ABSTRACT
The purpose of this case report is to describe the considerations in surgical orthodontic treatment of a patient with skeletal Class III malocclusion and potential airway problem. A 30-year-old female patient showed skeletal Class III malocclusion and a narrow airway space. After presurgical orthodontic treatment, the bimaxillary orthognathic surgery with bimaxillary anterior segmental osteotomy was done to move the posterior segment of the maxilla forward and reduce the amount of mandibular setback. The remaining extraction space was closed during the postoperative orthodontic treatment. After the orthodontic treatment, proper overjet and overbite were obtained and the protruded mandible was corrected. The airway space increased postoperatively compared to the preoperative condition. In patients with Class III malocclusion who have predisposing factors or present symptoms of obstructive sleep apnea (OSA) or who have been diagnosed with OSA, consideration to minimize reduction of the airway space is necessary in treatment planning. (Clin J Korean Assoc Orthod 2020;10(1):55-67)
Key words Surgical orthodontics, Orthognathic surgery, Anterior segmental osteotomy, Airway, Class III
골격성 III급 부정교합 환자의 양악 Anterior Segmental Osteotomy를 동반한 양악 수술교정 치험례
임근오,
1박지훈,
1안정섭
21
서울대학교 치의학대학원 치과교정학교실
2
서울대학교치과병원 치과교정과
Bimaxillary Surgical Orthodontic Treatment Combined with Bimaxillary Anterior Segmental Osteotomy of Skeletal Class III
Malocclusion Patient: Case Report
Keunoh Lim,
1Ji-Hoon Park,
1Jung-Sub An
21
Department of Orthodontics, School of Dentistry, Seoul National University, Seoul, Korea
2
Department of Orthodontics, Seoul National University Dental Hospital, Seoul, Korea
Dr. 박 지 훈 Dr. 임 근 오
Corresponding author: Jung-Sub An Department of Orthodontics, Seoul National University Dental Hospital, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-2072-4470 Fax: +82-2-2072-3817 Email: [email protected] Received: February 17, 2020 / Revised: February 29, 2020 / Accepted: March 1, 2020
Dr. 안 정 섭
서론
교정치료의 목표는 심미적일 뿐만 아니라 최적의 기 능을 발휘할 수 있는 치열 및 안모를 달성하는 데 있 다. 이 기능에는 저작, 발음뿐 아니라 원활한 호흡도 포 함되며 특히 최근 교정치료와 관련한 환자의 기도 공간 변화가 주목을 받고 있다.
1,2골격성 III급 부정교합의 전형적인 수술 교정치료는 비발치 또는 상악 소구치 발치를 동반한 술전 교정치 료가 진행된 뒤 턱교정 수술을 통한 상·하악 복합체 (maxillomandibular complex)의 시계방향 회전을 동 반한 하악골의 후퇴(setback)가 이루어지며, 필요에 따 라 턱끝성형술(genioplasty)이 동반된다. 이때 환자의 안모를 개선하기 위해 하악골의 후퇴가 상당량 이루어 지게 되는 경우가 있다. 턱교정 수술 시 하악골을 후퇴 시킬 경우 인두 기도 공간(pharyngeal airway space) 이 감소된다는 보고들이 있으며,
3-7이는 골뿐 아니라 연관된 근육 및 연조직이 후퇴하고 혀의 위치가 변하기 때문으로 생각된다.
6,7이와 같은 기도 공간의 감소는 수 면 무호흡(obstructive sleep apnea)의 소인으로 여겨 지므로,
8,9III급 부정교합 환자의 수술 교정 치료계획 수립 시 기도 공간에 대해서도 고려할 필요가 있다.
수술 후 기도 공간이 과도하게 좁아질 것으로 예상 되는 III급 부정교합 환자의 치료 시 하악 소구치를 발 치하여 발치 공간을 폐쇄하면 하악 전치가 후방 이동 되는 만큼 하악 후퇴량을 줄일 수 있다. 교정적으로 하 악 발치 공간을 폐쇄할 경우 이미 보상(compensation) 되어 있는 하악 전치가 지나치게 설측 경사될 우려가 있으나, 전방부 분절골절단술(anterior segmental osteotomy; ASO)를 병행하여 수술적으로 하악 전방 분절을 후방 이동시킨다면 이를 최소화할 수 있다. 또 한 상악의 경우도 상악 소구치를 발치하고 ASO를 통 해 후방 분절을 전방 이동시킨다면 기도 공간을 더욱 확보할 수 있을 것이다.
본 증례에서는 골격성 III급 부정교합과 좁은 기도를 가진 환자에서 상·하악 ASO와 양악 수술을 동반한 수 술 교정치료를 진행하였다. 이 증례를 통해 III급 부정 교합의 수술 교정치료 시 기도 공간과 관련한 고려사항 에 대해 고찰해 보고자 한다.
진단
30세 9개월 여자 환자가 구강내과로부터 앞니가 서 로 닿지 않는다는 주소로 치과교정과에 의뢰되었다.
환자는 임상검사 시 하악 돌출에 따른 오목한 측모 (concave profile) 및 우측으로의 비대칭을 보였고, 구 내 검사 시 III급 구치 관계, 전치부 개방교합 및 하악 전치부에 약간의 크라우딩이 관찰되었다(Figure 1). 환 자의 상악 우측 제2대구치는 결손되었는데(Figure 2), 이전에 매복된 제3대구치에 의한 제2대구치의 치근 외 흡수가 심해 구강악안면외과에서 두 치아를 함께 발치 한 과거력이 있었다.
측면 두부계측방사선사진 분석 결과 SNA 86.4°, SNB 86.3°, ANB 0.1°, mandibular body to anterior cranial base 1.2로 상대적으로 긴 하악체 길이에 의한 골격성 III급 부정교합을 보였다. 수직적으 로는 SN-MP angle 27.9°, facial height ratio 73.1%
로 저발산형 안모(hypodivergent pattern)를 보였다.
치열은 U1 to FH 117.1°, U1 to SN 110.6°, IMPA 90.0
°로 상·하악 전치는 기저골에 대해 정상 경사를 보였다
(Table 1). 또한 측면 두부계측방사선사진에서 환자의
기도가 일반적인 경우에 비해 다소 좁은 양상을 보임
을 관찰할 수 있었다. 정면 두부계측방사선사진에서 양
측 greater wing inferior orbit을 잇는 선과 이 선의
수직 이등분선을 각각 수평기준선, 수직기준선으로 설
정 후 계측한 결과
10교합평면의 횡적 회전(transverse
roll of occlusal plane)을 동반한 우측으로의 비대
칭을 확인하였으며 발달된 하악 우각부가 관찰되었다
Figure 2. Pretreatment panoramic radiograph.
Figure 1. Pretreatment facial and intraoral photographs.
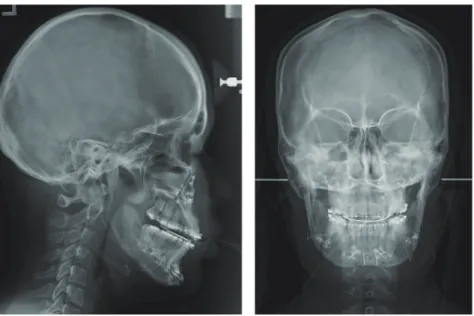
Figure 3. Pretreatment cephalometric radiographs.
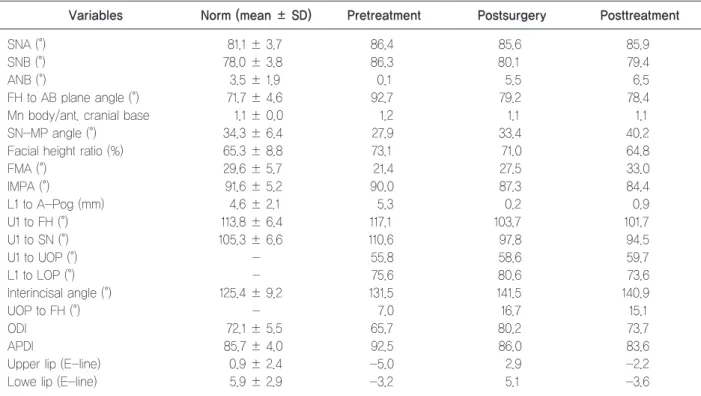
Table 1. Cephalometric measurements
Variables Norm (mean ± SD) Pretreatment Postsurgery Posttreatment
SNA (°) 81.1 ± 3.7 86.4 85.6 85.9
SNB (°) 78.0 ± 3.8 86.3 80.1 79.4
ANB (°) 3.5 ± 1.9 0.1 5.5 6.5
FH to AB plane angle (°) 71.7 ± 4.6 92.7 79.2 78.4
Mn body/ant. cranial base 1.1 ± 0.0 1.2 1.1 1.1
SN-MP angle (°) 34.3 ± 6.4 27.9 33.4 40.2
Facial height ratio (%) 65.3 ± 8.8 73.1 71.0 64.8
FMA (°) 29.6 ± 5.7 21.4 27.5 33.0
IMPA (°) 91.6 ± 5.2 90.0 87.3 84.4
L1 to A-Pog (mm) 4.6 ± 2.1 5.3 0.2 0.9
U1 to FH (°) 113.8 ± 6.4 117.1 103.7 101.7
U1 to SN (°) 105.3 ± 6.6 110.6 97.8 94.5
U1 to UOP (°) - 55.8 58.6 59.7
L1 to LOP (°) - 75.6 80.6 73.6
Interincisal angle (°) 125.4 ± 9.2 131.5 141.5 140.9
UOP to FH (°) - 7.0 16.7 15.1
ODI 72.1 ± 5.5 65.7 80.2 73.7
APDI 85.7 ± 4.0 92.5 86.0 83.6
Upper lip (E-line) 0.9 ± 2.4 -5.0 2.9 -2.2
Lowe lip (E-line) 5.9 ± 2.9 -3.2 5.1 -3.6
(Figure 3). 이러한 문제 목록을 종합하여 환자는 전치 부 개방교합, 안면 비대칭이 동반된 골격성 III급 부정 교합으로 진단하였다.
치료계획
우선적으로 턱교정 수술을 동반한 교정치료를 계획 하였다. 초진 시 크라우딩이 심하지 않았으며 두개저에 대한 상악 전치 각도 및 상악 교합평면에 대한 상악 전 치 각도가 크게 나쁘지 않아(U1 to SN 110.6°, U1 to UOP 55.8°)(Table 1) 상악 소구치는 발치하지 않기로 하였다. 상실된 상악 우측 제2대구치는 교정치료 후 임 플란트 보철치료를 통해 회복하기로 하였다.
환자의 초진 시 주소가 개방교합이었기 때문에 골 고 정원을 이용한 구치부 압하 및 하악 치열의 후방 이동 을 통한 비수술 절충치료계획도 수립해 두었으나, 상담
결과 환자는 턱교정 수술을 통한 안모의 개선까지 원하 여 수술 교정치료를 진행하기로 하였다.
치료경과 및 결과
상·하악에 MBT prescription의 0.022-inch slot 세라믹 자가결찰 브라켓(Clippy-C, Tomy, Tokyo, Japan)을 부착하여 고정식 교정치료를 개시하였다. 치 료 시작 시부터 상악 좌측 제2대구치의 협측 경사를 적극적으로 개선하기 위해, 상악 좌측 제1대구치와 제 2대구치 사이 구개측 치은에 교정용 미니 임플랜트를 식립하고 상악 제2대구치와 탄성 체인으로 연결하였 다. 환자의 크라우딩이 심하지 않은 편이었으며 arch coordination 또한 치료 전부터 적절하였던 상황이었 기 때문에 약 4개월간의 술전 교정치료를 진행하여 수 술 준비를 완료하였다(Figure 4).
Figure 4. Presurgical facial and intraoral photographs.
Surgical treatment objective를 통해 상·하악골의 시계방향 회전을 동반한 하악의 후퇴를 포함하는 통상 적 수술 계획을 수립하였다. 이와 같은 계획하에서 예 상되는 하악골의 후퇴량은 약 11 mm였다(Figure 5).
그러나 수술 계획을 구강악안면외과와 논의하는 과 정에서 환자의 기도가 좁아 하악의 후퇴량이 크면 술 후 수면 무호흡 발생이 우려되므로 수술 계획의 변경 이 필요하다는 결론을 내렸다. 이에 따라 수술 시 상·
하악 제1소구치를 발치하고 상악 ASO를 시행하여 상 악의 후방 분절을 전방 이동시켜 기도 공간을 확보하 고, 하악 ASO를 통해 전방 분절을 후방 이동시켜 하악 골의 후퇴량을 줄이는 것으로 계획을 수정하였다. 교합 평면의 횡적 회전을 개선하기 위해 상악골의 좌측을 우 측보다 상방 이동시키고, 하악 돌출에 따른 concave profile을 개선하기 위해 상악 후방부를 전방부에 비 해 상방 이동시키면서 하악을 후퇴시키기로 하였다. 턱 끝성형술을 통해 턱끝을 후방 이동시켜(setback) 하악 의 ASO에 따른 턱끝의 지나친 돌출양상을 방지하고, 길이를 감소시켜(reduction) 안면 고경을 감소시키기로
하였다. 또한 기도 공간의 부가적 확보를 위한 inferior turbinectomy 및 reduction glossectomy와 심미적 개선을 위한 angle reduction을 함께 진행키로 하였다 (Table 2).
환자에게 소구치 발치를 포함한 수술 계획 변경을 사 전고지하고 턱교정 수술을 진행하였다. 수술 시 치근 의 손상을 우려하여 소구치 발치 공간은 일부 남긴 채 로 폐쇄하였다(Figure 6). 수술 후 상악골의 차등적 상 방 이동으로 상악골의 횡적 회전과 두개저에 대한 교합 평면의 경사도가 개선되었고, 하악골의 차등적 후퇴를 통해 하악의 돌출양상이 감소되었으며 턱끝의 우측 편 위도 함께 개선되었음을 확인할 수 있었다(Figure 7, Table 1). 또한 angle reduction으로 환자의 하악 우각 부 부피가 감소하였다(Figure 7). 수술 전후 측면 두부 계측방사선사진 중첩을 통해 상악 후방 분절이 5 mm 전방 이동되었고, 하악 후퇴량은 7 mm로 초기 수술 계획에 비해 감소했음을 확인할 수 있었다(Figure 8).
수술 1개월째 술후 교정을 시작하였다(Figure 9). 수 술 직후 약한 힘의 수직적 고무줄을 이용해 교합을 긴 밀하게 형성한 뒤 배열 및 레벨링을 진행하여 0.019 × 0.025-inch 스테인리스강 와이어상에서 잔여공간을 폐쇄하였다. 이후 마무리 과정을 거쳐 치료 32개월째에 상·하악 설측에 고정식 유지장치를 부착하고 고정식 교
Figure 5. Initial surgical treatment objective (STO). The black line represents pretreatment and the red line depicts initial STO.
Table 2. Orthognathic surgery plan Maxilla Le Fort I osteotomy
A nterior segmental osteotomy (#14, 24 extraction)
Canting correction: #23 1.0 mm impaction Posterior impaction: 6.0 mm
Bodily setback 3.0 mm
Mandible Sagittal split ramus osteotomy (setback) Anterior segmental osteotomy (#34, 44 extraction)
Others Genioplasty (setback and reduction) Inferior turbinectomy
Reduction glossectomy
Angle reduction
Figure 6. Postsurgical panoramic radiograph.
Figure 7. Postsurgical cephalometric radiographs.
정장치를 제거한 뒤 상·하악 가철식 유지장치를 적용하 였다. 고정식 유지장치는 발치 공간의 재발을 막기 위 해 제2소구치까지 연장하였다.
치료 후 상·하악 치열은 조화롭게 배열되었고 적절한 수직피개 및 수평피개를 형성할 수 있었다. 또한 I급 구 치관계를 달성하였으며 치열 정중선은 일치하였다. 치 료 전과 비교하여 하악 돌출 경향이 감소하였고, 하악 각 부위도 심미적으로 개선되었다. 다만 수술을 통해 턱끝을 후퇴시켰음에도 턱끝 부위의 돌출감은 잔존하 였다(Figure 10). 치료 전후 측면 두부계측방사선사진 중첩을 통해 상악골 후방부의 상방 이동을 통한 상·
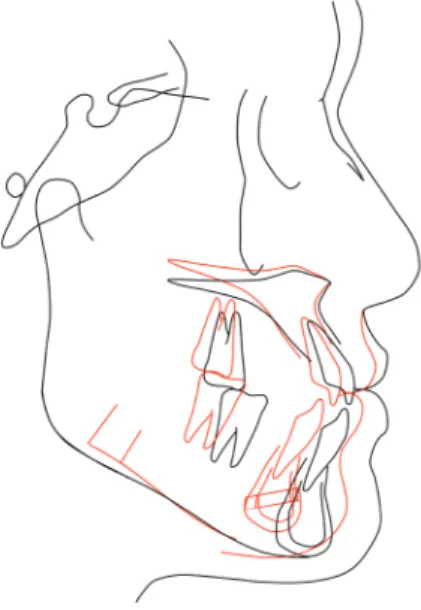
하악골의 시계방향 회전 및 하악골의 후방 이동을 통 해 골격성 III급 양상 해소되었고, 상악 후방 분절이 전 방 이동 되었음을 확인할 수 있었다(Figures 11, 12, Table 1). 치료 후 파노라마방사선사진 상에서 약간의 상악 전치부 치근 흡수가 관찰되었으며, 이는 공간폐쇄 Figure 8. Superimposition of presurgical, postsurgical trac-
ings and initial surgical treatment objective (STO). The black line, red line, and green line represents presurgical tracing, postsurgical tracing, and initial STO, respectively.
Figure 9. Facial and intraoral photographs at 1 month after the orthognathic surgery.
Figure 10. Posttreatment facial and intraoral photographs.
Figure 11. Posttreatment cephalometric radiographs.
시 상악 전치의 경사를 유지하기 위해 호선상에 설측 치근 토크를 부여한 영향으로 생각된다(Figure 13).
3D imaging software (Invivo 5, Anatomage, San Jose, CA, USA)를 사용해 수술 전과 수술 후 6개 월 전산화단층촬영(computerized tomography; CT) 영상에서 이전에 보고된 연구와 유사한 방법으로 기도 를 세 구획으로 나누어(nasopharynx, oropharynx,
and hypopharynx) 부피를 계측하였다.
11환자의 두부 를 FH plane에 평행하도록 재설정한 뒤 시상면상에서 Vp(ala of vomer의 최후방점)와 PNS를 연결한 평면 을 기도의 상방 한계로 설정하고, CV4(4번째 경추의 최 전하방점)를 지나면서 FH plane에 평행한 평면을 기도 의 하방 한계로 설정하였다. CV1(anterior arch of the atlas의 최전하방점)을 지나면서 FH plane에 평행한 평면을 nasopharynx와 orophyarynx의 경계, CV2(2 번째 경추의 최전하방점)를 지나면서 FH plane에 평행 한 평면을 oropharynx와 hypopharynx의 경계로 설 정하였다(Figure 14). 그 결과 수술 후 6개월째에 수술 전에 비해 모든 기도 구획에서의 부피가 증가하였음을 확인할 수 있었다(Table 3).
고찰
III급 부정교합 환자의 턱교정 수술에 수반되는 하악 의 후퇴가 인두 기도 공간을 줄이며 이로 인해 수면 무 호흡의 위험성이 증가될 수 있음을 우려하는 보고들 이 있다.
4-7그러나 상악의 수술이 포함되는 경우 상악 의 전진(advancement)이 이를 어느 정도 보상한다는 연구도 있으며
12-14심지어 상·하악을 모두 수술할 경우 Figure 12. Superimposition of pretreatment and posttreatment
tracings. The black line represents pretreatment and the red line depicts posttreatment.
Figure 13. Posttreatment panoramic radiograph.
기도 공간이 수술 전보다 증가함을 보고한 경우도 있
다.
15,16연구들 사이에 보이는 이 같은 차이들은 다양한
환자의 골격적 차이에 따른 수술 방향 및 양의 차이에 기인하였을 것으로 생각된다. 기도 공간 감소가 수면 무 호흡과 직접적 관련이 있다는 명확한 증거는 아직 없으 나,
17턱교정 수술 시 하악의 후퇴량이 컸거나,
6,17고령의 비만 환자에서 하악 후퇴 수술을 시행한 후 수면 무호 흡이 발생하였다는 보고도 있어
18주의할 필요가 있다.
골격성 III급 부정교합의 수술 교정치료에서 하악 의 후퇴량을 줄이기 위하여 하악 제1소구치 발치 및 ASO를 시행하는 방법을 고려할 수 있는데 본 증례 의 경우 구치부 III급 관계로 마무리하게 되면 상·하악 의 심한 너비 부조화가 예상되었고, 이를 개선하기 위 해 2-piece osteotomy를 시행하여 수술적으로 상악 을 확장할 경우 안정성이 저하될 것이 우려되었다.
19또 한 상악골의 전방이동을 통해 하악 후퇴로 인한 기도 공간 감소를 보상하는 것을 고려하였으나, 상악골을 전 체적으로 전진시킬 경우 안모 악화가 우려되었다. 따라 서 상·하악 모두 제1소구치를 발치하고 ASO를 시행 하여 하악 후퇴량을 줄였으며 상악의 후방 분절을 전 방 이동하여 결과적으로 전체적인 기도 공간을 증가 시켰고, 구치부 I급 관계로 마무리하여 적절한 arch coordination을 달성하였다.
수술 시 인접치의 치근 손상이 우려되어 발치 공간을 일부 남겨두고 공간을 폐쇄하였고 술후 교정치료 중 공
간폐쇄 과정에서 구치부의 정출로 하악평면각이 다소 증가하였으나(Table 1), 결과적으로는 하악의 추가적 후하방 회전으로 턱끝의 돌출도를 수술 직후에 비하여 조금 더 감소시킬 수 있었다.
III급 부정교합을 가진 한국인의 경우 상악을 전진시 키면 안모의 악화를 초래하는 경우가 많은데,
6본 증례 와 같이 상악의 ASO를 동반하여 후방 분절을 전방 이 동시킬 경우 안모의 악화를 막으면서도 기도 공간을 확 보할 수 있다는 장점이 있다. 그러나 ASO를 동반한 하 악 후퇴량의 감소는 경우에 따라 덜 심미적인 결과로 이어질 수 있다. 하악 전방 분절이 후방 이동되면서 생 기는 하악골 전연의 step은 마치 수술로 턱끝을 전방 이동시킨(advance genioplasty) 효과가 나타나며 하 악 후퇴량의 감소와 더불어 수술 후 턱끝의 돌출감 잔 존을 야기할 수 있다. 본 증례에서도 수술 계획 수립 시 이와 같은 문제를 방지하기 위해 턱끝의 후방 이동 (setback genioplasty)을 계획하였지만 결과는 충분치 않아 턱끝의 돌출감이 다소 남아 있었다.
따라서 이와 같은 수술 계획의 변경은 심미와 기능을 Table 3. Changes in airway volume after orthognathic
surgery
Location
Volume (mL)
Presurgery 6 months after surgery
Nasopharynx 7.5 10.2
Oropharynx 2.4 4.5
Hypopharynx 4.0 6.1
Total volume 14.0 20.8
Figure 14. Airway analysis using computed tomography (CT)
images. CV1: the most anterior inferior point of the anterior
arch of the atlas, CV2: the most anterior inferior point of the
body of the 2nd cervical vertebra, CV4: the most anterior in-
ferior point of the body of the 4th cervical vertebra, Vp: the
most posterior point of the ala of the vomer.
견주어 신중히 결정될 필요가 있으나 환자의 원활한 호 흡을 방해하지 않는 충분한 기도 공간 및 이를 위한 수 술량에 대한 명확한 지침은 아직 없으며 술자, 특히 수 술을 집도하는 외과의의 경험에 의존하는 경향이 크다.
다만 비만, 고령, 짧은 목, 큰 혀, 큰 구개수(uvula), 심 한 낮 시간의 졸림 및 심한 코골이 등 수면 무호흡의 소 인 및 증상을 가지고 있거나
11,20수면 무호흡으로 진단 을 받은 환자는 가급적 하악 후퇴량을 줄이고 상악을 전진시키거나 ASO를 통해 상악 후방 분절을 전진시켜 기도 공간을 침해하지 않는 방향의 수술 계획을 검토 할 필요가 있다고 생각된다. 이를 위해서는 초진 시부 터 문진 또는 설문을 통해 환자의 기도와 관련된 기능 적 문제를 적극적으로 파악하고, 필요시 수면다원검사 (polysomnography) 등을 통한 평가를 거쳐 치료계획 을 수립해야 할 것이다.
결론
수술 후 수면 무호흡이 우려되는 골격성 III급 부정교 합 환자의 경우 기도 공간의 침해를 최소화하는 치료계 획을 검토할 필요가 있으며, 턱교정 수술 시 상악 후방 분절의 전진 및 하악 후퇴량 감소를 위해 상·하악 ASO 를 동반한 턱교정 수술을 고려해 볼 수 있을 것이다.
REFERENCES