대한소화기학회지 2002;40:23-31
서 론
5)접수: 2002년 1월 23일, 승인: 2002년 5월 31일
연락처: 양웅석, 602-739, 부산광역시 서구 아미동 1가 10번지 부산대학교 의과대학 내과학교실
Tel: (051) 240-7516, Fax: (051) 244-8180 E-mail: [email protected]
Helicobacter pylori (이하 H. pylori)는 1983년 Warren1과 Marshall2에6)의해 위전정부 점막 조직생검에서 분리 동정
Correspondence to: Ung Suk Yang, M.D.
Department of Internal Medicine, Pusan National University College of Medicine
1-10 Ami-dong, Seo-gu, Busan 602-739, Korea Tel: +82-51-240-7516, Fax: +82-51-244-8180 E-mail: [email protected]
양성 위십이지장질환과 Helicobacter pylori cagA, vacA, iceA Genotype의 연관성에 관한 연구
부산대학교 의과대학 내과학교실
박승근·김광하·정을조·배용목·허 정·주형준·강대환·송근암·조 몽·양웅석
Clinical Relevance between the cagA, vacA, and iceA Status of Helicobacter pylori and Benign Gastroduodenal Diseases
Seung Keun Park, M.D., Gwang Ha Kim, M.D., Eul Jo Jeong, M.D., Yong Mock Bae, M.D., Jeong Heo, M.D., Hung Jun Chu, M.D., Dae Hwan Kang, M.D. Geun Am Song, M.D.,
Mong Cho, M.D., and Ung Suk Yang, M.D.
Department of Internal Medicine, Pusan National University College of Medicine, Busan, Korea
Background/Aims: There have been some reports regarding the cagA genotype of Helicobacter pylori (H. pylori), but only a few reports regarding the vacA and iceA genotypes of H. pylori in Korea. The aim of this study was to assess the relationships between genotypes of H. pylori and the severity of benign gastroduodenal diseases such as peptic ulcer disease (PUD) and nonulcer dyspepsia (NUD). Methods: Seventy H. pylori-positive patients with PUD or NUD were selected. Then, the genotypes of H. pylori obtained from them were analyzed using polymerized chain reaction. Results: cagA was detected in 91.3% (64/70) of the patients. The occurrence was similar in the patients with PUD and NUD (96.4% vs. 88.1%, p=0.390). Among vacA genotypes, s1 type was predominantly observed in 84.3% (59/70) of the patients. The occurrences of their subtypes were as follows: s1a/m1, 18.6%;
s1a/m2, 10.0%; s1c/m1, 51.5%; s1c/m2, 4.3%. The s1b type was not detected. The s2 type was detected in only 2.8%
of the patients. There was no difference in the frequency of vacA s1 between PUD and NUD (78.6% vs. 88.1%, p=0.283). iceA1 and iceA2 were detected in 91.4% (64/70) and 4.3% (3/70) of the patients, respectively. There was no difference in the frequency of iceA1 between PUD and NUD (89.3% vs. 92.9%, p=0.601). vacA s1/cagA
+/iceA1 strains were the most frequently found genotype, but there was no difference in the frequency between PUD and NUD (86.9% vs. 88.6%, p=1.000). Conclusions: cagA, vacA, and iceA genotypes of H. pylori strains are not associated with the severity of benign gastroduodenal diseases. (Korean J Gastroenterol 2002;40:23-31)
Key Words: Helicobacter pylori; cagA; vacA; iceA
대한소화기학회지: 제40권 제1호, 2002
된 나선형 간균으로 만성 위염, 십이지장궤양,3 위궤양 및 위선암4 그리고 위임파종5,6의 발병에 중요한 역할을 한다.
세계 인구의 50% 이상이 H. pylori에 감염되어 일생 동 안 지속되지만 이들 중 소수만이 임상적으로 의미 있는 질 환 즉, 소화성 궤양이나 위선암 등을 야기시킨다. 이러한 발병 요인으로 H. pylori 개개의 특성,7-9숙주의 면역반응,10 감염시기, 혹은 환경 요인11 등 많은 인자가 관여할 것으로 생각된다. H. pylori 개개의 특성으로 H. pylori 균주는 많은 이질성을 보이고, 표현형 변이12가 다양하며 여러 종류의 병독인자(virulence factor)를 가지고 있는 것으로 알려져 있 다.13 특히 병독인자는 H. pylori 균주 중 독성을 나타내는 균에 감염된 경우에 한하여 질병이 발생한다는 가정하에 연구되어 현재까지 발병에 관련된 특이적인 병독인자를 찾는 연구가 많이 진행되었다.
질병 연관 병독인자로는 67kD 크기의 vacA (vacuolating cytotoxin A) 유전자와 128kD 크기의 cagA (cytotoxin associated gene product A) 유전자 2가지가 가장 주목을 받고 있다.14-16 vacA는 H. pylori 균에서 분리되어 위상피세포에 공포 (vacuolation)를 일으키는 단백질을 생성하는 유전자로 모 든 균주에 존재하며, 유전학적으로 모자이크형(mosaicism) 이 존재한다.17,18 암호순서부위(signal sequence)와 중간지 역(mid region)을 발현하는 대립유전자(allele)의 다형성 (polymorphism)을 보이는데, 암호순서부위는 다시 s1a, s1b, s1c 그리고 s2의 4가지 유형을, 중간지역은 m1 및 m2의 2가지 유형을 보인다.
이러한 vacA 대립유전자의 모자이크 조합이 독소의 생 성을 결정하며, 균주의 발병 원인과 관련이 있다. vacA s1/m1 균주는 s1/m2 균주보다 다량의 독소를 생성하나 s2/m2 균주는 매우 적은 양의 독소를 생성하거나 하지 않 는다. 즉, s1a 유전자형이 s1b나 s2 유전자형에 비해서 더 심한 염증을 일으키며, m1 유전자형이 m2 유전자형보다 위상피세포에 더 많은 손상을 일으켜 소화성 궤양 환자에 서 더 빈도가 높음이 보고되었다.19
cagA는 균주에 따라 크기가 다양하고 CagA 단백질을 생 성하며, 약 40개의 유전자로 구성된 cag pathogenecity island 에 속해 있다.20이 복합체 중 몇 개의 기능적인 유전자들이 균주의 독성을 증가시키고 위상피세포에서 IL-8 생성을 촉 진한다.21,22
최근 iceA(induced by contact with epithelium)가 새로운 병독인자로 발견되었는데, 위상피세포와의 접촉에 의해 유 도되는 유전자이다.23iceA는 iceA1과 iceA2 두 유형의 주요 대립유전자가 있으며, iceA1의 주된 기능은 아직 명확하지 않으나 세균의 제한효소로 추정되며, H. pylori와 위상피세 포와의 접촉에 의해서 표현이 증강되고 소화성 궤양과 관 련이 있는 것으로 주장되고 있다.24,25
전세계적으로 H. pylori에 감염된 환자 모두를 치료하 기란 불가능하며 또한 비경제적이다. 따라서 독성과 관 련된 유전자형(genotype)과 연관성이 있는 균주에 감염된 환자만을 선택하여 예방적인 H. pylori 치료를 하고자 하 는 연구 보고들이 서구에서는 있다.22,24,25 그러나 국내에 서는 cagA와 위질환의 관련성에 대한 많은 연구가 이루 어졌지만 vacA, iceA 유전자형에 대한 보고는 드물다. 이에 저자들은 우리 나라에서 양성 위십이지장질환과 H. pylori cagA, vacA, iceA 유전자형의 연관성을 연구하고자 하였 다.
대상 및 방법
1. 대상
2001년 1월부터 9월까지 상부위장관증상으로 부산대 학교부속병원 내과에 내원한 환자 중 내시경검사를 시 행하여 rapid urease 검사, 조직검사, 중합체효소 연쇄반응 (polymerase chain reaction, 이하 PCR)으로 H. pylori 양성 이 확인된 70명 (남:여 42:28, 평균 연령 56.9세)의 양성 위 십이지장질환(위궤양 14명, 십이지장궤양 14명, 비궤양성 소화불량증 42명)을 대상으로 하였다.
2. 방법
1) 위생검 조직에서 DNA 분리
위생검 조직은 채취 즉시 -70oC 액체질소탱크에서 실험 직전까지 보관되었다. 해동된 조직에 TEN 완충액 [0.1 M NaCl, 10 mM tris·Cl (pH 8.0), 1 mM EDTA (pH 8.0)]
300 µL, 10% SDS 25 µL 및 proteinase-K (10 mg/mL) 20 µL 를 주입한 후 37oC에 14시간 두었다. 여기에 400 µL의 phenol/chloroform/isoamyl alcohol (25:24:1)을 가한 다음 진 탕하여 5분간 12,000 rpm에서 원심분리하고 상층액을 취하 여 chloroform/isoamyl alcohol (24:1) 400 µL로 이 과정을 한번 더 반복하였다. 각 검체에 5 M NaCl 10 5 µL, 냉동실 에 넣어둔 100% 에탄올 1,000 µL를 주입하여 -20oC에서 1시간 방치시킨 다음 12,000 rpm에서 20분간 원심분리를 하 였다. DNA 압착결정(pellet)을 취하여 70% 에탄올 1,000 µL 를 주입하고 12,000 rpm에서 5분간 원심분리한 다음, 상층 을 제거 후 DNA 압착결정을 건조시켰다. 그 후 20 µL의 TEN 완충액에 녹여 PCR에 사용하였다.
2) PCR primers 선정 및 제작
H. pylori 검출을 위한 실험에 사용한 PCR 시발체는 BIO-SYNTHESIS사에 주문 합성하였으며 ureA의 744번에서 853번까지의 109 bp를 증폭시켰다. cagA 검출을 위한 실험 24
박승근 외 9인. 양성 위십이지장질환과 H. pylori genotype
에 사용한 PCR 시발체는 cagA의 중간유지지역의 349 bp 절 편을 갖고 있는 CAGAF와 CAGAR 시발체를 사용하였다.
vacA s 유전자의 4가지 유형 즉 s1a, s1b, s1c 그리고 s2 대립유전자의 분석을 위해 Atherton 등17,18이 사용했던 VA1-F, VA1-R, S1A-F, SS3-F, S1C-F 시발체 등을 사용하 였고, vacA m 유전자의 m1, m2 두 유형의 대립유전자 분 석을 위해 VAG-F와 VAG-R 시발체를 각각 사용하였다.
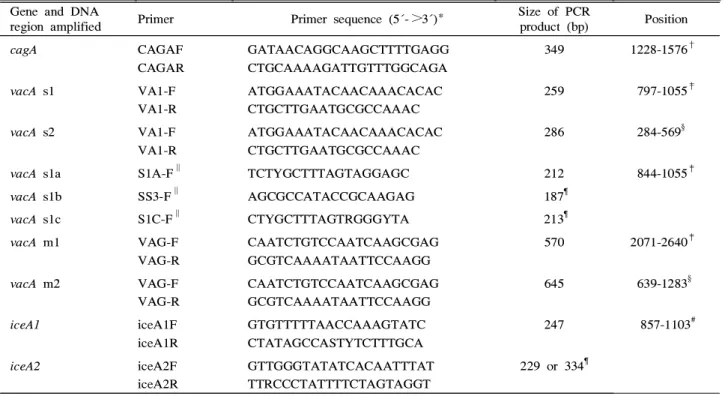
iceA 유전자의 iceA1 및 iceA2 두 유형의 대립유전자 분 석을 위해서는 Doorn 등25,26이 사용한 iceA1F, iceA1R, iceA2F 그리고 iceA2R 시발체들을 사용하였다. 이 연구에 사용된 PCR 시발체들은 Table 1과 같다.
3) PCR 조건 및 산물의 검출
PCR 반응은 10 mM Tris-HCl (pH 8.3), 50 ml KCl, 1.5 mM MgCl2, 0.001% gelatin, 5 pmole의 각 시발체와 200 µM의 dATP, dGTP, dCTP, dTTP 및 0.5 unit의 Tag DNA 중합효소로 구성된 용액에 검체 DNA 5 µL와 증류수 를 가하여 25 µL가 되게 하였다.
PCR 반응은 programmable thermal cycler (Perkin-Elmer
Table 1. PCR Primers for Amplication of cagA, vacA, and iceA Sequences Gene and DNA
region amplified Primer Primer sequence (5´->3´)* Size of PCR
product (bp) Position
cagA CAGAF
CAGAR
GATAACAGGCAAGCTTTTGAGG CTGCAAAAGATTGTTTGGCAGA
349 1228-1576†
vacA s1 VA1-F
VA1-R
ATGGAAATACAACAAACACAC CTGCTTGAATGCGCCAAAC
259 797-1055‡
vacA s2 VA1-F
VA1-R
ATGGAAATACAACAAACACAC CTGCTTGAATGCGCCAAAC
286 284-569§
vacA s1a S1A-F∥ TCTYGCTTTAGTAGGAGC 212 844-1055‡
vacA s1b SS3-F∥ AGCGCCATACCGCAAGAG 187¶
vacA s1c S1C-F∥ CTYGCTTTAGTRGGGYTA 213¶
vacA m1 VAG-F
VAG-R
CAATCTGTCCAATCAAGCGAG GCGTCAAAATAATTCCAAGG
570 2071-2640‡
vacA m2 VAG-F
VAG-R
CAATCTGTCCAATCAAGCGAG GCGTCAAAATAATTCCAAGG
645 639-1283§
iceA1 iceA1F
iceA1R
GTGTTTTTAACCAAAGTATC CTATAGCCASTYTCTTTGCA
247 857-1103#
iceA2 iceA2F
iceA2R
GTTGGGTATATCACAATTTAT TTRCCCTATTTTCTAGTAGGT
229 or 334¶
* Y is C or T, S is C or G, and R is A or G.
†Nucleotide positions in the cagA gene of H. pylori ATCC 53726 (Genbank accession no. L117714).
‡Nucleotide positions in the vacA gene of H. pylori 60190 (Genbank accession no. U05676).
§Nucleotide positions in the cagA gene of H. pylori Tx30a (Genbank accession no. U29401).
∥Used with primer-R.
¶No published coordinates for genes in strains of these types.
#Nucleotide positions in the iceA gene of H. pylori 60190 (Genbank accession no. U43917).
2400, Norwalk, USA)를 사용하였고, 그 방법은 먼저 94℃
에서 5분간 초기 변성을 충분히 시킨 후 94℃ 1분, 52℃
1분, 72℃ 1분씩의 반응 과정을 35회 반복하였고 마지막 단 계에서 72℃ 10분간 충분한 extension 과정을 추가하였다.
Mupid-2 전기영동 장치에서 ethidium bromide가 함유된 2% agarose gel에서 TAE buffer (40 mM Tris-acetate, 1 mM EDTA, pH 8.0)를 이용하여 100 V 일정 전압으로 20분간 전 기영동하였다. 100 bp ladder (Promega)를 size marker로 사용 하여 특이적인 band가 나타나는지 본 후 UV transilluminater 위에서 polaroid camera로 사진을 찍었다(Fig. 1, 2).
3. 통계 분석
데이터는 SPSS 버전 10.0.1에 의해 분석되었다. Pearson X2 검정과 Fisher의 직접확률계산법은 개개의 유전자형과 소화성 궤양 질환 사이의 상관관계를 평가하기 위해 사용 하였고, 소화성 궤양과 H. pylori의 vacA, cagA 그리고 iceA 유전자들의 서로 다른 조합과의 관련을 평가하기 위해서는 McNemar 검정을 사용하였다. p value는 0.05 미만일 때 통 계학적으로 의미 있는 것으로 받아들이기로 하였다.
25
The Korean Journal of Gastroenterology: Vol. 40, No. 1, 2002
Fig. 1. PCR products of vacA s subtype resolved by electro- phoresis in 2% agarose gel. Lane 1, 100 bp DNA ladder; lane 2, vacA s1 (259 bp) band; lane 3, vacA s2 (286 bp) band; lane 4, vacA s1a (212 bp) band; lane 5, vacA s1b (187 bp) band; lane 6, vacA s1c (213 bp) band.
Fig. 2. PCR products of vacA m subtype and iceA alleles resolved by electrophoresis in 2% agarose gel. Lane 1 and 5, 100 bp DNA ladder; lane 2, vacA m1 (570 bp) band; lane 3, vacA m2 (645 bp) band; lane 4, vacA m1/m2 (570/645 bp) band; lane 6, iceA1 (247 bp) band; lane 7, iceA2 (229 bp) band.
결 과
1. 소화성 궤양 및 비궤양성 소화불량증 환자의 비교 70명의 환자 중 소화성 궤양 환자는 40%, 비궤양성 소 화불량증 환자는 60%였으며, 양군 사이의 평균 연령 (각 각 50.3±13.7세, 48.6±12.1세)에 의미있는 차이는 없었다 (p=0.603).
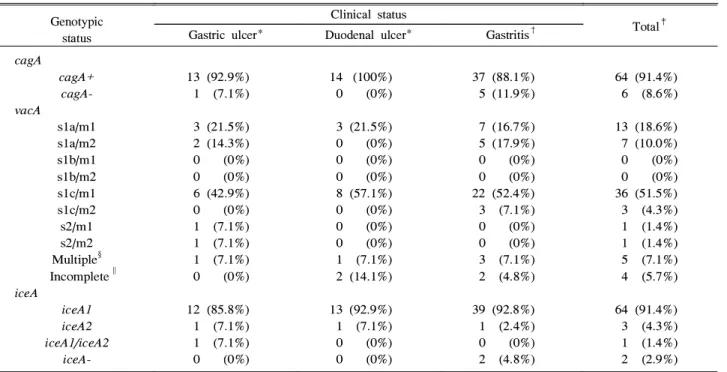
Table 2. Frequency of cagA, vacA, and iceA Status of H. pylori Strains in Gastric Biopsy Specimens from 70 Patients
Genotypic status
Clinical status
Total‡ Gastric ulcer* Duodenal ulcer* Gastritis†
cagA
cagA+
cagA- vacA
s1a/m1 s1a/m2 s1b/m1 s1b/m2 s1c/m1 s1c/m2 s2/m1 s2/m2 Multiple§ Incomplete∥ iceA
iceA1 iceA2 iceA1/iceA2
iceA-
13 (92.9%) 1 (7.1%)
3 (21.5%) 2 (14.3%) 0 (0%) 0 (0%) 6 (42.9%) 0 (0%) 1 (7.1%) 1 (7.1%) 1 (7.1%) 0 (0%)
12 (85.8%) 1 (7.1%) 1 (7.1%) 0 (0%)
14 (100%) 0 (0%)
3 (21.5%) 0 (0%) 0 (0%) 0 (0%) 8 (57.1%) 0 (0%) 0 (0%) 0 (0%) 1 (7.1%) 2 (14.1%)
13 (92.9%) 1 (7.1%) 0 (0%) 0 (0%)
37 (88.1%) 5 (11.9%)
7 (16.7%) 5 (17.9%) 0 (0%) 0 (0%) 22 (52.4%) 3 (7.1%) 0 (0%) 0 (0%) 3 (7.1%) 2 (4.8%)
39 (92.8%) 1 (2.4%) 0 (0%) 2 (4.8%)
64 (91.4%) 6 (8.6%)
13 (18.6%) 7 (10.0%) 0 (0%) 0 (0%) 36 (51.5%) 3 (4.3%) 1 (1.4%) 1 (1.4%) 5 (7.1%) 4 (5.7%)
64 (91.4%) 3 (4.3%) 1 (1.4%) 2 (2.9%)
* Peptic ulcer observed during gastroscopy or a documented history of ulcer disease. Percentages are given as a fraction of the total number of patients with gastric (n=14) or duodenal (n=14) ulcers.
†No peptic ulcer observed and no documented history of ulcer disease. Percentages in this column are given as a fraction of the total number of non-ulcer patients (n=42).
‡Percentages in this column are given as a fraction of the total number of patients (n=70).
§More than 1 vacA genotype detected, see also Table 4.
∥No signal sequence of vacA detected.
2. cagA 유전자 검출
위전정부에서 채취된 생검 조직으로부터 분리한 DNA를 cagA, vacA 그리고 iceA 유전자 분석을 위해 사용하였으며, 그 유전자 분석의 결과는 Table 2와 같다. 검체의 91.4%
(64/70)에서 cagA 유전자 양성이었고, cagA 양성 균주는 위 궤양과 십이지장궤양에서 차이가 없었다(92.9% vs. 100%, p=1.000). 소화성 궤양과 비궤양성 소화불량증에서도 차이 26
7
Park, et al. cagA, vacA, and iceA Status of H. pylori in Benig Gastroduodenal Diseases
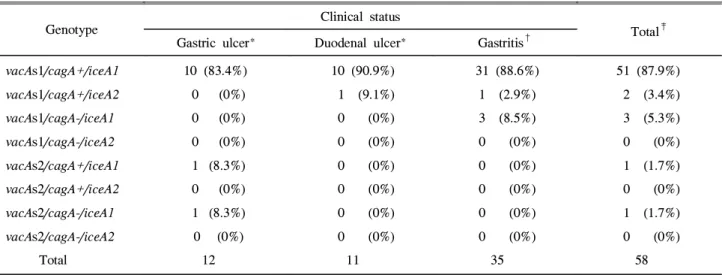
Table 3. vacA, cagA, and iceA Genotype Distribution among Ulcer and Non-ulcer Patients with a Single Combined Genotype
Genotype Clinical status
Total‡ Gastric ulcer* Duodenal ulcer* Gastritis†
vacAs1/cagA+/iceA1 vacAs1/cagA+/iceA2 vacAs1/cagA-/iceA1 vacAs1/cagA-/iceA2 vacAs2/cagA+/iceA1 vacAs2/cagA+/iceA2 vacAs2/cagA-/iceA1 vacAs2/cagA-/iceA2
Total
10 (83.4%) 0 (0%) 0 (0%) 0 (0%) 1 (8.3%) 0 (0%) 1 (8.3%) 0 (0%)
12
10 (90.9%) 1 (9.1%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
11
31 (88.6%) 1 (2.9%) 3 (8.5%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
35
51 (87.9%) 2 (3.4%) 3 (5.3%) 0 (0%) 1 (1.7%) 0 (0%) 1 (1.7%) 0 (0%)
58
* Peptic ulcer observed during gastroscopy or a documented history of ulcer disease. Percentages are given as a fraction of the total number of patients with gastric (n=12) or duodenal (n=10) ulcers.
†No peptic ulcer observed and no documented history of ulcer diease. Percentages in this column are given as a fraction of the total number of non-ulcer patients (n=35).
‡Percentages in this column are given as a fraction of the total number of patients with a single genotype (n=58). Patients with multiple vacA (n=5) and /or iceA (n=1) genotypes, as well as incomplete vacA (n=4) and/or untypeable iceA (n=2) genotypes, were excluded from analysis.
를 발견할 수 없었다(96.4% vs. 88.1%, p=0.390).
3. vacA 유전자 검출
완전한 vacA s- 및 vacA m- 대립유전자는 70명 중 66명 (5명은 복합형)으로 나타났고 불완전형이 4명이었다. s1 대 립유전자가 대부분(59/70, 84.3%)으로 s1c형 (39/59, 66.1%), s1a형(21/59, 35.6%)에서 양성이었으나 s1b형은 모든 환자에 서 음성이었고 독소를 생성하지 않는다고 알려진 vacA s2/m2형은 1명(7.1%)이었다. vacA s1 양성 균주는 위궤양과 십이지장궤양에서 차이가 없었다(78.6% vs. 78.6%, p=1.000).
소화성 궤양과 비궤양성 소화불량증에서도 차이를 발견할 수 없었다(78.6% vs. 88.1%, p=0.283). 질병의 임상양상과 관 계없이 vacA s1c/m1형이 가장 높은 비율(위궤양 42.9%, 십이 지장궤양 57.1% 그리고 비궤양성 소화불량증 52.4%)로 나 타났다.
4. iceA 유전자 검출
iceA1은 91.4% (64/70), iceA2는 4.3% (3/70)로 나타났다.
1명의 위궤양 환자에서 iceA1과 iceA2 모두 양성이었으며, vacA s1c/m1을 동반하였다. 비궤양성 소화불량증 환자 2명 에서 iceA에 대한 PCR이 음성으로 나타났다. iceA1 유전자는 위궤양과 십이지장궤양 사이에는 차이가 없었다(85.8% vs.
92.9%, p=0.541). 또한 소화성 궤양과 비궤양성 소화불량증 에서도 차이를 발견할 수 없었다(89.3% vs. 92.9%, p=0.601).
5. vacA, cagA 그리고 iceA 유전자형 조합
vacA s-유전자형(s1과 s2), cagA (양성 및 음성), 그리고 iceA 대립유전자형(iceA1과 iceA2)의 조합에 의한 분석으로 8개의 서로 다른 유전자 조합이 밝혀졌다(Table 3). vacA s1/cagA+/iceA1 유전자형이 87.9% (51/58)으로 가장 높았으 며, 소화성궤양과 비궤양성 소화불량증에서 의미 있는 차이 는 없었다(86.9% vs 88.6%, p=1.000). vacA s1/cagA-/iceA2, vacA s2/cagA+/iceA2 그리고 vacA s2/cagA-/iceA2 유전자형 은 양군 모두에서 음성이었다.
vacA 및 cagA만 고려한다면, vacA s1/cagA+은 소화성 궤양과 비궤양성 소화불량증에서 차이가 없었다(91.3%
vs. 91.4%, p=0.987). 그러나 비궤양성 소화불량증 환자 3명(8.5%)에서 vacA s1/cagA-가 양성으로, 한 명도 나타나 지 않은 소화성 궤양과 차이를 보였다. vacA 및 iceA만 고려한다면, vacA s1/iceA1은 소화성 궤양과 비궤양성 소 화불량증에서 의미있는 차이는 없었다(86.9% vs 97.1%, p=0.290).
6. cagA, vacA 그리고 iceA의 연관성
single vacA 유전자 중 cagA 양성은 93.1% (54/58)였고 이중 96.3% (52/54)에서 vacA s1을 가진 것으로 나타났으나 cagA와 vacA s1 사이에는 연관성이 없었다(p=0.219). iceA 유전자 중 cagA 양성은 93.1% (54/58)였고, 이중 96.3%
27
대한소화기학회지: 제40권 제1호, 2002
(52/54)에서 iceA1을 가진 것으로 나타났으나 cagA와 iceA1 사이에는 연관성이 없었다(p=0.727).
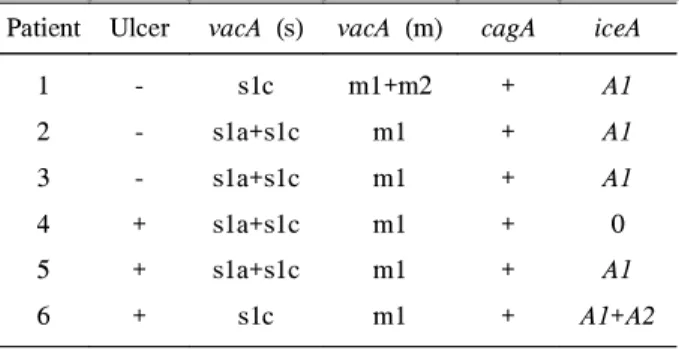
7. vacA 혹은 iceA의 다발 유전자형
8.6% (6/70)에서 나타났으며 질병 양상과의 관련성은 없 었다(Table 4).
Table 4. vacA, cagA, and iceA Genotypes in Biopsy Specimens Containing Multiple Strains
Patient Ulcer vacA (s) vacA (m) cagA iceA 1
2 3 4 5 6
- - - + + +
s1c s1a+s1c s1a+s1c s1a+s1c s1a+s1c
s1c
m1+m2 m1 m1 m1 m1 m1
+ + + + + +
A1 A1 A1 0 A1 A1+A2
고 찰
H. pylori 감염은 전 세계 인구의 50% 이상이 감염되어 있으며, 만성 위염, 위궤양3 및 십이지장궤양, 위암4 그리고 위림프종5,6 등의 중요한 인자로 알려져 있다.
서구의 경우 분리된 H. pylori의 60∼70%가 cagA 유전자 양성이며, 소화성 궤양 환자에서 높은 빈도로 cagA 유전자 양성으로 나타나고 이에 대한 CagA 단백을 발현하므로 상 부위장관질환과의 연관성을 주장하는 보고가 많다.14-16,27 이에 반해 성인의 80% 이상이 감염되어 있는 국내에서의 보고는 상당히 차이가 있다. cagA의 발현율은 서구의 발현 율보다 높아서 약 60∼90%에서 발현되는 것으로 보고되고 있지만, 대부분의 십이지장궤양과 소화불량증 환자 사이에 유의한 차이가 없는 것으로 보고하고 있다.28-38
본 연구는 소화성 궤양 환자 및 비궤양성 소화불량증 환 자에서 유문륜에서 2 cm 근처 전정부에서 생검을 하여 생 검조직내 H. pylori DNA를 이용하여 ureA PCR법을 실시하 였고 이후 cagA PCR법을 실시하였다.39,40 ureA 양성 소화 성 궤양 환자 및 비궤양성 소화불량증 환자에서 primary PCR에 의한 cagA 검사 결과 양성률이 각각 96.4%, 88.1%
로 양자 간의 양성률에 차이가 없었다. 이는 국외보다는 높 고 국내 보고와는 유사한 양성률을 보였다..25,30-35 본 연구 에서의 높은 양성률은 rapid urease검사상 양성으로 나온 환 자들을 대상으로 선정했기 때문으로 생각된다.
서구의 연구에서 vacA는 모든 박테리아에 존재하나 분리 균주의 약 50∼60%에서 VacA 독소를 생산한다고 알려져
왔다. 특히 소화성 궤양 환자에서 분리한 세균에서는 60%
이상이 세포독소를 생산하는 데 반해 위염에서는 30% 정 도에서 세포독소를 생산하여 이것이 발병인자로 작용한다 고 주장한다.16-19,25,41
이에 반해 국내에서는 미약하나마 VacA에 대한 혈청 양성률과 상부위장관질환의 연관성에 관한 연구 보고가 있는데 VacA의 혈청 양성률은 대개 50%
정도 양성이며 소화성 궤양과 만성 위염 사이에는 차이가 없다는 보고가 있다.28,36
본 연구에서는 vacA 유전자형과 상부위장관질환 사이의 관련성에 관한 것으로 vacA는 분리 균주 100%에서 발견되 었으며, vacA 유전자아형에 따른 차이는 s1형이 대부분 (84.3%)으로 s1c형(66.1%), s1a형(35.6%)에서 양성이었으나 s1b형은 모든 환자에서 음성이었다. 이는 다른 연구42에서 보고한 서울 지역에서의 s1c형(90%), s1a형(7%)와 비교하 면 다소 차이가 있는데, 이 점은 국내에서도 지역적 차이가 있음을 시사한다.
본 연구에서는 vacA 유전자형 중 s1c형이 질병 양상과는 관계없이 우세하였고 s1b형은 모두 음성이었는데, 최근 브 라질에서의 연구는 브라질, 코스타리카, 페루 및 콜롬비아 등의 중미 및 남미에서는 vacA s1b형이 우세하였음을 보고 하였다.42 또 다른 연구에서 세계의 여러 지역에서 서로 다 른 균주의 존재가 증명되고 있으며, 24개국에서 700개 이 상의 H. pylori 균주를 분석하여 vacA 유전자형이 s1a형은 북유럽 및 오스트레일리아에서, s1b형은 남미에서, 그리고 s1c형은 동아시아에서 주요 형이나 서유럽에선 극히 드문 형임을 발견하여 전세계적으로 분포가 다름을 보고하였 다.43,44
일부 보고17,19에서는 cagA의 존재와 소화성 궤양과의 의 미 있는 관련성 및 vacA s1형이 s2형 균주보다 더 흔히 소 화성 궤양에서 발견되어 cagA 및 vacA s1 genotype의 존재 가 소화성 궤양과 매우 연관성이 있다고 주장하였다. 그러 나 본 연구에서는 vacA s1형이 s2형 균주보다 질병에 관계 없이 훨씬 우세하였으나 각 임상질환군 사이에 유의한 차 이는 없어 아시아의 보고42,45,46및 기존의 국내의 연구 보고
28-38
를 확인할 수 있었다.
또 다른 보고25에서는 최근에 발견된 iceA 유전자의 다양 성 및 임상양상과의 관련성에 대해 네덜란드의 환자들에서 채취한 94개의 위생검 조직을 분석하여 iceA1 대립유전자 가 소화성 궤양 질환에서 훨씬 우세하게 나타나 cagA 및 vacA와는 독립적으로 소화성 궤양 질환의 예측인자가 될 수 있다고 하였다. 본 연구의 데이터는 iceA1형이 질병에 관계없이 훨씬 우세하였으나 각 임상질환군 사이에 유의한 차이가 없어, 일본에서의 연구 결과47와 일치한다. 이 점에 서 서구와 달리 아시아에서는 iceA 대립유전자와 질병의 임상 양상과는 관련성이 없으리라 생각된다. 한편, 본 연구 28
박승근 외 9인. 양성 위십이지장질환과 H. pylori genotype
에서 iceA1 대립유전자가 질병에 관련없이 우세하였는데, 이는 네덜란드25 및 일본42,47과는 유사한 결과였지만 미국 및 콜롬비아42에서는 iceA2 대립유전자가 우세하게 나타나 지역적 차이가 있음을 알 수 있다.
이런 일련의 보고들에서 알 수 있듯이 지역에 따른 vacA 및 iceA 유전자형들의 양상들은 다르게 나타났는데, 이는 H. pylori 감염의 예측 병독인자로서의 지역적 차이 혹은 인종에서도 차이를 보임을 시사한다. 즉, 한 지역에서 혹은 한 인종에서 H. pylori와 관련된 우세한 유전자형은 다른 지 역이나 인종에서 동일한 결과가 나오지 못하므로 H. pylori 의 예측인자로서 될 수 없음을 시사한다.
연구에서는 질병 양상과 관계없이 cagA+ vacA s1c/m1 iceA1 유전자형이 가장 우세하였는데, 이는 서울 지역과 일 본에서도 유사한 결과를 보였다.42 이런 점으로 보아 동아 시아에서는 질병 양상과 관계없이 전자의 유전자형이 우세 할 것으로 예측할 수 있다.
본 연구에서는 소화성 궤양을 가진 환자 모두가 H. pylori 의 병독인자의 유전자형을 갖지는 않듯이 역으로 병독인자 의 유전자형들이 소화성 궤양을 갖고 있지 않은 환자들에 서도 나타났다. 내시경을 시행할 시점에서 몇 가지 중요한 점이 고려되어야 하는데,25첫째, 임상적 진단의 확실성으로 내시경상 위염만 있던 환자들이 나중에 궤양으로 진행될 수도 있고 과거 궤양을 앓았던 사람이 현재는 위염만 있는 상태로 증상을 호소하는 경우가 있다. 따라서 현재에는 위 염으로만 잘못 분류되는 경우가 있다. 둘째, 위생검 조직 의 부위에 따른 차이점으로 위전정부, 위체부, 위기저부 등의 부위에 따른 H. pylori의 존재 및 밀도에 있어서 차 이가 있기 때문에 표본 추출 오류의 영향을 배제하여야 한다. 셋째, 담배, 위산분비 등 그리고 HLA 상태 등의 숙 주인자도 H. pylori 감염의 임상 발현에 영향을 미칠 수 있고 병독인자와 상호작용할 수 있다는 점으로 비교연구 가 필요하다. 넷째, 부가되는 병독인자들의 역할도 무시할 수 있는가 하는 점이다. 특히 babA와 관계 있는 혈액형군 항원이나 Lewis 항원 등이 소화성 궤양 환자에서 발현율이 높다고 보고되고 있다.48,49
본 연구에서는 서구에서의 연구와는 다르게 cagA 및 vacA s1 유전자형의 존재가 소화성 궤양과 강한 연관성이 있음을 입증하지 못했고, 마찬가지로 iceA1이 소화성 궤양 질환에서 cagA 및 vacA와는 독립적으로 소화성 궤양 질환 의 병독인자가 될 수 있음을 확인할 수 없었다. 이러한 연 구 결과의 차이는 지역적 차이에 기인한 것으로 추정되나 더욱 광범위한 연구가 필요할 것으로 생각된다.
결론적으로 양성 위십이지장질환에서 cagA+vacA s1c/m1 iceA1 유전자형이 국내에서 가장 많은 빈도로 발견되었으 나, cagA, vacA(s1a, s1b, s1c, s2, m1, m2), iceA(A1, A2) 양
상은 소화성 궤양군과 비궤양성 소화불량증 환자군에서 차 이를 보이지 않아 본 연구에서는 H. pylori 유전자형과 양 성 위십이지장질환의 중증도와는 연관성이 없는 것으로 나 타났다.
요 약
목적: H. pylori 감염의 임상양상이 독성과 관련된 유전 자형과 연관성이 있는 균주에 감염된 환자만을 선택하여 예방적인 H. pylori 치료를 하고자 하는 연구 보고가 서구 에서는 많다. 그러나 국내에서는 cagA와 위질환의 관련성 에 대한 많은 연구가 이루어졌지만 vacA, iceA 유전자형 에 대한 보고는 드물다. 이에 저자들은 국내에서의 양성 위십이지장질환에서 H. pylori cagA, vacA, iceA 유전자형 과의 연관성을 연구하였다. 대상 및 방법: 상부위장관증 상으로 내원한 환자 중 내시경검사를 시행하여 CLO검사, 조직검사, 중합체 연쇄반응에 H. pylori 양성으로 확인된 70명의 양성 위십이지장질환(위궤양 14명, 십이지장궤양 14명, 비궤양성 소화불량증 42명)을 대상으로 cagA, vacA, iceA 유전자형을 PCR로 분석하였다. 결과: 검체의 91.4%
(64/70)에서 cagA 유전자 양성이었고, 소화성 궤양과 비 궤양성 소화불량증 차이를 발견할 수 없었다(96.4% vs.
88.1%, p=0.390). vacA s1 대립유전자가 대부분(59/70, 84.3%)으로 s1c형(39/59, 66.1%), s1a형(21/59, 35.6%)에서 양성이었으나 s1b형은 모든 환자에서 음성이었으며, vacA s1 양성 균주는 양군에서 차이를 발견할 수 없었다(78.6%
vs. 88.1%, p=0.283). 질병의 임상양상과 관계없이 vacA s1c/m1형이 가장 높은 비율(51.5%)로 나타났다. iceA1 유전 자는 91.4% (64/70), iceA2는 4.3% (3/70)으로 나타났으며, 양 군에서 차이를 발견할 수 없었다(89.3% vs 92.9%, p=0.601).
복합 유전자형에서는 vacA s1/cagA+/iceA1 유전자형이 87.9%
(51/58)으로 가장 높았으나 양군에서 의미 있는 차이는 없 었다(86.9% vs. 88.6%, P=1.000). vacA 및 cagA만 고려한다 면, vacA s1/cagA+은 양군에서 차이가 없었다(91.3% vs.
91.4%, p=0.987). vacA 및 iceA만 고려한다면, vacA s1/iceA1 은 양군에서 의미 있는 차이는 없었다(86.9% vs. 97.1%, p=0.290). cagA, vacA 그리고 iceA의 연관성을 보면 vacA 유전자 중 cagA 양성은 93.1%(54/58)였고 이중 96.3%
(52/54)에서 vacA s1을 가진 것으로 나타났으나 cagA와 vacA s1 사이에는 연관성이 없었다(p=0.219). 또한 iceA 유전자 중 cagA 양성은 93.1% (54/58)였고 이중 96.3%
(52/54)에서 iceA1을 가진 것으로 나타났으나 cagA와 iceA1 사이에는 연관성이 없었다(p=0.727). 결론: 양성 위십이 지장질환에서 cagA+ vacA s1c/m1 iceA1형이 국내에서 가 29
The Korean Journal of Gastroenterology: Vol. 40, No. 1, 2002
장 많은 빈도로 발견되었으나, cagA, vacA, iceA 양상은 소화성궤양과 비궤양성 소화불량증 환자군에서 차이를 보이지 않아 본 연구에서는 H. pylori 유전자형과 양성 위 십이지장질환의 중증도와는 연관성이 없는것으로 나타 났다.
색인단어: H. pylori, cagA, vacA, iceA
참 고 문 헌
1. Warren JR, Marshall BJ. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983;1:1273-1275.
2. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration.
Lancet 1984;1:131-135.
3. Graham DY. Helicobacter pylori infection in the pathogenesis of duodenal ulcer and gastric cancer: a model.
Gastroenterology 1997;113:1983-1991.
4. Graham DY and Yamaoka Y. H. pylori and cagA:
relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter 1998;
3:145-151.
5. Isaacson PG, Spencer J. Is gastric lymphoma an infectious disease? Hum Pathol 1993;24:569-570.
6. Wotherspoon AC. Gastric MALT lymphoma and Helicobacter pylori. Yale J Biol Med 1996;69:61-68 7. Eaton KA, Krakowkas. Effect of gastric pH on
urease-dependent colonization of gnotobiotic piglets by Helicobacter pylori. Infect Immun 1994;62:3604-3607.
8. Go MF, Graham DY. How does Helicobacter pylori cause duodenal ulcer disease: The bug, the host, or both. J Gastroenterol Hepatol 1994;9:S8-S10.
9. Lingwood CA, Wasfy G, Han H, Huesca M. Receptor affinity purification of a lipid-binding adhesion from Helicobacter pylori. Infect Immun 1993;61:2474-2478.
10. Knipp U, Birkholz S, Kaup W, Opferkuch W. Immune suppressive effects of Helicobacter pylori on human peripheral blood mononuclear cells. Med Microbiol Immunol 1993;182:63-76.
11. Malaty HM, Engstrand L, Pedersen NL, Graham DY.
Helicobacter pylori infection: Genetic and environmental influences. A study of twins. Ann Int Med 1994;120:982-986.
12. Blaser MJ. Helicobacter pylori phenotypes associated with peptic ulceration. Scand J Gastroenterol Suppl 1994;205:1-5.
13. Covacci A, Censini S, Bugnoli M, et al. Molecular
characterization of the 128-kDa immunodominant antigen of Helicobacter pylori associated with cytotoxicity and duodenal ulcer. Proc Natl Acad Sci 1993;90:5791-5795.
14. Cover TL, Glupczynski Y, Lage AP, et al. Serologic detection of infection with CagA+ Helicobacter pylori strains. J Clin Microbiol 1995;33:1496-1500.
15. Crabtree JE, Taylor JD, Wyatt JI, et al. Mucosal IgA recognition of Helicobacter pylori 120 kDa protein, peptic ulcer, and gastric pathology. Lancet 1991;338:332-335.
16. Xiang Z, Censini S, Bayeli PF, et al. Analysis of expression of CagA & VacA virulence factors in 43 strains of Helicobacter pylori reveals that clinical isolates can be divided into two major types and that CagA is not necessory for expression of the vacuolating cytotoxin. Infect Immun 1995;63:94-98.
17. Atherton JC, Cao P, Peek RM Jr, Tummuru R, Blaser MJ, and Cover TL. Mosaicism in vacuolating cytotoxin alleles of Helicobacter pylori. Association of specific vacA types with cytotoxin production and peptic ulceration. J Biol Chem 1995;270:17771-17777.
18. Atherton JC, Twells RJ, Hawkey CJ, Peek MK, Cover TL, and Blaser MJ. New, internationally applicable, polymerase chain reaction based typing of Helicobacter pylori vacA.
Gastroenterology 1997;112(suppl):A61.
19. Atherton JC, Peek RM Jr, Tham KT, Cover TL, and Blaser MJ. Clinical and pathological importance of heterogeneity in vacA, the vacuolating cytotoxin gene of Helicobacter pylori. Gastroenterology 1997;112:92-99.
20. Sensini S, Lange C, Xiang Z, et al. cag, a pathogenicity island of Helicobacter pylori, encodes type 1-specific and disease-associated virulence factors. Proc Natl Acad Sci 1996;93:14648-14653.
21. Crabtree JE, Covacci A, Farmery SM, et al. Helicobacter pylori induced interleukin-8 expression in gastric epithelial cells is associated with CagA positive phenotype. J Clin Pathol 1995;8:41-45.
22. Sharma SA, Tummuru MKR, Miller GG, Blaser MJ.
Interleukin-8 response of gastric epithelial cell lines to Helicobactor pylori stimulation in vitro. Infect Immun 1995;63:1681-1687.
23. Peek RM Jr, Thompson SA, Atherton JC, Blaser MJ, and Miller GG. Expression of a novel ulcer-associated H. pylori gene, iceA, following adherence to gastric epithelial cells.
Gastroenterology 1996;110(suppl.):A225.
24. Peek RM Jr, Thompson SA, Donahue JP, et al. Adherence to gastric epithelial cells induces expression of a Helicobacter pylori gene, iceA, that is associated with clinical outcome.
30
Park, et al. cagA, vacA, and iceA Status of H. pylori in Benig Gastroduodenal Diseases
Proc Assoc Am Phys 1998;110:531-544.
25. van Doorn LJ, Figueiredo C, Sanna R, et al. Clinical relevance of the cagA, vacA, and iceA status of Helicobacter pylori. Gastroenterology 1998;115:58-66.
26. van Doorn LJ, Figueiredo C, Sanna R, et al. Expanding alleic diversity of Helicobacter pylori vacA. J Clin Microbiol 1998;36:2597-2603.
27. Ching CK, Wong BC, Kwok E, Ong L, Covacci A, Lam SK. Prevalence of CagA-bearing Helicobacter pylori strains detected by the anti-CagA assay in patients with peptic ulcer disease and in controls. Am J Gastroenterol 1996;91:
946-953.
28. Kim KC, Park HJ, Lee HW, et al. Relation of serum gastrin and pepsinogen levels to serologic recognition of CagA and VacA in Helicobacter pylori infection. Korean J Gastroenterol 1997;29:25-34.
29. Kim JW, Chung KS. Serologic recognition of VacA and CagA in children with Helicobacter pylori infection. Korean J Gastroenterol 1998;31:167-174.
30. Kim DY. The positive rates of Helicobacter pylori cagA gene in gastric biopsy specimens of the patients with gastritis, gastric ulcer, duodenal ulcer, and gastric cancer and comparison of the degree of gastritis. Korean J Gastroenterol 1998;32:24-31.
31. Kim JG, Do JH, Kim HJ, Park JW, Park SM. CagA gene detection in H . pylori strains isolated from korean upper gastrointestinal disease. Korean J Gastroenterol 1996;28(suppl 2):116.
32. 김재규, 박중원, 장세경, 유병철, 박실무. 한국인에서 cagA 유전자 발현율과 상부위장관 질환과의 관계. 대한내과학회 지 1997;53(suppl 1):71.
33. Park IS, Lee SI, Park HJ. Diagnosis of Helicobacter pylori using polymerase chain reaction and relation between cagA and severity of gastritis. Korean J Gastroenterol 1998;31:
281-289.
34. Son HJ, Kim JJ, Lee HY, et al. Detection of cagA gene in Helicobacter pylori strains isolatedfrom gastrodudenal diseases. Korean J Gastroenterol 1999;33:590-594.
35. Yang US, Song GA, Kang DH, Park SK, Song CS, Cho M.
The prevalence of cagA+ Helicobacter pylori in the peptic ulcer diseases. Korean J Gastroenterol 1998;31:184-191.
36. Lee YC, Kim BS, Park HJ, et al. Prevalence of seropositivity to CagA and VacA in Helicobacter pylori infected Korean patients using commercial Western blot kit (Helicoblot2.0TM). Korean J Gastroenterol 1998;31:
432-440.
37. 정현채, 김정목, 이주영, 송인성, 김정룡. Helicobacter pylori의 병리인자와 상부위장관 질환과의 관계: cagA 또는 cytotoxin 표현균주로 감염시킨 인체 위상피세포에서의 cytokine 유전 자의 발현 양상. 대한내과학회지 1995; 47(suppl 1):7.
38. Park SM, Park J, Kim JG, et al. Infection with Helicobacter pylori expressing the cagA gene is not associated with an increased risk of developing peptic ulcer disease in Korean patients. Scand J Gastroenterol 1998;33:923-927.
39. Lage AP, Godfroid E, Fauconnier A, et al. Diagnosis of Helicobacter pylori infection by PCR: Comparison with other invasive techniques and detection of cagA gene in gastric biopsy specimens. J Clin Microbiol 1995;33:2752-2756.
40. Peek RM Jr, Miller GG, Tham KT, et al. Detection of Helicobacter pylori gene expression in human gastric mucosa. J Clin Microbiol 1995;33:28-32.
41. Wang HJ, Kuo CH, Yeh AA, Chang PC, and Wang WC.
Vacuolating toxin production in clinical isolates of Helicobacter pylori with different vacA genotypes. J Infect Dis 1998;178:207-212.
42. Yamaoka Y, Kodama T, Gutierrez O, Kim JG, Kashima K, Graham DY. Relationship between Helicobacter pylori iceA, cagA, and vacA status and clinical outcome: studies in four different countries. J Clin Microbiol 1999;37:2274-2279.
43. van Doorn LJ, Figueiredo C, Sanna R, et al. Geographic distribution of vacA alleic types of Helicobacter pylori.
Gastroenterology 1999;116:823-830.
44. van Doorn LJ, Figueriedo C, Carneiro F, et al. Worldwide heterogeneity of the Helicobacter pylori vacA gene. Gut 1997;41(suppl 1):A34.
45. Ito Y, Azuma T, Ito S, et al. Analysis and typing of the vacA gene from cagA-positive strains of Helicobacter pylori isolated in Japan. J Clin Microbiol. 1997;35:1710-1714.
46. Pan ZJ, Berg DE, van der Hulst RW, et al. Prevalence of vacuolating cytotoxin production and distribution of distinct vacA alleles in Helicobacter pylori from China. J Infect Dis 1998;178:220-226.
47. Ito Y, Azuma T, Ito S, et al. Sequence analysis and clinical significance of the iceA gene from Helicobacter pylori strains in Japan. J Clin Microbiol. 2000;38:483-488.
48. Ilver D, Arnqvist A, Ogren J, et al. Helicobacter pylori adhesion binding fucosylated histo-blood group antigens revealed by retagging. Science 1998;279:373-377.
49. Zheng PY, Hua T, Yeoh KG, Ho B. Association of peptic ulcer with increased expression of Lewis antigens but not cagA, iceA, and vacA in Helicobacter pylori isolates in a Asian population. Gut 2000;47:18-22.
31