CONTENTS
Ⅰ. INTRODUCTION
Ⅱ. MATERIALS AND METHODS
Ⅲ. RESULTS
Ⅳ. DISCUSSION
Ⅴ. CONCLUSIONS REFERENCES KOREAN ABSTRACT
Ⅰ. INTRODUCTION
Myofascial pain syndrome is a muscular pain disorder which is the most common diagnosis causing chronic pain. It is a regional myogenous pain condition characterized by local areas of firm, hypersensitive bands of muscle tissue known as a trigger points.
Trigger points can range from 2 to 5 mm in diameter and evoke referred pain and local twitch response.
1)The autonomic symptoms including vasoconstriction, sweating, and pilomotor response are described in the patients with myofascial trigger points.
2)Prevalence of trigger points can be explained by the epidemiologic study of myofascial pain syndrome (MPS). Fishbain et al.
3)reported that 85%
of 283 chronic pain patient had a primary diagnosis of MPS. Fricton et al.
4)found 54.6% of 296 head and neck patient had a primary diagnosis of MPS. Sola
et al.
5)found the prevalence of one or more hypersensitive points in the shoulder and neck muscles to be about 50% in normal subjects.
Dry needling without any injection of drugs has been used one of the effective treatment of myofascial trigger points.
6)-9)The immediate or permanent analgesic effects by needling without any medication have been reported by many clinical trials.
10)-14)It is suspected that analgesic effect appears to be mediated by the input into the central nervous system during needle stimulation. But there was no rigorous evidence that needling therapies have an effect beyond placebo in myofascial trigger point pain. So, an investigation on the objective changes of myofascial trigger point during dry needling is needed.
Many reports agree that spontaneous electrical activity is found in trigger points of resting muscle.
15)-20)This electrical activity is highly localized in depth and stable during recording time.
17)But the source of this activity is controversial.
Spontaneous electrical activity is different from the electrical activity from local twitch response at the trigger point area. Spontaneous electrical activity is suspected to originate from the motor structure such as motor endplate
15),16)or muscle spindle
17)-19)whereas local twitch responses originate from the nervous system
21)by snapping stimulation of trigger point. Spontaneous electrical activity from myofascial trigger points can be recorded by
Effect of Dry Needling on Subjective Pain and EMG Activity of Myofascial Trigger Points
Jin-Woo Chung, D,D,S.,Ph,D,
Department of Oral Medicine and Diagnosis College of Dentistry, Kangnung National University
insertion of needle electrode into a certain depth of the trigger point, but there are no specific electrical signals recorded at the same depth in the adjacent non-tender area.
17),18)Insertion of needle electrode for EMG examination can be a form of dry needling, so the investigation on the changes of the electrical activity during needle advancing and withdrawing through the trigger point area can provide some evidences of needling effect on the trigger point.
This study was performed to investigate the needling effect on the immediate pain and spontaneous electrical activity of myofascial trigger point area by recording subjective pain and EMG amplitude during advancing and withdrawing the monopolar needle electrode through the myofascial trigger point.
Ⅱ. MATERIALS AND METHODS 1. Subjects
Eight subjects (4 males and 4 females, 33.0 ± 4.9 years old) who have active trigger points in their trapezius muscles have been recruited. Trigger point was located by manual palpation according to the criteria of Travell and Simons.
1)The pain by palpation was moderate to severe, and was referred or radiated to the adjacent neck and head areas.
Taut bands were observed by palpation in association with the trigger point.
Trigger point was confirmed by measuring pressure pain thresholds (PPTs) both trigger points and adjacent non-tender area. The adjacent non-tender area was the same muscle site which was absent of the above described symptoms. The PPTs were measured three times on each sites and averaged. The mean and standard deviation of PPTs on the trigger points (3.2 ± 0.8 kg/cm
2) was significant lower than adjacent non-tender area (4.2
± 1.0 kg/cm
2) confirming the manual palpation method for trigger point selection (p<0.01, paired t-test).
2. Equipment
Electromyographic (EMG) signals were recorded with 50 mm monopolar TECA disposable EMG needles, amplified with Model 7P511 amplifiers (Grass Instrument, MA, USA). Sampling frequency was 10 kHz and signals were digitized at 12 bits for 1.6 second. Each EMG epochs were stored, and processed by TestPoint program (Keithly, OH, USA).
Pressure pain thresholds were measured with an algometer (Pain Diagnostics and Thermography, NY, USA).
3. Protocol
Each subject was asked to relax and not move his or her shoulders during the experiments.
Monopolar needle was inserted into the skin directly overlying the identified trigger point. The needle was advanced in small increments until the action potentials were detected on the oscilloscope.
When the action potentials were observed from the needle electrode in the presumed trigger point, the subject was asked to his or her subjective pain in verbal pain scale, then an EMG epoch of 1.6 second was recorded. Each individual EMG epoch was converted into a root mean square amplitude.
The electrode was continued to advance in small increments to the possible depth which was maximum needle length or until the electrode could contact the bone. Then, the needle was withdrawn in small increments until the same depth at which the action potentials were recorded during needle advancing. When the needle electrode was withdrawn to the same depth, the subject's pain and EMG epoch was recorded.
4. Statistical analyses
The mean PPT values of trigger points and
adjacent non-tender areas of each subjects were
compared using paired t-test in order to confirm
the localization of the trigger point. Paired t-test of
verbal pain scale before and after dry needling, and root mean square values of EMG amplitude before and after needling were performed respectively.
Statistical analyses were performed at 5%
significant level.
Ⅲ. RESULTS
The action potentials of spontaneous electrical activities were recorded at certain depth in the presumed trigger point during advancing the needle in all 8 subjects. When the needle was further advanced in few millimeters from the depth, the action potentials were disappeared.
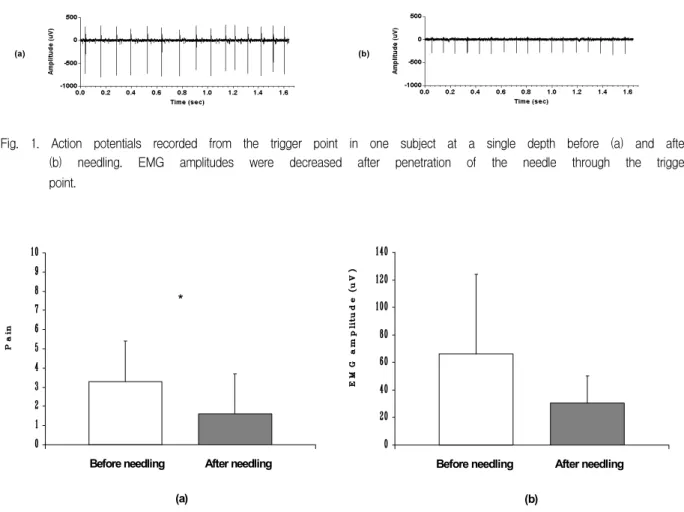
During withdrawing the needle, the action potentials of spontaneous electrical activity was also recorded in 6 of 8 subjects. Two of 8 subjects were recorded no specific large action potentials of spontaneous electrical activity during withdrawing the needle (Table 1). The depth of spontaneous electrical activity during needle withdrawing was almost same as the depth of spontaneous electrical activity during needle advancing. Fig. 1 shows typical action potentials recorded when needle advancing (before needling) and withdrawing (after needling) at
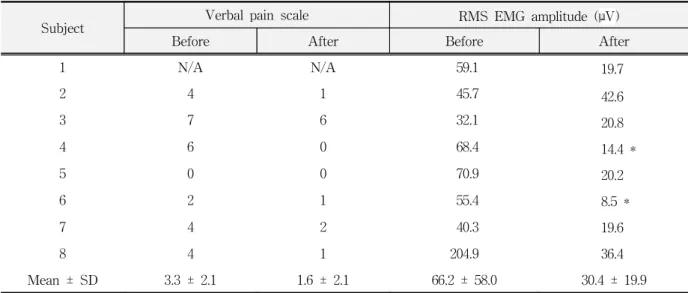
Table 1. Subjective pain and RMS EMG amplitude before and after needling.
Subject Verbal pain scale RMS EMG amplitude (μV)
Before After Before After
1 N/A N/A 59.1 19.7
2 4 1 45.7 42.6
3 7 6 32.1 20.8
4 6 0 68.4 14.4 *
5 0 0 70.9 20.2
6 2 1 55.4 8.5 *
7 4 2 40.3 19.6
8 4 1 204.9 36.4
Mean ± SD 3.3 ± 2.1 1.6 ± 2.1 66.2 ± 58.0 30.4 ± 19.9
N/A: Not available.
* : No specific action potentials were recorded during withdrawing the needle.
the same depth. The action potentials recorded during needle withdrawing were smaller than the action potentials recorded during needle advancing.
The subjects reported increased pain when the needle approached into certain depth. This depth was roughly matched the depth at which the spontaneous electrical activities were recorded. The symptomatic pain reported during withdrawing the needle was also smaller than the pain reported during the needle advancing.
Table 1 shows verbal pain scale and root mean square (RMS) amplitude of EMG epoch at the presumed trigger point area before and after the needing in each subjects.
The verbal pain scale of the subjects was decreased in 5 subjects, unchanged in 2 subjects, and not taken in 1 subject. The mean values of the verbal pain scale decreased significantly (3.3 ± 2.1 to 1.6 ± 2.1, p<0.05) after the penetration of needle through the trigger point.
The EMG amplitude of spontaneous electrical
activity was decreased in 7 subjects and increased
in 1 subject. The mean values of RMS EMG
amplitude decreased (66.2 ± 58.0 µV to 30.4 ± 19.9
µV) after the needling but not significantly (Fig. 2).
Ⅳ. DISCUSSION
Trigger point injection with local anesthetics or sterile saline has been recommended as a therapeutic method of myofascial pain. It has been reported that dry needling without any injection can relieve myofascial pain and is equally effective as trigger point injection.
10)-14)Garvey et al.
10)demonstrated that there was no significant difference between lidocaine injection and dry needling groups on the trigger point of lower back pain patients. Hong
12)demonstrated that both lidocaine injection and dry needling could reduce subjective pain, pressure pain threshold of the trigger point in the trapezius muscle, and range of
motion of cervical spine.
However, the hypotheses that dry needling have efficacy beyond placebo have not been supported.
McMillian et al.
13)investigated the effect of procaine topical application with superficial dry needling (placebo dry needling), dry needling with superficial saline injection (placebo topical application), and superficial saline injection with superficial dry needling (double placebo). All three groups showed significant improvement on the subjective symptoms and did not show any significant differences between groups.
Our results showed that the spontaneous electrical activities from the presumed trigger point were decreased after the needle penetration of the
Fig. 1. Action potentials recorded from the trigger point in one subject at a single depth before (a) and after(b) needling. EMG amplitudes were decreased after penetration of the needle through the trigger point.
(a) (b)
Fig. 2. The effect of dry needling on subjective pain (a) and EMG activity (b) from myofascial trigger point.
The verbal pain scale was significantly decreased after needling. (*: p<0.05, paired t-test)
*
(a)
Before needling After needling
(b)
Before needling After needling
trigger point area in 7 of 8 subjects. In 2 of 7 subjects the specific large action potentials were disappeared after the needle penetration through the trigger point. But, the statistical analyses failed to show significantly decreased RMS EMG amplitude.
It is suspected that minor mechanical disruption of the trigger point such as a single penetration of the needle was not enough to cause inhibitory effect on the activation of the motor structure within the trigger point area.
Hong
12)emphasized the role of local twitch reponses during needle insertion for the inhibitory effect of dry needling on the myofascial trigger point. He reported that rapid needling with elicitation of local twitch responses of trigger point area was significantly effective whereas slow needling without elicitation of local twitch responses showed little change in subjective pain.
Chen et al.
22)recently demonstrated that the spontaneous electrical activity was significantly decreased in the trigger point of rabbit muscles after rapid dry needling with elicitation of local twitch responses. They demonstrated that slow insertion of needle into the trigger point for minimal local twitch response elicitation did not cause any inhibitory effect on the spontaneous electrical activity of trigger point in rabbit muscle. In our study the needle electrode was advanced and withdrawn slowly in few millimeters to find a precise depth of spontaneous electrical activity, so local twitch responses did not elicit during procedure.
The origin of the spontaneous electrical activity from the trigger point is still unknown. Two possible origin are motor endplate and muscle spindle. Simons et al.
16)suggested that the electrical activity of the trigger point is similar to normal endplate potential. They explained that the abnormal electrical activity of trigger point in the resting muscle came from neuromuscular dysfunction at the motor endplate of an extrafusal skeletal muscle. They suggested that spontaneous electrical activity correspond to abnormal end-plate potentials caused by excessive leakage of
acetylcholine. The excessive acetylcholine release depolarize the postjunctional membrane, which may cause significant local increase in Ca
++release, and the increase of Ca
++cause sustained sarcomere shortening and increased metabolism.
1),16)Hubbard et al.
17)hypothesized that the source of electrical activity was sympathetically stimulated intrafusal contraction and it could explain the effects of emotional factors on pain and autonomic symptoms associated with myofascial trigger points. Hubbard
19)demonstrated a single case of biopsy specimen from the trigger point site where the spontaneous electrical activities were recorded.
He reported that the specimen was composed of intrafusal muscle fibers. Donaldson et al.
20)hypothesized that dysregulation of gamma motor neuron of contralateral muscle spindle may develope myofascial trigger point and occur the electrical activity of trigger point.
It is suspected that decrease of the spontaneous electrical activity from the trigger point after the needle penetration may due to the inhibitory effect of mechanical disruption of either muscle spindle stimulation or abnormal acetylcholine release at the motor endplate during needle insertion.
Chen et al.
22)proposed a possibility that the insertion of a needle at the endplate region may lead to greater endplate discharges and thereby reduce immediately available acetylcholine stores.
Reduced acetycholine release may reduce spontaneous electrical activity from the trigger point. In their hypothesis, presence of local twitch response during needle insertion may cause more strong effect on the reduction of excessive acetylcholine.
If the spontaneous electrical activity originates from muscle spindle activation, it is suspected that the insertion of needle into the muscle spindle may occur and cause inhibitory effect on the gamma motor neuron of the intrafusal fiber which can reduce spontaneous electrical activity from myofascial trigger point.
Another possibility is that formation of hematoma
or edema by trauma during needle insertion can
cause inhibitory effect on the activation of motor structure. But there were no visible swelling or ecchymosis on the insertion site of the subjects, and the reduced symptomatic pain after the penetration of the needle does not coincide with this possibility.
The symptomatic pain of the subjects during needle insertion was significantly decreased after the needle penetration. It is suspected that the mechanical disruption of needle penetration through the trigger point was enough to cause an analgesic effect which was mediated by the input into the central nervous system during needle stimulation.
This study provide an evidence that dry needling can reduce subjective pain and spontaneous electrical activity from myofascial trigger point area, but a single penetration was not enough to demonstrate significant effect on the electrical activity. Minor mechanical disruption of the trigger point (single penetration of the needle) did show a decreased subjective pain. Further careful studies with controlled trial and comparing with elicitation of local twitch responses are needed in order to provide more strong evidence about therapeutic effect of dry needling and develope effective treatment of myofascial trigger point.
Ⅴ. CONCLUSIONS
The therapeutic effect of dry needling on myofascial trigger points without any injection of drugs has been reported by many clinical trials. But there was no rigorous evidence that needling therapies have an effect beyond placebo in myofascial trigger point pain.
Eight subjects (4 males and 4 females) who have active trigger points in their trapezius muscles have been recruited. Trigger point was located by manual palpation and confirmed by measuring pressure pain thresholds. The verbal pain scale from the subject and an EMG epoch from a monopolar needle electrode at a certain depth at which spontaneous electrical activity was observed during needle advancing (before needling) and
withdrawing (after needling) were recorded.
The verbal pain scale of the subjects was decreased in 5 subjects, unchanged in 2 subjects, and not taken in 1 subject. The mean values of the verbal pain scale were significantly decreased (3.3
± 2.1 to 1.6 ± 2.1, p<0.05) after the penetration of needle through the trigger point. The EMG amplitude of spontaneous electrical activity was decreased in 7 subjects and increased in 1 subject.
The mean values decreased (66.2 ± 58.0 µV to 30.4
± 19.9 µV) after the needling but not significantly.
This study provide an evidence that dry needling can reduce subjective pain and spontaneous electrical activity from myofascial trigger point area, but a single penetration is not enough to demonstrate significant effect on the electrical activity. Minor mechanical disruption of the trigger point (single penetration of the needle) did show a decreased subjective pain.
REFERENCES
1. Simons, D.G., Travell, J.G., and Simons, L.S. : Travell and Simons' Myofascial Pain and Dysfunction: the Trigger Point Manual, 2nd ed., Vol. 1. Upper Half of Body. Baltimore, 1999, Williams and Wilkins.
2. Fricton, J.R. : Myofascial pain syndrome, characteristics and epidemiology. In: Fricton, J.R., Awad, E.A., editors. Myofascial pain and fibromyalgia. Advances in pain research and therapy, Vol. 17. New York, 1990, Raven Press.
3. Fishbain, D.A., Goldberg, M., Meagher, B.R. et al. : Male and female chronic pain patients categorized by DSM-III psychiatric diagnostic criteria. Pain, 26:181-197, 1986.
4. Fricton, J.R., Kroening, R., Haley, D. et al. : Myofascial pain syndrome of the head and neck: A review of clinical characteristics of 164 patients. Oral Surg., 60:615-623, 1985.
5. Sola, A.E., Rodenberger, M.L., and Gettys, B.B. : Incidence of hypersensitive areas in posterior shoulder muscles. Am. J. Phys. Med., 34:585-590, 1955.
6. Baldry, P. : Management of myofascial trigger point pain. Acupunct. Med., 20:2-10, 2002.
7. Hong, C.Z. : Myofascial trigger point injection. Crit.
Rev. Phys. Med. Rehab., 5:203-217, 1993.
8. Cummings, T.M. and White, A.R. : Needling therapies in the management of myofascial trigger point pain:
a systematic review. Arch. Phys. Med. Rehabil., 82:986-92, 2001.
9. Han, S.C., and Harrison, P. : Myofascial pain syndrome and trigger-point management. Reg.
Anesth., 22:89-101, 1997.
10. Garvey, T.A., Marks, M.R., and Wiesel, S.W. : A prospective, randomized, double-blind evaluation of trigger-point injection therapy for low-back pain.
Spine, 14:962-964, 1989.
11. Hesse, J., Mogelvang, B., and Simonsen, H. : Acupuncture versus metoprolol in migraine prophylaxis: a randomized trial of trigger point inactivation. J. Intern. Med., 235:451-456, 1994.
12. Hong, C.Z. : Lidocaine injection versus dry needling to myofascial trigger point. The importance of the local twitch response. Am. J. Phy. Med. Rehabil.
73:256-263, 1994.
13. McMillan, A.S., Nolan, A., and Kelly, P.J. : The efficacy of dry needling and procaine in the treatment of myofascial pain in the jaw muscles. J. Orofac.
Pain, 11:307-314, 1997.
14. Chu, J. : Does EMG (dry needling) reduce myofascial pain symptoms due to cervical nerve root irritation?
Electromyogr. Clin. Neurophysiol., 37:259-272, 1997.
15. Hong, C.Z. and Simons, D.G.: Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch. Phys. Med. Rehabil., 79:863-872, 1998.
16. Simons, D.G., Hong, C.Z., and Simons, L.S. : Prevalence of spontaneous electrical activity at trigger spots and at control sites in rabbit skeletal muscle. J. Musculoskel. Pain, 3:35-48, 1995.
17. Hubbard, D.R. and Berkoff, G.M. : Myofascial trigger points show spontaneous needle EMG activity. Spine, 18:1803-1807, 1993.
18. McNulty, W.H., Gevirtz, R.N., Hubbard, D.R. et al. : Needle electromyographic evaluation of trigger point response to a psychological stressor. Psychophysiol., 31:313-316, 1994.
19. Hubbard, D.R. : Chronic and recurrent muscle pain:
pathophysiology and treatment, and review of pharmacologic studies. J. Musculoskel. Pain, 4:123-143, 1996.
20. Donaldson, C.C., Nelson, D.V., and Schulz, R. : Disinhibition in the gamma motoneuron circuitry: a neglected mechanism for understanding myofascial pain syndromes? Appl. Psychophysiol. Biofeedback, 23:43-57, 1998.
21. Hong, C.Z. : Pathophysiology of myofascial trigger point. J. Formos. Med. Assoc., 95:93-104, 1996.
22. Chen, J.T., Chung, K.C., Hou, C.R. et al. : Inhibitory effect of dry needling on the spontaneous electrical activity recorded from myofascial trigger spots of rabbit skeletal muscle. Am. J. Phys. Med. Rehabil., 80:729-735, 2001.
Corresponding Author : Jin-Woo Chung, Assistant Professor, Department of Oral Medicine & Diagnosis, College of Dentistry, Kangnung National University, Chibyun-dong 123, Kangnung, Kangwon-do, 210-702, Korea