Feasibility and Safety of Single-Port Video-Assisted Thoracic Surgery for Primary Lung Cancer
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치
+2
관련 문서
[6] Thus, we speculated that super ficial SAPB could provide a more effective intraoperative pain control than deep SAPB during video-assisted thoracic surgery
Video-assisted thora- coscopic management of recurrent primary spontaneous pneu- mothorax after prior talc pleurodesis: a feasible, safe and efficient treatment
Serratus anterior plane block or thoracic paravertebral block for postoperative pain treatment after uniportal video-assisted thoracoscopic surgery: a
All patients received operation under a standard general an- esthesia protocol, with single lung ventilation by a double-lu- men endotracheal tube. VATS lobectomy
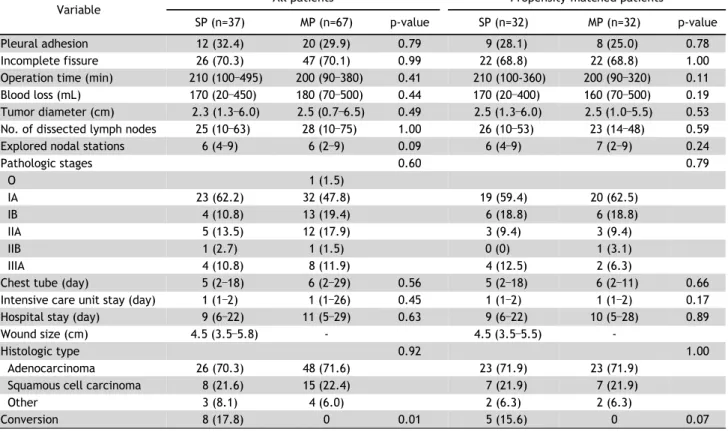
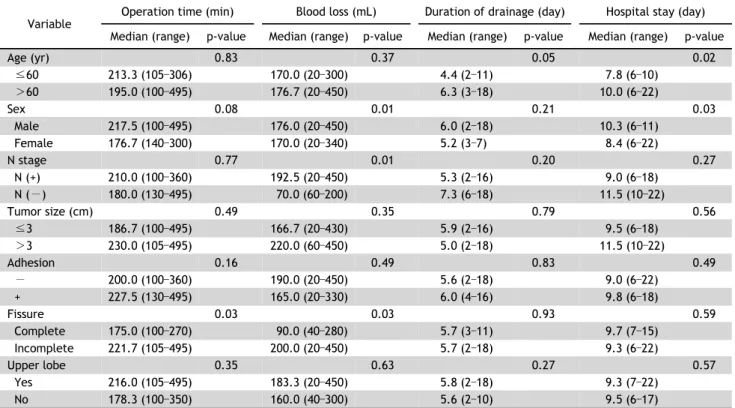
Both groups were compared in terms of the operation time, number of wedge resections, amount of chest tube drainage during the first 24 hours after surgery,
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License
In order to evaluate the feasibility of sin- gle-port VATS for SSP, the postoperative results of single-port VATS (n=15) in patients with emphysema were compared with those
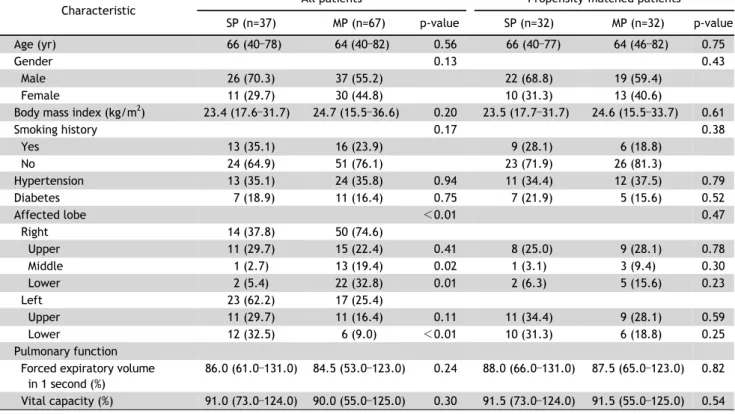
Background: We evaluated the feasibility and outcomes of pulmonary resection and mediastinal node dis- section (MND) by video-assisted thoracoscopic surgery (VATS)
