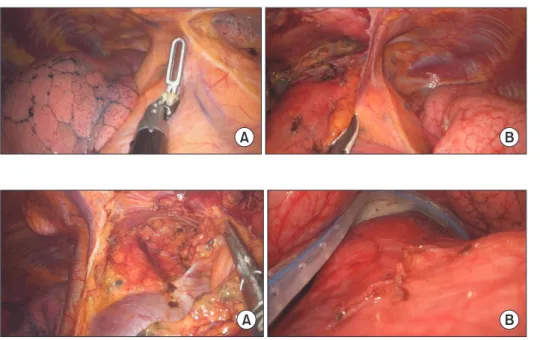
Video-Assisted Thoracic Surgery Thymectomy: Subxiphoid Approach
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치

관련 문서
In this paper, we investigate the differential game theoretic approach for distributed dynamic cooperative power control in cognitive radio ad hoc networks (CRANETs).. First,
In this regard, I would like to request your full cooperation to Kangnam University when they contact you regarding the verification of enrollment
In this regard, I would like to request your full cooperation to Kangnam University when they contact you regarding the verification of enrollment
It considers the energy use of the different components that are involved in the distribution and viewing of video content: data centres and content delivery networks
Pathology, Internal Medicine, Neuroscience, Psychiatry, Pediatrics, Dermatology, Surgery, Thoracic and Cardiovascular Surgery, Neurosurgery, Orthopedic Surgery,
The purpose of this study is to investigate the effect of video- conferencing(VC) English class on affective domains of elementary school students.. They
This paper is written to find answers of the research question that the 'Meeting First, Key-issue Agreement Later" approach of the US and South Korea
Patient had laparoscopic surgery on the adnexal tumor and excised tissue was removed through Douglas pouch incision by single surgeon.. Results: The mean age
