J Korean Neurosurg Soc/Volume 30/October, 2001 1241 KISEP Case Reports J Korean Neurosurg Soc 30::::1241-1244, 2001
척수 신경초종을 동반한 결핵성 척추염 1례
- 증 례 보 고 -
성균관대학교 의과대학 마산삼성병원 신경외과학교실
박종훈·김규홍·이운기·최정훈·이인창·배상도
=
=
=
= Abstract ====
A Case of Tuberculous Spondylitis Combined with Schwannoma of Spinal Cord
- A Case Report -
Jong Hoon Park, M.D., Kyu Hong Kim, M.D., Woon Gi Lee, M.D., Jeong Hoon Choi, M.D., In Chang Lee, M.D., Sang Do Bae, M.D.
Department of Neurosurgery, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, Masan, Korea
he authors report a very rare case of tuberculous spondylitis combined with a schwannoma of spinal cord. A 39- year-old man was admitted because of paraparesis(G1/G2). MRI showed severe cord compression at two different levels. One was by the bulged soft tissue and subligamentous abscess extending from T7 to T9 and the other was by an intradural extramedullary cord tumor at the level of T1-2. At first operation, T8 corpectomy and T7-9 plate fixation with autogenous iliac bone graft were performed. After then, Paraparesis was improved(G2/G3) postoperatively. The second operation underwent two weeks later. The tumor was totally removed and shortly after second operation, paraparesis was markedly improved(G3/G4). Histological diagnosis were tuberculous spondylitis and schwannoma, respectively. The authors reviewed this case where good surgical outcome was obtained by two stage operation.
KEY WORDS:Tuberculous spondylitis・Schwannoma・Paraparesis・Two stage operation.
서 론
결핵성 척추염은 결핵성 질환의 약 1%를 차지하며1)12), 과거 흔한 질환의 하나 였으나 효과적인 결핵 치료후 그 발 생이 크게 감소하였다. 신경초종은 척추강내 종양중 가장 많 은 발생 빈도를 보이며 주로 경막내수외에 발생하는 종양
이다7)20). 신경초종은 주로 단일병변으로 발생하며, 결핵성
척추염과 동반되어 발생한 증례 보고는 아직 없다. 본 교실 에서는 제 7, 8, 9 흉추부에 결핵성 척추염을 가진 환자가 상부 흉추에 척수 신경초종을 동반하였고 이 두 질환 모두 가 척수를 압박하여 신경학적 증상을 일으키는데 관여한 경 우를 치료, 경험하였기에 문헌 고찰과 함께 보고하고자 한다.
증 례
39세 남자 환자로 내원 1개월전부터 배부통이 있다가 갑
자기 일어난 하지마비를 주소로 내원하였다. 과거력상 결 핵이나 종양성 병변, 수술 병력 및 가족력에서도 특이 소견 은 없었다. 이학적 검사상 전반적인 건강상태는 양호한 편 이었으나 최근 1개월간 약 3kg의 체중 감소가 있었다. 흉부 청진 소견상 우측 하부 폐야에서 호흡성 습성 나음(moist rale)이 청진되었고, 우측 제 9 늑골간 아래로 타진음이 감 소한 소견을 보였다. 신경학적 검사상 하지 근력이 G1/G2 였으며 흉추 8번 신경절이하 감각저하 및 배뇨장애가 관찰 되었고, 심부 건반사는 정상이었으며 병적 반사는 관찰되 지 않았다. 일반혈액 검사상 적혈구 침강속도가 54mm/hr 로 증가되어 있었고, 백혈구가 55.000/μl으로 증가되어 있 었다. 다른 혈액 화학검사, 뇨검사, 혈청검사, 심전도 등의 기본검사는 모두 정상이었다. 객담검사상 결핵균은 관찰할 수 없었다. 흉부 X-선 촬영상 우측 폐상부에 석회화 결절 이 관찰되었으며 우측 늑골 횡격각의 둔감이 관찰되었다. 흉 부 전산화 단층 촬영상 우측 상엽에 2×3cm의 고음영 결
TTTT
척수 신경초종을 동반한 결핵성 척추염 1례
J Korean Neurosurg Soc/Volume 30/October, 2001 1242
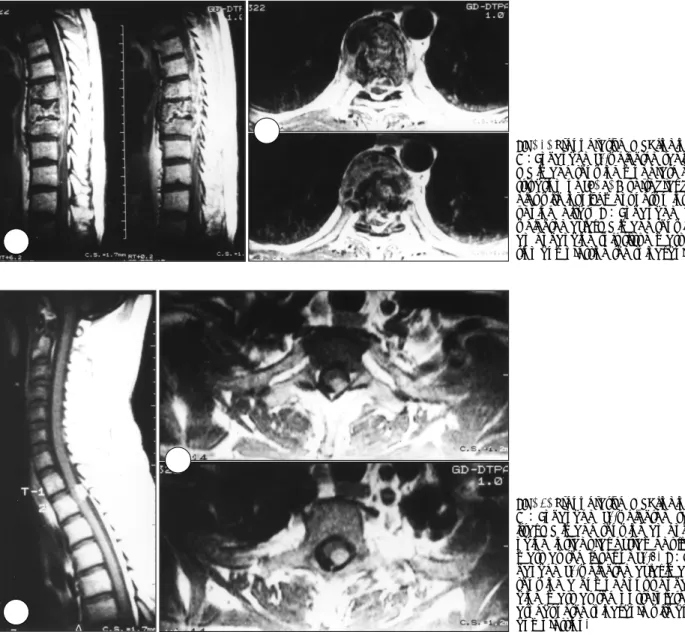
절과 주위에 집합 임파선(conglomerated lymph node)이 관찰되어 활동성 폐결핵이 의심되었다. 흉추 단순 X-선 촬 영상 제 8 흉추체의 골피질 손실 및 그 상하 추체의 일부 골경화 소견이 보였으며 제 7-8, 8-9 흉추간 추간판 간격 의 협소화가 관찰되었다. 흉추부 전산화 단층 촬영상 제 7, 8, 9 흉추체의 불규칙한 골피질의 소실과 골경화 소견이 보 였다. 척추 자기 공명영상에서 또한 제 7, 8, 9 흉추체 골피 질의 소실 및 추간판의 심한 파괴를 보였으며 연부조직 및 인 대하 농양으로 인한 척수의 심한 압박이 관찰되었다(Fig. 1).
제 1-2 흉추부에는 난원형의 경막내수외 종양이 보였으며 척수의 후면에서 척수를 압박하고 있었다(Fig. 2).
수술은 2주 간격으로 두차례 시행하였다. 1차 수술은 결 핵성 척추염을 전방경유 척수 감압술 및 기구 사용 추체 유 합술 시행하였으며 수술 후 하지근력이 G2/G3로 호전을 보
였다(Fig. 3). 1차 수술 2주 후 제 1~2 흉수 사이에 있는 1×
1×1.5cm 크기의 경막내수외 척수종양을 제거하였다. 2차 수술 후 환자의 하지근력이 G3/G4로 호전되는 것을 관찰 할 수 있었다. 수술후 18개월간 항결핵 화학 요법 및 조기 운동 요법을 시행하였으며 3개월만에 보행기 도움없이 걸 을 수 있을 정도로 하지근력의 호전을 보였고 추적 검사한 CT 및 MRI에서 제 7, 8, 9 흉추부에 골유합이 잘 이루어졌 고(Fig. 3) 상부 흉추부의 척수 종양이 완전히 적출된 소견 을 보였다.
1차 수술에서 얻은 조직 병리 소견에서 전형적인 건락 성괴사와 그 주위로 유상피세포, Langhans 거대세포, 임파 구가 둘러싸는 결핵성 병변의 소견을 보였다(Fig. 4). 2차 수술로 제거된 종양의 조직 병리 소견에서 세포핵은 난원형 으로 호산성으로 염색이 되는 색화체를 가지고 있었고 An-
Fig. 1. Preoperative MRI findings.
A:Enhanced T1-weighted sagittal MR image showing moderate de- struction of T7, 8, 9 vertebral bo- dies with involvement of two inter- vening discs. B:Enhanced T1- weighted axial MR image showing an enhancing soft tissue mass le- sion compressing the spinal cord.
A AA A
BBB B
AA AA
BBB B
Fig. 2. Preoperative MRI findings.
A: Enhanced T1-weighted sag- ittal MR image showing an enha- ncing intradural extramedullary mass at the level of T1-2. B:En- hanced T1-weighted axial image showing a homogenous enhan- cing mass at the posterolateral aspect of the spinal cord with cord compression.
박종훈·김규홍·이운기·최정훈·이인창·배상도
J Korean Neurosurg Soc/Volume 30/October, 2001 1243
toni A형과 Antoni B형을 모두 포함하고 있는 신경초종으 로 진단되었다(Fig. 5).
고 찰
척수의 신경초종은 척수종양중 25%라는 가장 많은 빈도 로 발생하며 양성으로 서서히 자라고 원칙적으로 신경초 세 포로 구성되어 있는 국한성 피낭성 종양이다7)20). 척수 신 경초종의 호발연령은 25~40세이며 척추내의 호발 부의는 흉추부, 경추부, 요추부 순이다. 대체로 2/3에서 경막내 척 수외에 발생하며 척수내의 신경초종은 대단히 드문 것으로
알려져 있다7)9)11)17)18)20)
.
결핵성 척추염은 전체 결핵 환자의 1% 정도로 큰 비중 은 차지하지 않지만1)12), 골파괴에 의한 척추동통 및 척추 변형을 일으키고 심한 경우 경막외 농양이나 부골이 척수를 압박하여 하지마비를 초래하는 질환으로 적극적인 치료가 요구되고 있다3)13). 대부분 흉추 하부 및 요추에 발생하고, 약 3~5% 정도에서만 경추에 발생하는 것으로 알려져 있 으나4)6), 최근에는 면역억제 환자, 후천성 면역 결핍증 유행 군에서 경추 발생 빈도가 증가하고 있다고 한다2)14).
척수 종양 및 척추 감염시 가장 심각한 합병증은 하반신 마비로, 특히 흉추부는 척수관이 좁고 척수가 척수관 내에 서 차지하는 비율이 높으며, 정상적으로 후만이 되어 있고 A
AA
A BB BB
Fig. 3. Thoracolumbar AP and la- teral radiographs taken 6 months after operation demonstrating no further erosion of vertebral bodies and the firmly fused iliac bone strut with metallic plate and screws at the right side of T7, 8, 9 bodies.
Fig. 4. Photomicrograph showing several variable sized granulo- matous lesions, having caseous necrosis(large black arrows), peripheral epitheloid cells(small black arrows) and a Lang- hans giant cell(white arrow)(H & E, ×200).
Fig. 5. Photomicrograph showing compact spindle cells with storiform pattern and several verocay bodies(arrows), indicating schwannoma(H & E, ×200).
척수 신경초종을 동반한 결핵성 척추염 1례
J Korean Neurosurg Soc/Volume 30/October, 2001 1244
척수에 대한 혈류 공급이 타 부위만큼 풍부하지 못하기 때문 에 이 부위에 발생시 하반신 마비가 호발 한다고 한다3)13)19). 본 증례에서도 흉추부에 척수 종양 및 척추감염이 발생하 였으며 심각한 하지마비 증세를 보였다.
결핵성 척추염의 수술요법의 적응증은 신경학적 장애, 척 추 불안정성, 약물요법의 실패, 연부조직 농양의 증상이 심 한 경우 등이며 가장 좋은 수술적 치료법은 전방 감압 및 골융합이라고 하며8)15)16), 저자등도 이 방법을 선택하여 좋 은 결과를 얻었다.
결핵의 특징적인 조직학적 소견은, 결핵 결절의 형성과 건 락성 괴사(caseation necrosis)이다. 전형적인 결핵 결절 은 1~2개의 Langhans 거대 세포를 중심으로 그 주위에 유 상피 세포 및 임파구가 운집해 있고 섬유 조직이 둘러싸고 있다13). 신경초종은 조직학적으로 신경초로 구성된 섬유성 피막에 의해 둘러싸여 있는 종양으로 Antoni A형과 Antoni B형으로 나누어진다. Antoni A형은 방추형세포가 밀집되 어 배열되어 있고 주로 척수나 말초신경 종양에 많고 An- toni B형은 성상세포들이 밀집되어 그물같이 형성되어 있 는 것이 특징이다5)10).
결 론
하지마비로 내원한 37세 남자환자에서 흉추부 결핵성 척 수염과 척수 신경초종이 모두 척수를 압박하여 증상을 유발 시키는 매우 드문 경우를 2차례의 수술로 만족할 만한 신경 학적 호전을 보였기에 문헌 고찰과 함께 보고하는 바이다.
•논문접수일:2001년 5월 4일
•심사완료일:2004년 7월 20일
•책임저자:박 종 훈
630-522 경남 마산시 회원구 합성2동 50번지 성균관대학교 의과대학 마산삼성병원 신경외과학교실 전화:055) 290-6899, 전송:055) 290-6899 E-mail:[email protected]
References
1) Alvarez S, McCabe WR:Extrapulmonary tuberculosis revi- sited:A review of experience at Boston City and other hos- pitals. Medicine 6:25-55, 1984
2) Cantwell MF, Snider DE, Cauthen GM, Onorato IM:Epide- miology of tuberculosis in the United States, 1985 through 1992,
JAMA 272:535-539, 1994
3) Crenshaw AH:Campbell’s Operative Orethopedics. 8th ed., Saint Louis:The CB Mosby company, 1992, pp3802-3823 4) Dobson J:Tuberculosis of the spine:An analysis of the results
of conservative treatment and of the factors influencing the prognosis. J Bone Joint Surg(Br) 33:517-531, 1951 5) Enzinger FM, Weiss SW:Benign tumors of peripheral ne-
rves:Soft tissue tumors. The CV Mosby Co, 1983, pp586-615 6) Hsu LC, Leong JC:Tuberculosis of the lower cerviceal spine
(C2 to C7). J Bone Joint Surg 66:1-5, 1984
7) Kim YT, Chung HY:Wide-spread benign schwannoma invol- ving multiple cervical vertebral bodies. J Korean Neurosurgical Society 9:615-617, 1980
8) Lifeso RM, Weaver P, Harloke H:Tuberculous spondylitis in adults. J Bone Joint Surg(Am) 67:1045-1413, 1985 9) Mason TH, Keiger HA:Intramedullary spinal neurilemmoma.
J Neurosurgery 29:414-416, 1968
10) Northfield DWC:Schwannoma and neurofibroma:The sur- gery of the central nervous system. Blackwell scientific publi- cations, 1973, pp263-279
11) Park KS, Sim BS:A case of intramedullary neurilemmoma.
J Korean Neurosurgical Society 3:55-58, 1974
12) Rebecca W, Zafar Q, David S, Wurtz R, Quader Z, Simon D, et al:Cervical tuberculous vertebral osteomyelitis:Case re- port and discussion of the literature. Clin Infect Dis 16:806- 808, 1993
13) Rothman RH and Simeone FA:The Spine. 3rd ed. W.B. Sa- unders Company, 1992
14) Slater RR, Beale RW, Bullitt E:Pott’s disease of the cervical spine. South Med J 84:521-523, 1991
15) Stagnara P, DE Mauroy JC, Dran G, Gonon GP, Costanzo G, Dimnet J, et al:Reciprocal angulation of vertebral bodies in a sagittal plane:Approach to references for the lordosis. Spine 7:335-342, 1982
16) Tuli SM:Results of the treatment of spinal tuberculosis by “mi- ddle-path” regimen. J Bone Joint Surg(Br) 57:13-23, 1975 17) Vinken PH, Bruyn GW:Tumors of the spine and spinal cord:
Hand book of clinical neurology. Amer Elsevier Pub Co Inc, New York part 2, 19, 1976, pp18-20
18) Vinken PH, Bruyn GW:Tumors of the spine and spinal cord: Hand book of clinical neurology. Amer Elsevier Pub Co Inc, New York part 2, 20, 1976, pp238-289
19) Weinstein JN and Wiesel SW:The Lumbar Spine. W.B. sa- unders Company, 1990
20) Youman JR:Spinal cord tumors in adult:Neurological sur- gery. WB Saunders Co Philadelphia London Toronto Vol 5, 1982, pp3202-3204