서 론
최근 들어 의학계에서는 vitamin D에 대한 관심이 커지고 있다.
Vitamin D는 칼슘대사에 중요한 역할을 하는 스테로이드 호르몬으 로, 피부에서 자외선 자극에 의해서 대부분의 vitamin D가 생성되며, 약 20% 정도는 음식을 통해서 섭취하게 된다.1) 그러나, vitamin D 결 핍이 전세계적인 보건문제로 대두되고 있고, vitamin D 결핍은 전세 계 인구의 30%–50%가량이 겪고 있는 매우 흔한 문제이다. 국민건강
영양조사에 따르면 한국 남성 50%–60%, 여성 60%–70%가 심각한 vi- tamin D 결핍을 경험한다고 한다.2,3) Vitamin D 결핍이나 불충분은 골다공증을 유발할 뿐만 아니라, 근육량 및 근육기능을 감소시켜 낙상의 위험을 증가시키고 결과적으로 골다공증에 의한 골절을 유 발한다. 근골격계 이외에 뇌, 전립선, 유방, 면역세포, 혈관의 근육 및 내피세포 등 다양한 조직에서 vitamin D 수용체가 발견되었고, 1,25(OH)D3가 직접 또는 간접적으로 200여 개의 유전자를 조절하여 세포의 증식과 분화, 세포자멸사, 혈관형성 등에 영향을 미치는 것
Received June 5, 2017 Revised September 12, 2017 Accepted September 18, 2017
Corresponding author Kyunam Kim Tel: +82-2-950-1150, Fax: +82-2-950-1153 E-mail: [email protected]
ORCID: http://orcid.org/0000-0003-4168-4616
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.3.435 eISSN 2233-9116
Korean J Fam Pract. 2018;8(3):435-440
Korean Journal of Family Practice
KJFP
한국 성인남성에서 동맥경화지수와 Vitamin D의 관련성
원지혜, 김규남*, 이선영, 김대연, 신혜린, 백정기
인제대학교 의과대학 상계백병원 가정의학교실
The Relationship between Atherosclerosis Index and Vitamin D in Korean Male Adults
Jihye Won, Kyunam Kim*, Seon Yeong Lee, Dae Youn Kim, Hyerin Shin, Jeong Ki Paek Department of Family Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
Background: Recently, interest in vitamin D has been increasing in the medical field. Vitamin D receptors have been found in various tissues such as muscles and endothelial cells of blood vessels, other than the musculoskeletal system. Studies on the relationship between vitamin D level and cardiovascular diseases have been actively conducted. We investigated the correlation between atherogenic index and vitamin D level in healthy Korean men.
Methods: The study included 438 male subjects whose ankle-brachial indexes and serum 25(OH)D levels were measured between January 2016 and December 2016 at the health promotion center of a Sanggye Paik Hospital. They were divided into deficient and sufficient groups according to a cutoff 25(OH)D level of 20 ng/mL. Age, smoking, hypertension, diabetes, and dyslipidemia were considered traditional risk factors of peripheral arterial disease, and ankle-brachial index was used as an atherogenic index.
Results: The ankle-brachial index was statistically significantly different between the two groups (1.11±0.006 vs. 1.14±0.005, P=0.001). Multivariate regression analysis revealed that vitamin D level (β=0.177) and smoking (β=-0.140) were independently associated with ankle-brachial index (P<0.05). We found a statistically significant positive correlation between vitamin D level and ankle-brachial index after adjusting for the traditional risk factors of peripheral arterial disease. However, these correlations were no longer statistically significant after the serum 25(OH)D concentration reached 25 ng/mL.
Conclusion: Primary prevention of peripheral arterial disease requires vitamin D supplementation, but excessive supplementation is unnecessary.
Keywords: Ankle-Brachial Index; Vitamin D; Age; Smoking; Fasting Blood Glucose; Inflammatory Marker
Jihye Won, et al. The Relationship between Atherosclerosis Index and Vitamin D in Korean Male Adults
Korean Journal of Family Practice
KJFP
으로 확인이 되어 vitamin D 대사에 대한 관심이 증가되고 있다.1,4) 25(OH)D는 혈관 내피세포와 단핵구에 발현되어 있는 vitamin D 수 용체에 결합함으로써, 혈관 내피세포의 성장인자의 전사, 합성, 분비 증가에 중요한 역할을 하게 된다. 따라서 vitamin D 결핍은 내피세포 에 영향을 미쳐 혈관확장을 감소시키고, 염증반응과 혈전 형성을 증 가시키며, 혈관의 강직을 증가시킨다.4,5)
말초동맥질환(peripheral artery disease)은 동맥경화에 의해 유발되 는 만성 폐쇄성 동맥 질환이다. 말초동맥질환의 일차적 위험인자는 나이, 흡연, 고혈압, 당뇨, 이상지질혈증 등으로 알려져 있다.6) Vita- min D 결핍이나 불충분이 말초동맥질환의 위험인자인지에 대해 정 립된 바는 없다. 이전 연구에 따르면 vitamin D 결핍이 말초동맥질환 을 포함하는 다양한 심혈관 질환의 높은 유병률과 관계가 있었던 반
면,7-11) 몇몇 연구에서는 관련이 없었다.6,12)
발목-상완지수(ankle-brachial Index, ABI)는 말초동맥질환의 진단 과 동맥경화의 심각한 정도를 평가하는데 널리 이용되고 있다. ABI 가 0.9–1.3 범위를 정상으로 보고 있고, 수치가 낮을수록 다양한 원 인의 심혈관 질환의 사망률을 예측하는데 강력한 독립인자로 이용 된다.
이전 연구에서는 심혈관 질환이 있는 사람에게서 vitamin D와 말 초동맥질환에 연구이거나,13) 서구인을 대상으로 한 연구10,14-16)가 대 부분으로 한국의 건강한 성인에 대한 연구는 부족한 실정이었다. 본 연구에서는 상계백병원 건강검진센터를 방문한 성인 남성에서 동맥 경화의 지표라 할 수 있는 발목 상완 지수와 vitamin D와의 관련성에 대해 알아보고자 한다. 말초동맥질환을 진단받지 않았던 성인에서 말초동맥질환에 독립적으로 영향을 미치는 질환 관련 인자를 확인 하고자 하며, 특히 전통적인 위험인자 외 vitamin D와의 상관관계를 확인하고자 한다. 우리는 vitamin D의 혈중 농도가 높을수록 발목- 상완 지수가 상승할 것이라고 가정하였고, 25(OH)D가 일정 농도 이 상에 도달하면 발목-상완지수(ABI)가 유의한 변화를 보이지 않을 것으로 예상하였다.
방 법
1. 대상
본 연구는 2016년 1월부터 2016년 12월까지 상계백병원 건강검진 센터에 내원하여 동맥경화지수를 대표하는 발목-상완지수(ABI) 및 vitamin D 검사를 시행한 남성 438명을 대상으로 하였다. 신장과 체 중은 신장-체중 자동측정기(Inbody BSM330; Biospace, Seoul, Korea) 를 이용하여 측정하였고, 측정 수치를 토대로 체질량지수(body mass index, BMI)를 계산하였다. 세계보건기구 아시아-태평양 기준(World
Health Organization, Asia-Pacific Perspective, 2000)17)에 따라 체질량지 수 25 kg/m2 이상인 경우를 비만으로 정의하였다. 흡연은 현재 담배 를 피우고 있는 경우 흡연자, 전혀 담배를 피운 적이 없거나 금연 기 간 15년 이상을 비흡연자로 정의하였다. 이외, 혈액검사를 통하여 총 콜레스테롤(total cholesterol, TC), 중성지방(triglycerides, TG), 고밀도 지단백 콜레스테롤(high-density lipoprotein cholesterol, HDL-C), 저밀 도 지단백 콜레스테롤(low-density lipoprotein cholesterol, LDL-C)를 포함한 혈중 지질과 염증 표지자로서 고감도 C-반응단백(high-sensi- tivity C-reactive protein, hs-CRP), 공복혈당(glucose), 당화혈색소 (HbA1c)를 측정하였다. 이 중 LDL-C의 경우 Friedewald 공식에 의한 계산값이 아닌 실측값을 이용하였다. Vitamin D 농도는 화학발광 면 역측정법(chemiluminescent immunoassay) 방법으로 혈중 25(OH)D 를 측정하였다. 현재 혈중 25(OH)D 농도의 참고치 기준이 세계적으 로 통일이 이루어지고 있지 않지만, 대개 25(OH)D 농도가 20 ng/mL 미만인 경우를 결핍, 20–29 ng/mL인 경우를 부족, 30 ng/mL 이상을 정상으로 구분하고 있어 이를 기준으로 하였다.1)
2. 동맥경화지수 측정
동맥경화지수는 발목-상완지수(ABI)를 측정하여 사용하였다. 환 자가 누운 상태에서 약 5분간 안정을 취한 이후 오므론(Omron)사의 VP-1000 자동혈압계(Omron, Kyoto, Japan)를 이용하여 사지 혈압을 측정하였다. 이후 발목 수축기 혈압을 팔 수축기 혈압으로 나누어 오른쪽, 왼쪽 ABI로 나타내었다. 본 논문에서는 양측 ABI 값 중 낮은 값을 택하여 연구를 진행하였다.
3. 통계
통계 분석을 위하여 SPSS version 18 (IBM Co., Armonk, NY, USA) 를 이용하였고, 통계 결과는 평균±표준편차로 표시하였다. 두 군간 연속변수 차이 비교를 위하여 Student’s t-test를 이용하여 분석하였 고, 명목변수의 경우 Chi-square test를 이용하여 분석하였다. 각 생화 학적 표지자와 동맥경화지수의 정규성 검증을 실시하였고, 정규성 분포를 띄지 않는 변수에 대해서는 Spearman’s correlation을, 정규성 을 띄는 변수에 대해서는 Pearson’s correlation을 이용하였다. 동맥경 화지수에 영향을 줄 수 있는 독립인자 확인을 위하여 다변량 선형 회귀분석을 이용하였다. 95%의 유의 수준(P=0.05)에서 통계적 유의 성을 평가하였다.
원지혜 외. 한국 성인남성에서 동맥경화지수와 Vitamin D의 관련성 Korean Journal of Family Practice
KJFP
결 과
1. 연구 대상자의 임상적 특성
총 438명을 대상으로 연구를 진행하였으며, 25(OH)D가 <20 ng/mL 인 그룹이 209명, 25(OH)D ≥20 ng/mL인 그룹이 229명이었다. 평균 연 령은 vitamin D 부족군 47.96세, 정상군은 48.77세로 두 군 간에 통계 적으로 유의한 차이를 보이지 않았다. 혈중 중성지방 및 공복혈당 수치는 두 군간 통계적으로 유의한 차이를 보인 반면, 총 콜레스테 롤, 고밀도 지단백 콜레스테롤, 저밀도 지단백 콜레스테롤, 염증 표 지자 등의 생화학적 지표 및 수축기 혈압, 이완기 혈압, BMI는 두 군 간의 통계적으로 유의한 차이를 보이지 않았다. 발목-상완지수는 vitamin D 부족군 1.11±0.006, 정상군 1.14±0.005로 통계적으로 유의 한 차이를 보였다(Table 1).
2. 각 변수들과 동맥경화지수의 상관관계
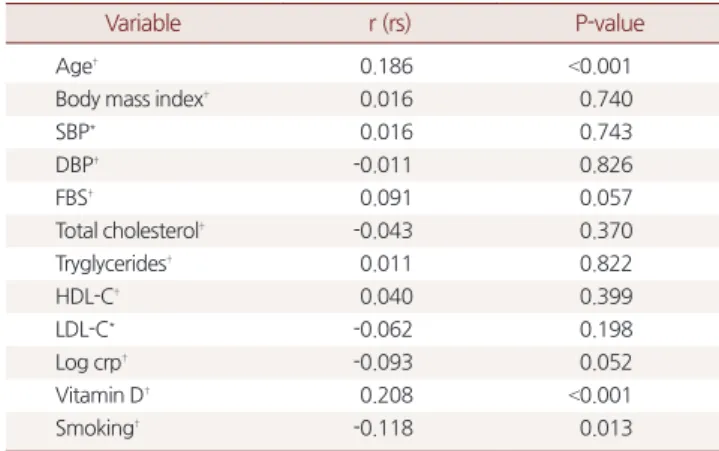
Spearman’s correlation을 이용한 상관분석에서 동맥경화지수는 나이, 25(OH)D 농도와 Spearman 상관계수가 각각 0.186 (P<0.001),
0.208 (P<0.001)로 의미 있는 양의 상관 관계를 보였다. 또한, 공복혈당 과 동맥경화지수 사이에는 Spearman 상관계수가 0.091 (P=0.057)로 통계적으로 유의하지는 않으나 공복혈당이 증가할수록 동맥경화지 수가 증가하는 경향을 보인 반면, 염증 표지자 Log CRP와 동맥경화 지수 사이에는 Spearman 상관계수가 -0.093 (P=0.052)으로 통계적으 로 유의하지는 않으나 염증지수가 높을수록 동맥경화지수는 낮아 지는 경향을 보였다. 그 이외 BMI, 수축기 혈압, 이완기 혈압, 총 콜레 스테롤(TC), 중성지방(TG), 고밀도 지단백 콜레스테롤(HDL-C), 저 밀도 지단백 콜레스테롤(LDL-C) 등의 변수들과 동맥경화지수 사이 에는 통계적으로 유의한 상관 관계를 보이지 않았다(Table 2).
3. 동맥경화지수의 독립적인 영향인자
다변량 선형 회귀분석을 이용하여 동맥경화지수의 독립적인 영 향 인자를 분석하였다. 먼저 각 변수들 간에 상관분석을 실시하여 P<0.1인 변수, 나이, vitamin D level의 계절변이들을 공변수로 설정하 여 다중회귀 분석을 시행하였다. 먼저, 동맥경화지수와 흡연력은 β=-0.140 (P=0.003)으로 통계적으로 유의한 독립적인 영향인자였으 며, 25(OH)D 농도 역시 β=0.177 (P<0.001)로 통계적으로 유의한 독립 적인 영향인자로 확인 되었다(Table 3).
Table 1. Baseline clinical characteristics of study subjects (obesity, BMI
≥25 kg/m2)
Variable Vitamin D <20 (n=209)
Vitamin D ≥20
(n=229) P-value*
Age (y) 47.96±0.72 48.77±0.58 0.373
BMI (kg/m2) 25.14±0.22 25.3±3.2 0.229
Obesity* 101 (48.32) 73 (31.88) <0.001
SBP 119.6±0.86 120.79±0.92 0.348
DBP 78.57±0.75 78.86±0.74 0.789
FBS* (mg/dL) 92.76±1.47 88.93±1.16 0.039
TC 192.72±2.56 194.30±2.03 0.620
TG* 166.20±6.98 122.72±4.41 <0.001
HDL-C 49.04±0.78 49.83±0.77 0.472
LDL-C 119.06±1.85 122.18±1.52 0.189
hs-CRP† (mg/dL) 0.13±0.2 0.12±0.2 0.863
ABI* 1.11±0.006 1.14±0.005 0.001
HTN‡ 60 (28.7) 68 (29.70) 0.821
DM§ 19 (9.10) 14 (6.11) 0.238
Dyslipidemia*,∥ 88 (42.10) 65 (28.38) 0.003
Smoking¶ 62 (29.7) 51 (22.3) 0.081
Values are presented as mean±standard deviation or number (%).
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pres- sure; FBS, fasting blood glucose; TC, total cholesterol; TG, triglycerides; HDL-C, high density lipoprotein-cholesterol; LDL-C, low density lipoprotein-cholesterol;
hs-CRP, high-sensitivity C-reactive protein; ABI, ankle-brachial index; HTN, hyper- tension; DM, diabetes mellitus.
*P <0.05, vitamin D ≤20 versus vitamin D >20. †hs-CRP levels are plotted on a log scale. ‡HTN: SBP ≥140 mmHg or DBP ≥90 mmHg or who taking HTN medica- tion. §DM: HbA1C ≥6.5% or FBS ≥126 mg/dL or who taking DM medication or Insulin therapy. ∥Dyslipidemia: TC ≥240 mg/dL or TG ≥200 mg/dL or LDL-C ≥ 160 mg/dL or who taking dyslipidemia medication. ¶Smoking: current smokers or ex-smokers of no more than 15 years.
Table 2. Pearson’s (spearman) correlation between ABI and variables
Variable r (rs) P-value
Age† 0.186 <0.001
Body mass index† 0.016 0.740
SBP* 0.016 0.743
DBP† -0.011 0.826
FBS† 0.091 0.057
Total cholesterol† -0.043 0.370
Tryglycerides† 0.011 0.822
HDL-C† 0.040 0.399
LDL-C* -0.062 0.198
Log crp† -0.093 0.052
Vitamin D† 0.208 <0.001
Smoking† -0.118 0.013
ABI, ankle-brachial index; SBP, systolic blood pressure; DBP, diastolic blood pres- sure; FBS, fasting blood sugar; HDL-C, high-density lipoprotein cholesterol; LDL- C, low-density lipoprotein cholesterol.
*r: pearson’s correlation coefficient. †rs: spearman’s correlation coefficient.
Table 3. Multiple linear regression analysis between ABI and variables (adjusted by age and season)
Variable β P-value
Vitamin D 0.177 <0.001
Log crp -0.059 0.170
FBS 0.049 0.313
Smoking -0.140 0.003
ABI, ankle-brachial index; FBS, fasting blood sugar.
Jihye Won, et al. The Relationship between Atherosclerosis Index and Vitamin D in Korean Male Adults
Korean Journal of Family Practice
KJFP
4. 하위그룹 분석
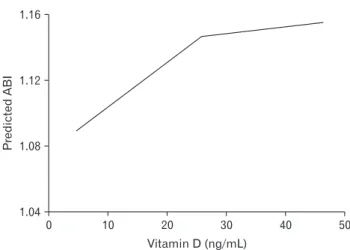
혈청 25(OH)D 농도를 25 ng/mL 기준으로 두 그룹으로 나누어 단 변량 회귀 분석 및 다변량 회귀 분석을 시행하였다. 단변량 선형 회 귀 분석 모델에서(Figure 1) 혈청 25(OH)D가 증가할수록 발목-상완 지수가 통계적으로 유의하게 증가하지만 25(OH)D 농도가 25 mg/
mL 이상에서는 특이적인 상관관계를 보이지 않았다. 또한, 다변량 선형 회귀 모델에서도 혈청 25(OH)D 농도가 25 ng/mL까지는 통계학 적으로 유의한 양의 상관 관계를 보이지만, 25 ng/mL 이상에서는 통 계적으로 유의한 상관 관계를 보이지 않았다(Table 4).
고 찰
본 연구는 한국 성인 남성에서 말초동맥질환 위험 예측을 위한 발 목-상완 지수를 측정함에 있어 측정 결과에 독립적으로 영향을 줄 수 있는 말초동맥질환의 관련인자를 확인하고, 특히 전통적인 위험 인자 외 vitamin D와의 상관관계를 확인하고자 하였다.
본 연구의 결과에 따르면 전통적인 심혈관 질환의 위험인자와 독 립적으로 혈청 vitamin D 수치가 높아질수록 발목-상완 지수가 증가 한다는 결과를 보여주었고, 이는 25(OH)D 농도와 말초동맥질환 사 이의 음의 상관 관계가 있음을 반영한다고 볼 수 있겠다. 하지만, 혈 청 25(OH)D 농도가 25 ng/mL 이상인 경우 vitamin D 농도와 ABI 사 이는 통계적으로 유의한 차이를 보이지 않았다. 이러한 결과는 무증 상의 성인에서 혈청 25(OH)D 농도가 ABI와 비선형적인 관계가 있을 것이라는 우리의 가정과 일치한다고 볼 수 있다.
Vitamin D와 말초동맥질환사이의 상관관계에 대한 국내외 여러
연구 논문이 있다. 먼저 Oh 등18)에 따른 Dong-gu study에서는 혈청 25(OH)D 농도가 증가할수록 말초동맥혈관 질환의 유병률이 통계 적 유의미하게 감소하는 결과를 보여주었다. 국외의 대표적인 연구 결과로는 2001–2004년 미국 국민건강영양조사(National Health and Nutrition Examination Survey) 자료를 이용한 연구가 있다.8,10) Melamed 등8)에 의하면 혈청 25(OH)D 농도가 10 ng/mL 감소할 때마다 말초동 맥질환의 유병률은 1.35 (95% confidence interval, 1.15–1.59)로 증가하 였다. Reis 등10)은 vitamin D 농도와 말초동맥질환 유병률의 인종적인 차이에 대한 연구를 하였다. 흑인이 백인에 비하여 vitamin D 결핍이 통계적으로 유의미하게 낮았고(P<0.001) 말초동맥질환의 유병률이 흑인에게서 더 높게 나타났으며(8.5%, 5.3%, P<0.05) 다른 심혈관계 위 험인자를 보정한 이후에도 여전히 오즈비(odds ratio)가 1.67이었다. 하 지만, 이러한 연구결과에서도 혈청 25(OH)D 농도와 말초동맥질환간 의 비선형적인 관계를 보였는데, Reis 등10)의 연구에는 특히 흑인에서 25(OH)D 사분위수가 증가할수록 낮은 오즈비(odds ratio)를 보였으 며, Melamed 등8)의 연구에서도 4사분위와 비교했을 때, 1사분위 그 룹의 말초동맥질환 유병률은 특이하게 증가한 반면, 2–3사분위 그룹 에서는 그렇지 못하였다.
Vitamin D는 유익한 관점에서 보면 bimodal한 분포를 나타내며,19) 과도한 섭취는 혈관 독성을 보일 수 있다.20) Zittermann 등21)에 의하 면 vitamin D가 결핍되는 것과 마찬가지로 과다한 상태에서도 동맥 경직도 및 석회화가 증가하는 효과인 vitamin D의 혈관 독성 효과 (angiotoxic effect)에 대해 보고하였다.
Vitamin D 결핍이 말초동맥질환 발병 및 합병증을 유발시킨다는 가설을 뒷받침하는 생물학적 설명은 vitamin D 수용체가 혈관내피 세포, 혈관평활근세포 등의 동맥 내의 세포에 발현되어 있어 동맥경 화 합병증과 발병에 영향을 미칠 수 있다는 것이다.22) 또 다른 설명은 vitamin D는 Thrombomodulin 발현을 상향 조절,23) plasminogen acti- vator inhibitor-1 및 mmp-9 단백질 발현을 저해 함으로써 죽상혈전 증을 억제하는 역할을 하기 때문에 vitamin D 결핍이 말초 동맥 질 환과 관련 있다는 것이다.24) 한편, vitamin D가 과다한 경우 parathy- roid hormone이 억제되고, 장내에서 Ca과 PO4 흡수가 증가함으로써
PredictedABI
0 1.16
1.12
1.08
50 Vitamin D (ng/mL)
1.04
40 30
20 10
Figure 1. Relationship between predicted ankle-brachial blood pres- sure index (ABI) and rising serum 25(OH)D concentration from the univariate (single knot at 25 ng/mL; 75th percentile of 25(OH)D) re- gression.
Table 4. Simple linear regression between ABI and 25(OH)D and Mul- tiple linear regression analysis between ABI and variables (adjusted by age and season)
Variable
Linear regression 25(OH)D
<25 ng/mL P-value 25(OH)D
≥25 ng/mL P-value
Univariable (B) 0.003 0.005 0.0004 0.722
Multivariable (β) 0.159 0.003 -0.045 0.711
ABI, ankle-brachial index.
원지혜 외. 한국 성인남성에서 동맥경화지수와 Vitamin D의 관련성 Korean Journal of Family Practice
KJFP
혈관 석회화가 증가되고, 동맥 경직도가 증가할 수 있기 때문에 혈관 독성을 가진다는 설명을 하고 있다.21)
본 연구는 말초동맥질환을 진단받지 않은 무증상의 한국 성인 남 성을 대상으로 연구가 진행되었다. Vitamin D 농도와 말초동맥질환 유병률의 인종적인 차이가 있다는 연구 결과가 있는데, 한국인을 대 상으로 연구를 진행했다는 점에서 의의가 있겠다. 또한, 발목-상완 지수(ABI)라는 객관적인 지표를 사용하여 연구를 진행한 점, 말초 동맥 질환에 영향을 미칠 수 있는 전통적인 위험인자들을 보정한 것 을 강점으로 들 수 있겠다.
반면, 본 연구의 제한점은 첫째로 비교적 적은 수(n=438)를 대상 으로 한 연구라는 점이다. 둘째로 본 연구는 단면연구로 디자인되었 기 때문에 25(OH)D와 말초동맥질환 사이의 시간적인 관계에 대해 서는 알 수 없었다. 셋째로 vitamin D 섭취력, 햇빛 노출 정도 및 운동 에 대한 평가가 이루어지지 않아서 교란 변수로 작용할 수 있다는 점 이 한계로 작용하였다.
결론적으로, 전통적인 심혈관 질환의 위험인자와 독립적으로, 혈 청 25(OH)D 농도가 증가할수록 ABI가 상승하였고, 이는 낮은 혈청 25(OH)D 레벨은 말초동맥질환의 위험도를 높이는 것으로 생각된 다. 하지만 혈청 25(OH)D 농도가 25 ng/mL 이상인 경우 통계학적으 로 유의하지 않은 결과를 보여주었다. 이는 말초동맥질환을 일차적 으로 예방하기 위해서는 혈청 25(OH)D를 과도하게 높이는 것보다 25 ng/mL 정도로 유지하는 것이 더 효율적이라는 것을 보여준다.
Durup 등25)에 의하면 혈중 vitamin D 농도가 20–24 ng/mL을 유지할 때 사망률이 가장 낮은 것을 보고하였고, 사망률 감소 측면에서도 도움이 된다 볼 수 있겠다.
하지만 이러한 vitamin D의 긍정적인 효과가 말초동맥질환의 진 행에 어떠한 영향을 미치는지에 대해서는 알 수 없기 때문에 향후 장기적인 추적검사 및 대규모 연구를 진행하는 것이 필요하다 볼 수 있겠다.
요 약
연구배경:
최근 들어 의학계에서는 vitamin D에 대한 관심이 커지고 있다. Vitamin D의 수용체는 근골격계 이외 혈관의 근육 및 내피세 포 등 다양한 조직에서 발견이 되어 vitamin D와 심혈관 질환 사이의 관계에 대한 연구도 활발하게 이루어지고 있다. 한국의 건강한 성인 남성에게서 동맥경화지수와 vitamin D와의 상관관계를 확인하고자 한다.방법:
2016년 1월부터 2016년 12월까지 상계백병원 건강검진센터에 내원하여 발목-상완지수 및 vitamin D 검사를 시행한 438명의 남성을 대상으로 하였다. 혈청 25(OH)D 수치에 따라 20 ng/mL 미만인 군 을 결핍군, 이상인 군을 충분 군으로 정의하였다. 말초동맥질환에 영 향을 미칠 수 있는 전통적인 위험인자인 나이, 흡연력, 고혈압, 당뇨, 이상지질혈증 등을 고려하였고 동맥경화지수는 발목-상완 지수를 이용하였다.
결과:
발목-상완지수는 vitamin D 결핍군이 1.11±0.006, 충분군이 1.14±0.005로 두 그룹 간 통계적으로 유의한(P=0.001) 차이를 보였다.다중회귀분석에서 vitamin D (β=0.177)와 흡연(β=-0.140)이 ABI와 독 립적인 상관관계를 보였다(P<0.05). 말초동맥질환의 전통적 위험인 자를 보정한 이후에도 vitamin D와 발목-상완지수 사이에는 통계적 으로 유의한 양의 상관관계를 보였다(β=0.177, P<0.001). 하지만 혈청 25(OH)D 농도가 25 ng/mL 도달한 이후에는 이러한 상관관계가 통 계적으로 유의하지 않았다.
결론:
말초동맥질환을 일차적으로 예방하기 위해서는 vitamin D를 보충해 주는 것이 필요하지만, 과도한 보충은 불필요하다.중심단어:
발목-상완지수; 비타민 D; 나이; 흡연; 공복혈당; 염증표 지자REFERENCES
1. Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357: 266-81.
2. Ministry of Health & Welfare. Korea health statistics 2014: Korea national health and nutrition examination survey (KNHANES IV-2). Seoul: Minis- try of Health Welfare; 2015 Dec. 451 p.
3. Joo NS, Dawson-Hughes B, Yeum KJ. 25-Hydroxyvitamin D, calcium in- take, and bone mineral content in adolescents and young adults: analysis of the fourth and fifth Korea national health and nutrition examination survey (KNHANES IV-2, 3, 2008-2009 and V-1, 2010). J Clin Endocrinol Metab 2013; 98: 3627-36.
4. Dessein PH. Vitamin D replacement therapy: a promising adjunct in car- diovascular risk management among patients with rheumatoid arthritis? J Rheumatol 2013; 40: 1463-5.
5. McGreevy C, Williams D. New insights about vitamin D and cardiovascular disease: a narrative review. Ann Intern Med 2011; 155: 820-6.
6. McDermott MM, Liu K, Ferrucci L, Tian L, Guralnik J, Kopp P, et al. Vitamin D status, functional decline, and mortality in peripheral artery disease. Vasc Med 2014; 19: 18-26.
7. Kim DH, Sabour S, Sagar UN, Adams S, Whellan DJ. Prevalence of hypovi- taminosis D in cardiovascular diseases. Am J Cardiol 2008; 102: 1540-4.
8. Melamed ML, Muntner P, Michos ED, Uribarri J, Weber C, Sharma J, et al.
Serum 25-hydroxyvitamin D levels and the prevalence of peripheral arterial disease: results from NHANES 2001 to 2004. Arterioscler Thromb Vasc Biol 2008; 28: 1179-85.
9. van de Luijtgaarden KM, Voûte MT, Hoeks SE, Bakker EJ, Chonchol M, Stolker RJ, et al. Vitamin D deficiency may be an independent risk factor for
Jihye Won, et al. The Relationship between Atherosclerosis Index and Vitamin D in Korean Male Adults
Korean Journal of Family Practice
KJFP
arterial disease. Eur J Vasc Endovasc Surg 2012; 44: 301-6.
10. Reis JP, Michos ED, von Mühlen D, Miller ER 3rd. Differences in vitamin D status as a possible contributor to the racial disparity in peripheral arterial disease. Am J Clin Nutr 2008; 88: 1469-77.
11. Amer M, Narotsky DL, Qayyum R. 25-Hydroxyvitamin D and ankle-bra- chial blood pressure index in adults without peripheral artery disease. Clin Transl Sci 2014; 7: 391-5.
12. Veronese N, De Rui M, Bolzetta F, Toffanello ED, Coin A, Zambon S, et al.
Serum 25-hydroxyvitamin D and the incidence of peripheral artery disease in the elderly. J Atheroscler Thromb 2015; 22: 726-34.
13. Nsengiyumva V, Fernando ME, Moxon JV, Krishna SM, Pinchbeck J, Omer SM, et al. The association of circulating 25-hydroxyvitamin D concentra- tion with peripheral arterial disease: a meta-analysis of observational stud- ies. Atherosclerosis 2015; 243: 645-51.
14. Anderson JL, May HT, Horne BD, Bair TL, Hall NL, Carlquist JF, et al. Rela- tion of vitamin D deficiency to cardiovascular risk factors, disease status, and incident events in a general healthcare population. Am J Cardiol 2010;
106: 963-8.
15. Lee JH, O’Keefe JH, Bell D, Hensrud DD, Holick MF. Vitamin D deficiency an important, common, and easily treatable cardiovascular risk factor? J Am Coll Cardiol 2008; 52: 1949-56.
16. Wallis DE, Penckofer S, Sizemore GW. The “sunshine deficit” and cardiovas- cular disease. Circulation 2008; 118: 1476-85.
17. World Health Organization. Prevention and management of osteoporosis:
report of a WHO scientific group. Report of a WHO Scientific Group, Ge- neva, 2000. WHO Technical report series 921. Geneva: World Health Orga-
nization; 2003. p 92-3.
18. Oh SH, Kweon SS, Choi JS, Rhee JA, Lee YH, Nam HS, et al. Association be- tween vitamin D status and risk of peripheral arterial disease: the Dong-gu study. Chonnam Med J 2016; 52: 212-6.
19. Rajasree S, Rajpal K, Kartha CC, Sarma PS, Kutty VR, Iyer CS, et al. Serum 25-hydroxyvitamin D3 levels are elevated in South Indian patients with ischemic heart disease. Eur J Epidemiol 2001; 17: 567-71.
20. Toda T, Toda Y, Kummerow FA. Coronary arterial lesions in piglets from sows fed moderate excesses of vitamin D. Tohoku J Exp Med 1985; 145:
303-10.
21. Zittermann A, Schleithoff SS, Koerfer R. Vitamin D and vascular calcifica- tion. Curr Opin Lipidol 2007; 18: 41-6.
22. Kassi E, Adamopoulos C, Basdra EK, Papavassiliou AG. Role of vitamin D in atherosclerosis. Circulation 2013; 128: 2517-31.
23. Ohsawa M, Koyama T, Yamamoto K, Hirosawa S, Kamei S, Kamiyama R.
1alpha,25-dihydroxyvitamin D(3) and its potent synthetic analogs down- regulate tissue factor and upregulate thrombomodulin expression in mono- cytic cells, counteracting the effects of tumor necrosis factor and oxidized LDL. Circulation 2000; 102: 2867-72.
24. Artaza JN, Mehrotra R, Norris KC. Vitamin D and the cardiovascular sys- tem. Clin J Am Soc Nephrol 2009; 4: 1515-22.
25. Durup D, Jørgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B. A reverse J-shaped association of all-cause mortality with serum 25-hy- droxyvitamin D in general practice. J Clin Endocrinol Metab 2012; 97:
2644-52.