 (0.9)
Others 18 (1.3)
Inflammation 3
Hamartoma 2
Fat 2
Hemangioma 1
Lipoma 1
Sclerosing adenosis 1
Adenosis 1
Tubular adenoma 1
Etc. 6
Malignancy, n=188 (13.4%)
Ductal carcinoma in situ 153 (10.9) Invasive ductal carcinoma 32 (2.3) Lobular carcinoma in situ 2 (0.1) Mucinous carcinoma 1 (0.1)
Total 1,399
1.4 (range 0-5). Microcalcifications were confirmed radiographically in the obtained tissue of 1,360 (97.2%) of 1,399 biopsies in which the tissue from le- sions with microcalcifications. The 39 cases (2.8%) The pathological diagnoses of VABB were as follows (Table 1). Among 1,399 diagnoses, 33 were invasive cancer, 155 were carcinoma in situ, and 1,211 were benign disease (including ADH in 14). Among the le- sions diagnosed as benign diseases, except for ADH, we found 46 mucocele-like tumors and 25 intraductal papilloma. Although those lesions are now regarded as high risk, we did not perform surgical biopsies for them. Out of 153 lesions diagnosed as DCIS by VABB biopsy, 3 invasive cancers were found on another quadrant of the breast after definitive mastectomy.
Finally, 188 (13.4%) lesions were diagnosed as ma- lignant (32 invasive ductal carcinomas, 153 DCISs, 2 lobular carcinoma in situ, 1 mucinous carcinoma), while 1,211 were benign (including 14 ADHs).
All 1,211 benign lesions were not removed surgi- cally shortly after the VABB, but were follow up at least once by palpation, mammography and ultraso-
nography. No cancers developed from the lesions that were diagnosed as ADH by VABB but not surgically biopsied, and from those of other types with high
risk. All these benign cases were followed up every 6 months or every year for mammography and ultra- sonography. There were no abnormal findings or ma- lignant tumors to date.
DISCUSSION
The purpose of screening mammography is de- tection of early stage breast cancers that are usually nonpalpable. As the majority of very early breast cancers do not show mammographic and sonographic findings typical of cancers, it is usually necessary to perform biopsy and make a histological diagnosis for mammographically detected suspicious lesions. The common methods to perform biopsy for lesions with microcalcifications are stereotactic core needle biop- sy (including VABB) and surgical excision under lo- calization (mammography guided).
Currently, many papers regarding stereotactic VABB using a prone table have shown outstanding results.(4,6,20-22) However, several problems re- main, including the high cost of prone tables. Another problem is the large space required for the prone ta- ble, even though it cannot be used for examinations other than breast needle biopsy. Even if the up- right-type stereotactic add-on unit has helped to overcome these drawbacks, the combination with a mammography unit and wire is adaptable to local- ization of microcalcification for VABB.
It is still unclear whether the combination of the Sono-guided VABB and wire-localization is practi- cally feasible, and the diagnoses made with the tissue thus obtained with the combination are correct.
Currently, a very limited number of reports with a small number of patients have been published re- garding this combination. Its value must thus be confirmed, especially when using a localization wire.
The present report has shown our 14-year experience of about 1399 biopsies with this combination, and this is the largest number reported among those us-
ing the localization wire and Sono-guided VABB.
The retrieval rate of the microcalcifications (97.2%) from the microcalcified lesions in this combination was comparable to those in previous studies.
(6,9,14,15,18,22) The time required for this proce- dure was 30-40 minutes per biopsy. We therefore can conclude that the combination of a Sono-guided VABB and a Wire-localization without stereotactic device is feasible. We conclude that the accuracy of the biopsy performed with the combination of the VABB and wire-localization is acceptable.
The 39 biopsy failure cases (2.8%) were technically infeasible. Previous studies reported technical feasi- bility rates of 93-99% (23-25) and vasovagal re- action rates of 0-2% in the prone position.(6,23) The biopsy failure rate for Stereotactic-guided VABB can differ according to patient’s position. The prone po- sition, which is used in most institutions, is reliable and accurate but requires significant space and is relatively expensive. Some institutions prefer the sitting or decubitus position, but they can present problems due to the relatively high frequency of vas- ovagal reactions and patient’s motion.(23,26,27) Digital breast tomosynthesis-guided biopsies are performed at some institutions using the lateral de- cubitus position, and a higher biopsy success rate in less procedure time was reported compared with prone.(25)
The complications we experienced consisted mainly of subcutaneous bleeding with or without hematoma.
The risk of subcutaneous bleeding is thought to be the same between the stereotactic prone tables and this our method. All the bleeding cases we experi- enced were self-limited.
The calcification lesions associated with mass might have been biopsied by a Sono-guided approach in a way that was less stressful to the patients than the stereotactic approach. Among the all 1,399 calci- fication lesions, most of them (1,391 cases, 99.4%) were not well identified by ultrasonography. However,
804 cases were identified as suspicious calcification on ultrasonography.
There are some limitations in this report. First, this study was performed as a part of clinical practice in a single center, not as a protocol study. Also, all procedures including mammography reading, ultra- sonography, and J-wire localization were performed by experienced surgeons only. Further study with a larger number of patients from multiple centers is needed to compare the overall diagnostic outcomes of the various biopsy methods. Second, breast ultra- sonography is an operator dependent procedure and reproducibility is dependent on individual skill of the doctor. Inter-operator variability was not evaluated in this study.
CONCLUSION
In conclusion, the Sono-guided VABB technique using the combination of the wire-localization with- out a stereotactic system is cost- and space-effec- tive, safe and accurate, and it should be regarded as one of the standard biopsy methods for mammo- graphically detected microcalcifications.
CONFLICTS OF INTEREST
Corresponding author, Dr. Heeboong Park is a de- veloper of BexcoreⓇ system and CalocⓇ device, and Chief Executive Officer of Medical Park Inc.
REFERENCES
1. Smith RA, Saslow D, Sawyer KA, Burke W, Costanza ME, Evans WP 3rd, et al. American Cancer Society guidelines for breast cancer screening: update 2003.
CA Cancer J Clin 2003;53:141-69.
2. Anania G, Bazzocchi M, di Loreto C, Risaliti A, Terrosu G, Donini A, et al. Percutaneous large core needle biopsy versus surgical biopsy in the diagnosis of breast lesions. Int Surg 1997;82:52-5.
3. Parker SH, Klaus AJ. Performing a breast biopsy with a directional, vacuum-assisted biopsy instrument.
Radiographics 1997;17:1233-52.
4. Liberman L, Smolkin JH, Dershaw DD, Morris EA, Abramson AF, Rosen PP. Calcification retrieval at stereotactic, 11-gauge, directional, vacuum-assisted breast biopsy. Radiology 1998;208:251-60.
5. Zannis VJ, Aliano KM. The evolving practice pattern of the breast surgeon with disappearance of open bi- opsy for nonpalpable lesions. Am J Surg 1998;176:
525-8.
6. Kettritz U, Rotter K, Schreer I, Murauer M, Schulz- Wendtland R, Peter D, et al. Stereotactic vacuum-as- sisted breast biopsy in 2874 patients: a multicenter study. Cancer 2004;100:245-51.
7. Golub RM, Bennett CL, Stinson T, Venta L, Morrow M. Cost minimization study of image-guided core bi- opsy versus surgical excisional biopsy for women with abnormal mammograms. J Clin Oncol 2004;22:2430-7.
8. Park JS, Park YM, Kim EK, Kim SJ, Han SS, Lee SJ, et al. Sonographic findings of high-grade and non-high-grade ductal carcinoma in situ of the breast. J Ultrasound Med 2010;29:1687-97.
9. Soo MS, Baker JA, Rosen EL. Sonographic detection and sonographically guided biopsy of breast micro- calcifications. AJR Am J Roentgenol 2003;180:941-8.
10. Yu PC, Lee YW, Chou FF, Wu SC, Huang CC, Ng SH, et al. Clustered microcalcifications of intermediate concern detected on digital mammography: ultra- sound assessment. Breast 2011;20:495-500.
11. Parker SH, Burbank F. A practical approach to mini- mally invasive breast biopsy. Radiology 1996;200:11-20.
12. Soo MS, Baker JA, Rosen EL, Vo TT. Sonographically guided biopsy of suspicious microcalcifications of the breast: a pilot study. AJR Am J Roentgenol 2002;
178:1007-15.
13. Cho N, Moon WK, Cha JH, Kim SM, Jang M, Chang JM, et al. Ultrasound-guided vacuum-assisted biopsy of microcalcifications detected at screening mam- mography. Acta Radiol 2009;50:602-9.
14. Kim HS, Kim MJ, Kim EK, Kwak JY, Son EJ, Oh KK.
US-guided vacuum-assisted biopsy of microcalci- fications in breast lesions and long-term follow-up results. Korean J Radiol 2008;9:503-9.
15. Yi J, Lee EH, Kwak JJ, Cha JG, Jung SH. Retrieval rate and accuracy of ultrasound-guided 14-G semi- automated core needle biopsy of breast microcal- cifications. Korean J Radiol 2014;15:12-9.
16. Parker SH, Klaus AJ, McWey PJ, Schilling KJ, Cupples TE, Duchesne N, et al. Sonographically guid- ed directional vacuum-assisted breast biopsy using a handheld device. AJR Am J Roentgenol 2001;177:
405-8.
17. March DE, Coughlin BF, Barham RB, Goulart RA, Klein SV, Bur ME, et al. Breast masses: removal of all US evidence during biopsy by using a handheld vac- uum-assisted device--initial experience. Radiology 2003;227:549-55.
18. Hahn SY, Shin JH, Han BK, Ko EY. Sonographically- guided vacuum-assisted biopsy with digital mam- mography-guided skin marking of suspicious breast microcalcifications: comparison of outcomes with stereotactic biopsy in Asian women. Acta Radiol 2011;
52:29-34.
19. Kim YM, Park HB, Ryu JW. Usefulness of ultra- sound-guided mammotome biopsy for microcalcification.
J Korean Radiol Soc 2005;53:129-35.
20. Pfarl G, Helbich TH, Riedl CC, Wagner T, Gnant M, Rudas M, et al. Stereotactic 11-gauge vacuum-as- sisted breast biopsy: a validation study. AJR Am J Roentgenol 2002;179:1503-7.
21. Rao A, Parker S, Ratzer E, Stephens J, Fenoglio M.
Atypical ductal hyperplasia of the breast diagnosed by 11-gauge directional vacuum-assisted biopsy. Am J Surg 2002;184:534-7.
22. Jackman RJ, Marzoni FA Jr, Rosenberg J. False-neg- ative diagnoses at stereotactic vacuum-assisted nee- dle breast biopsy: long-term follow-up of 1,280 le- sions and review of the literature. AJR Am J Roentgenol 2009;192:341-51.
23. Wunderbaldinger P, Wolf G, Turetschek K, Helbich TH. Comparison of sitting versus prone position for stereotactic large-core breast biopsy in surgically proven lesions. AJR Am J Roentgenol 2002;178:
1221-5.
24. Jackman RJ, Rodriguez-Soto J. Breast micro- calcifications: retrieval failure at prone stereotactic core and vacuum breast biopsy--frequency, causes, and outcome. Radiology 2006;239:61-70.
25. Schrading S, Distelmaier M, Dirrichs T, Detering S, Brolund L, Strobel K, et al. Digital breast tomosyn- thesis-guided vacuum-assisted breast biopsy: initial experiences and comparison with prone stereotactic vacuum-assisted biopsy. Radiology 2015;274:654-62.
26. Jung YJ, Bae YT, Lee JY, Seo HI, Kim JY, Choo KS.
Lateral decubitus positioning stereotactic vac- uum-assisted breast biopsy with true lateral mammography. J Breast Cancer 2011;14:64-8.
27. Welle GJ, Clark M, Loos S, Pauls D, Warden D, Sheffield M, et al. Stereotactic breast biopsy: re- cumbent biopsy using add-on upright equipment. AJR Am J Roentgenol 2000;175:59-63.