폐경기 골감소증 여성에서 호르몬 요법과 랄록시펜이 골밀도와 지질 대사에 미치는 영향
고신대학교 의과대학 가정의학교실, 경희대학교 의학전문대학원 경희의료원 산부인과학교실1, 대구보건대학2,
건국대학교 의학전문대학원 산부인과학교실3, 을지대학교 의과대학 을지대학병원 영상의학센터4,
조선대학교 의과대학 산부인과학교실5, 고신대학교 의과대학 산부인과학교실6
김준석․정민형1․김지열2․이태화6․이지영3․양승오4․정 혁5․김흥열6
A Comparison of the Effects of Raloxifene and Hormon Therapy on Lipid Profile and Bone Mineral Density in Postmenopausal Osteopenia Women
Jun Seok Kim, Min Hyung Jung1, Ji Yeol Kim2, Tae Hwa Lee6, Ji Young Lee3, Seoung-Oh Yang4, Hyeok Jung5, Heung Yeol Kim6
Department of Family Medicine, College of Medicine, Kosin University, Busan,
Department of Obstetrics and Gynecology, Kyung Hee Medical Center, School of Medicine, Kyung Hee University1, Seoul, Daegu Health College2, Department of Obstetrics and Gynecology, School of Medicine, Konkuk University3, Seoul,
Department of Radiology, Eulji University Hospital4, Daejeon,
Department of Obstetrics & Gynecology, College of Medicine, Chosun University5, Gwangju, Department of Obstetrics & Gynecology, College of Medicine, Kosin University6, Busan, Korea
Objectives: To compare the raloxifene lipid profile and bone mineral density to estrogen therapy in postmenopausal women with osteopenia.
Methods: In this prospective clinical trial, a total of 132 natural or surgical menopausal women at the Department of Obstetrics and Gynecology of Kosin University Hospital between June 2007 and December 2008 were studied. The effects of raloxifene (Evista® 60mg/day, N=42) and estrogen therapy (PremarinⓇ 0.625mg/day, N=84) were compared in terms of the lipid profile (total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride) changes in bone mineral density over 24 months. The lipid profile and bone mineral density measurements were performed at baseline, and at 12 and 24months.
Results: Women treated with raloxifene for 24 months had a decrease in the total cholesterol and triglyceride levels by 4.8% and 5.5%, and increase in the LDL-C and HDL-C levels by 1.7% and 7.1%, respectively these differences were not statistically significant. Women treated with estrogen for 24 months had a decrease in the total cholesterol level by 1.1%, an increase in the triglyceride level, LDL-C and HDL-C levels by 2.5%, 6.1%, and 5.3%, respectively these differences were not statistically significant. Women treated with estrogen for 24 months had a decrease in the bone mineral density of the lumbar spine by 2.7% and increase in the bone mineral density of the femur neck by 0.7%, respectively these differences were not statistically significant. There was no statistically significant difference in total cholesterol, LDL-C and HDL-C, triglyceride, and bone mineral density between the raloxifene and estrogen therapy groups.
Conclusion: There was no statistically significant difference in the effects of raloxifene and estrogen on the lipid profile and bone mineral density in postmenopausal women after 24 months. Further studies are necessary to establish a definitive comparison of the effects of raloxifene and estrogen therapy on the lipid profile and bone mineral density of postmenopausal women.
Key Words: Menopause, Raloxifene, Estrogen, Lipid profile, Bone mineral density
논문접수일: 2009년 10월 25일, 심사일: 2009년 11월 5일, 게재확정일: 2009년 11월 25일 책임저자: 김흥열, 부산광역시 서구 암남동 34번지 고신대학교 복음병원 산부인과학교실
Tel: 051)990-6226, Fax: 051)990-3300, E-mail: [email protected]
노인 인구가 증가하고 여성에 있어서 건강에 대한 관심도가 증가함에 따라 적절한 호르몬 요법이 임상 적으로 중요한 연구 분야가 되었다. 폐경 여성은 폐 경 초기 열성 홍조와 야간 발한 등 혈관 운동성 증상 뿐만 아니라 골다공증이나 심혈관 질환 같은 만성 질환이 발생할 위험성이 높으며 일반적으로 호르몬 요법이 폐경 증상을 완화시키고 골다공증이나 심혈 관 질환을 줄이기 위해 사용되어 왔다. 그러나 호르 몬 요법을 장기간 사용하였을 경우 유방암이나 자궁 내막암의 위험성을 증가시키며1,2 최근 여러 연구를 통해서는 호르몬 요법이 심혈관 질환을 예방하지 못 한다고 하였다3-6. 하지만 에스트로겐 요법을 이용한 연구에서는 유방암과 심혈관 질환의 위험성은 증가 하지 않았다7. 호르몬 요법은 폐경 증상의 완화에 효 과적이며 골밀도의 증가와 골절을 감소시키는 효과 가 있지만 장기간 사용할 경우 유방암 발생 위험도 가 증가되므로 호르몬 요법의 이점을 유지하면서 호 르몬 요법의 해로운 점이 없는 약제를 연구하게 되 었는데 이러한 약제 중 현재 임상에 이용되고 있는 것이 SERM (Selective Estrogen Receptor Modulator)이 다6,8.
랄록시펜 (Raloxifene hydrocholoride; Evista®; Eli Lilly and Company)은 선택적 에스트로겐 수용체 조 절제로서 골격계와 심혈관계에는 에스트로겐 작용 제로서, 자궁과 유방에는 에스트로겐 길항제로서 작 용한다9,10. 랄록시펜에 대한 가장 대표적인 임상시험 은 1999년 보고된 MORE (In the Multiple Out-comes of Raloxifene Evaluation) 연구로서 골다공증이 있는 폐경 여성 7,705명을 대상으로 3년간 랄록시펜을 투 여한 시험이다. 이 시험에서 랄록시펜 투여군은 대 조군에 비해 요추 골밀도와 대퇴골 골밀도의 유의한 증가를 보일 뿐 아니라 새로운 척추 골절의 발생률 도 기존 골절이 있었던 군에서 30%, 없었던 군에서 50% 감소하였다고 보고하였다11. 랄록시펜은 혈중 총 콜레스테롤과 저밀도 지단백 위험성이 있는 여성 에서 심혈관 질환의 위험성을 감소시킨다고 보고하
였다3,11-13. 또한 랄록시펜은 자궁이나 유방에는 에스
트로겐의 길항제로 작용하여 자궁내막증식이나 자 궁출혈을 증가시키지 않으며 유방암의 발생률도 감 소시킨다고 보고하고 있다10,14-16.
에스트로겐과 랄록시펜이 지질 대사와 골밀도에 미치는 영향은 이미 여러 나라에서 대규모 전향적 연구가 이루어져 있는 상태이지만 에스트로겐과 랄 록시펜의 효과를 비교한 연구는 일부에 지나지 않으
며11,17,18 한국 폐경 여성을 대상으로 한 에스트로겐과
랄록시펜에 대한 비교 연구가 희소하여 이에 저자는 한국 폐경 여성을 대상으로 랄록시펜과 에스트로겐 을 24개월 동안 투여하였을 때 지질 대사와 골밀도 변화에 미치는 영향을 비교하여 알아보기 위하여 본 연구를 시행하게 되었다.
대상 및 방법
1. 연구대상
본 연구는 전향적 연구로서 2007년 6월부터 2008 년 12월까지 고신대학교 복음병원을 방문한 폐경 여 성 중 선정된 132명을 대상으로 하였다. 랄록시펜 투 여군은 42명으로 적어도 1년 이상의 무월경이 있거 나, 자궁의 양성 질환으로 전자궁적출술을 시행 받 았던 여성들 중에서 혈중 FSH (Follicular Stimulating Hormone) 농도가 40 mIU/ml 이상이면서 초기 폐경 증상이 경하거나 없는 여성을 대상으로 하였으며, 에스트로겐 요법군은 84명으로 자궁의 양성 질환으 로 전자궁적출술을 시행 받았던 여성들 중에서 혈중 FSH 농도가 40 mIU/ml 이상이면서 안면 홍조 등 초 기 폐경 증상을 호소하는 여성을 대상으로 하였다.
최근 6개월 이내에 호르몬제를 투여한 과거력이 있 거나 동반된 내분비 질환이나 대사성 질환이 있는 경우는 연구대상에서 제외하였고 최근 6개월간 지질 대사에 영향을 미치는 것으로 알려진 약물을 비롯한 골생성과 골흡수에 영향을 미친다고 생각되는 약제 복용의 과거력이 없는 환자를 대상으로 하였다.
2. 연구 방법
약물의 투여는 랄록시펜 투여군 (N=42)에서는 매 일 Evista® 60 mg을 투여하였고, 에스트로겐 요법군 (N=84)에서는 매일 Progynova® 2 mg을 투여하였다.
약물 투여 전 골밀도 및 공복 시 혈중 총 콜레스테 롤, 중성 지방, 고밀도 지단백 콜레스테롤, 저밀도 지 단백 콜레스테롤을 측정하였으며 이후 매 1년마다
Raloxifene user
Estrogen
user P value No.
Age (yrs) Parity
Menopause age (yrs) Menopause type Natural Surgical Height (cm) Weight (kg) BMI (kg/m²)
42 62.5±11.5
3.2±2.8 47.4±7.1
28 (66.7%) 14 (33.3%) 156.2±6.9 57.6±10.4
24.6±4.7
84 56.1±7.3
3.6±2.4 50.1±5.2
72 (85.7%) 12 (14.3%) 156.3±6.7 59.7±9.6 25.4±4.7
NS NS NS
NS NS NS Valuse are espressed as mean±SD; Statistical analysis:
Student's t-test; BMI=weight(kg)/height(m)2 Table 1. Baseline characteristics of the subjects 총 2년간 위 검사를 시행하였다. 혈중 총 콜레스테
롤, 중성 지방, 고밀도 지단백 콜레스테롤 및 저밀도 지단백 콜레스테롤은 Hitachi 747 자동 분석기를 이 용한 효소법으로 측정하였으며 골밀도 측정은 대퇴 골 경부와 제1~4요추의 골밀도를 Lunar사 (lunar PPODIGY with SmartFAN, #1000, Medison, Wis- consin, USA)의 이중 에너지 X-ray 흡수 계측법 (DXA, 오차율: ±1% 이내)을 이용하여 동시에 측정 하였다. 골밀도의 비교를 위한 단위로는 T-score를 이용하였다.
3. 통계분석
자료의 분석은 SPSS 10.0 for windows 프로그램을 이용하였으며, Paired sample에 대한 Wilcoxon signed rank 검정을 사용하여 약물 투여 이전에 실시한 기저 치에 대한 변화를 분석하였으며 그룹 간의 통계분석 은 Mann-Whitney U 검정을 사용하였다.
치료 후 지질 대사 및 골밀도 변화는 기저치에 대 한 비로 계산하였으며, 각 군의 변화치는 중앙값 [최 소값, 최대값] (median [min, max])으로 표시하였다.
결 과
약물 투여 전 랄록시펜 투여군과 에스트로겐 요법 군의 임상적 특성은 Table 1과 같으며 연령, 분만력, 폐경 연령, 그리고 체질량 지수 (BMI) 사이에는 유의 한 차이는 없었다. 폐경의 유형은 랄록시펜 투여군 에서는 자연 폐경이 28명 (66.7%), 수술적 폐경이 14 명 (23.3%)이었으며 에스트로겐 요법군에서는 자연 폐경이 72명 (85.7%), 수술적 폐경이 12명 (14.3%)이 었다. 2년간 추적 관찰을 하는 동안 랄록시펜 투여군 에서 5명은 자의로 병원을 방문하지 않아 추적 관찰 소실되었으며 2명은 본인이 원하여 에스트로겐제제 로 변경되었으며 3명은 비스포스포네이트 제제로 변 경되어 2년간 추적 관찰한 환자는 32명(탈락률:
23.5%)이었다. 에스트로겐 요법군에서는 15명의 추 적 관찰 소실이 있었으며 4명이 비스포스포네이트 제제로 변경되어 2년간 추적 관찰한 환자는 65명 (탈 락률: 22.6%)이었다.
1. 지질 대사의 변화
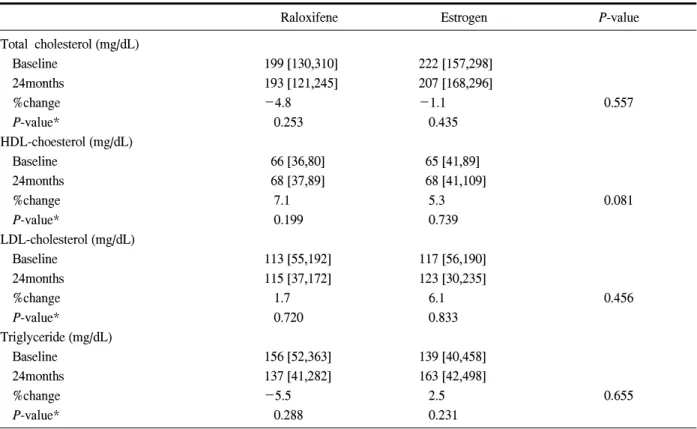
총 콜레스테롤은 랄록시펜 투여군에서는 투여 전 199 [130,310] mg/dL에서 24개월 후 193 [121,245]
mg/dL로 4.8% 감소하였으며 에스트로겐 요법군에서 는 투여 전 222 [157,298] mg/dL에서 24개월 후 217 [168,296] mg/dL으로 1.1% 감소하였으며 두 군 모두 기저치에 대하여 통계적으로 유의한 변화를 보이지 않았다. 또한 각 군 사이에 총 콜레스테롤 농도의 변 화 정도에도 유의한 차이를 보이지 않았다.
고밀도 지단백 콜레스테롤은 랄록시펜 투여군에 서는 투여 전 66 [36,80] mg/dL에서 24개월 후 68 [37,89] mg/dL로 7.1% 증가하였으며 에스트로겐 요법 군에서는 투여 전 65 [41,88] mg/dL에서 24개월 후 68 [41,107] mg/dL로 5.3% 증가하였으며 두 군 모두 기 저치에 대하여 통계적으로 유의한 변화를 보이지 않 았다. 또한 각 군 사이에 고밀도 지단백 콜레스테롤 농도와 변화 정도에는 유의한 차이를 보이지 않았 다.
저밀도 단백질 콜레스테롤은 랄록시펜 투여군에 서는 투여 전 103 [55,192] mg/dL에서 24개월 후 115 [37,172] mg/dL로 1.7% 증가하였으며 에스트로겐 요 법군에서는 투여 전 117 [56,190] mg/dL에서 24개월 후 123 [30,235] mg/dL로 6.1% 증가하였으며 두 군 모 두 기저치에 대하여 통계적으로 유의한 변화를 보이 지 않았다. 또한 각 군 사이에 저밀도 지단백 콜레스
Raloxifene Estrogen P-value Total cholesterol (mg/dL)
Baseline 24months
%change P-value*
HDL-choesterol (mg/dL) Baseline
24months
%change P-value*
LDL-cholesterol (mg/dL) Baseline
24months
%change P-value*
Triglyceride (mg/dL) Baseline
24months
%change P-value*
199 [130,310]
193 [121,245]
-4.8 0.253
66 [36,80]
68 [37,89]
7.1 0.199
113 [55,192]
115 [37,172]
1.7 0.720
156 [52,363]
137 [41,282]
-5.5 0.288
222 [157,298]
207 [168,296]
-1.1 0.435
65 [41,89]
68 [41,109]
5.3 0.739
117 [56,190]
123 [30,235]
6.1 0.833
139 [40,458]
163 [42,498]
2.5 0.231
0.557
0.081
0.456
0.655
* Baseline vs 24 months. Statistical analysis: Wilcoxon signed rank test. Raloxifene group vs estrogen group. Statistical analysis: Mann-Whitney U test.
Table 2. Comparison of lipid profile in postmenopausal women Values expressed as median (min, max)
테롤 농도의 변화 정도에도 유의한 차이를 보이지 않았다.
중성 지방은 랄록시펜 투여군에서는 투여 전 156 [52,363] mg/dL에서 24개월 후 137 [42,282] mg/dL로 5.4% 감소하였으며 에스트로켄 요법군에서는 투여 전 139 [40,458] mg/dL에서 24개월 후 163 [42,498]
mg/dL로 2.5% 증가하였으며 두 군 모두 기저치에 대 하여 통계적으로 유의한 변화를 보이지 않았다. 또 한 각 군 사이에 중성 지방 농도의 변화 정도에도 유 의한 차이를 보이지 않았다 (Table 2).
2. 골밀도의 변화
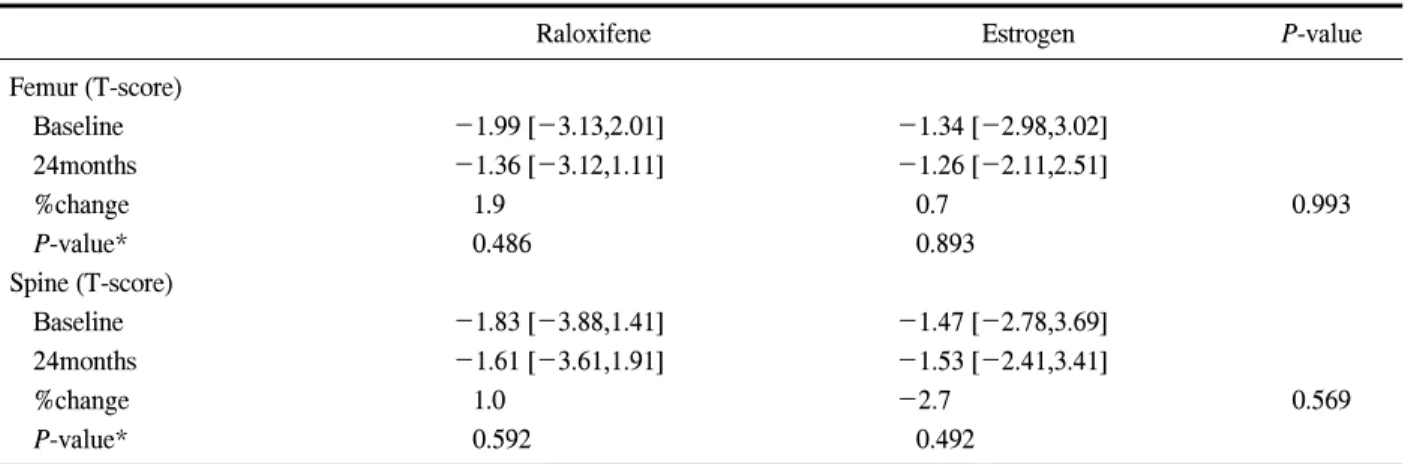
대퇴골 골밀도는 랄록시펜 투여군에서는 투여 전 T-score -1.99 [-3.13,2.01]에서 24개월 후 -1.36 [-3.12,1,11]으로 109% 증가하였으며 에스트로겐 요 법군에서는 투여 전 T-score -1.34 [-2.98,3.02]에서 24개월 후 -1.26 [-2.11,2.51]으로 0.7% 증가하였으 며 두 군 모두 기저치에 대하여 통계적으로 유의한
변화를 보이지 않았다. 또한 각 군 사이에 대퇴골 골 밀도 변화 정도에도 유의한 차이를 보이지 않았다.
척추 골밀도는 랄록시펜 투여군에서는 투여 전 T-score -1.83 [-3.88,1.41]에서 24개월 후 -1.61 [-3.61,1.91]으로 1.0% 증가하였으며 에스트로겐 요 법군에서는 투여 전 -0.47 [-2.78,3.69]에서 24개월 후 -0.53 [-2.41,3.41]으로 2.7% 감소하였으며 두 군 모두 기저치에 대하여 통계적으로 유의한 변화를 보 이지 않았다. 또한 각 군 사이에 척추 골밀도 변화 정도에도 유의한 차이를 보이지 않았다(Table 3).
고 찰
에스트로겐은 동맥경화증의 주된 원인이 되는 저 밀도 지단백 콜레스테롤의 혈중 농도를 감소시키고 고밀도 지단백 콜레스테롤을 증가시켜 심혈관 질환 의 위험을 감소시키지만, 반면에 중성 지방은 증가
시킨다8,19,20. 폐경 여성을 대상으로 한 여러 연구에서
Raloxifene Estrogen P-value Femur (T-score)
Baseline 24months
%change P-value*
Spine (T-score) Baseline 24months
%change P-value*
-1.99 [-3.13,2.01]
-1.36 [-3.12,1.11]
1.9 0.486
-1.83 [-3.88,1.41]
-1.61 [-3.61,1.91]
1.0 0.592
-1.34 [-2.98,3.02]
-1.26 [-2.11,2.51]
0.7 0.893
-1.47 [-2.78,3.69]
-1.53 [-2.41,3.41]
-2.7 0.492
0.993
0.569
Values expressed as median [min, max]. *Baseline vs 24months. Statistical analysis: Wilcoxon signed rank test. Raloxifene group vs estrogen group. Statistical analysis: Mann-Whitney U test.
Table 3. Comparison of Bone Mineral density in postmenopausal women
에스트로겐을 투여하였을 때 1년 후 고밀도 지단백 콜레스테롤은 12~27% 증가하였고21 중성 지방은 5~17% 증가하였는데, 이러한 경구 에스트로겐에 의 한 중성 지방의 증가는 매우 중요한 의미를 가지며 심혈관계에 나쁜 영향을 미칠 수 있다22. 본 연구에 서는 에스트로겐 요법군에서 총 콜레스테롤은 1.1%
감소, 고밀도 지단백 콜레스테롤은 5.3% 증가, 중성 지방은 2.5% 증가하였으나 통계적인 유의성은 없었 으며 저밀도 지단백 콜레스테롤은 기존 연구와 달리 6.1% 증가하였다. 랄록시펜은 심혈관계에 에스트로 겐 작용제로서 작용하여 총콜레스테롤과 저밀도 지 단백 콜레스테롤을 감소시킨다고 보고되었다. 하지 만 에스트로겐이 고밀도 지단백 콜레스테롤과 중성 지방을 증가시키는 것과는 달리 랄록시펜은 이들에 유의한 변화를 보이지 않는다고 하였다23. 폐경 여성 을 대상으로 랄록시펜을 투여한 연구에서 총 콜레스 테롤은 7.0%, 저밀도 지단백 콜레스테롤은 13.2% 감 소하여 대조군에 비해 유의한 변화를 보였으나24 고 밀도 지단백 콜레스테롤은 대조군에 비해 유의한 변 화를 보이지 않았다고 보고 하였다25. 본 연구에서는 랄록시펜 투여군에서 총 콜레스테롤은 4.8% 감소하 였으나 통계적인 유의성은 없었으며 기존 연구와 달 리 저밀도 지단백 콜레스테롤은 1.7% 증가, 고밀도 지단백 콜레스테롤은 7.1% 증가, 중성 지방은 5.5%
감소하였다.
Reid 등26은 3년간 랄록시펜 투여군, 에스트로겐 요
법군, 위약군을 비교한 바 저밀도 지단백 콜레스테 롤은 랄록시펜 투여군과 에스트로겐 요법군에서 위 약군에 비해 큰 변화가 없었으나 고밀도 지단백 콜 레스테롤은 에스트로겐 요법군에서 13.4%의 증가를 보인 반면 랄록시펜 투여군에서는 변화가 없었다고 하였다. 중성 지방은 에스트로겐 요법군에서는 24.6% 증가를 보인 반면 랄록시펜 투여군에서는 4.9%의 증가를 보여 지질 대사에 있어서 랄록시펜 투여군과 에스트로겐 요법군 사이에 서로 다른 양상 의 변화를 보인다고 보고하였다. Christodoulakos 등27 의 연구에서는 에스트로겐 요법군에서 중성 지방은 23.7%, 고밀도 지단백 콜레스테롤은 7.4% 증가하였 으나 랄록시펜 투여군에서는 중성 지방, 고밀도 지 단백 콜레스테롤은 11.2%, 11.0%의 감소를 보였다고 보고하였다. 본 연구에서는 기존 연구와는 달리 랄 록시펜 투여군과 에스트로겐 요법군 사이에 유의한 차이를 보이지 않았다.
에스트로겐 요법이 골밀도를 증가시킨다는 증거 는 Postmenopausal Estrogen/Progestin Intervention (PEPI) trial을 포함한 많은 연구를 통해 입증된 바 있 으며 이러한 연구에서 에스트로겐 요법군은 대조군 에 비해 척추 골밀도는 3.5~7.0%, 대퇴골 골밀도는 2~4% 증가하였으며 기저치에 비해 대퇴골 골밀도 는 0.6% 증가하였고, 척추 골밀도는 1.6% 감소하였 으나 통계적으로 유의한 차이는 없었다. 랄록시펜이 골밀도에 미치는 영향은 MORE 연구를 비롯한 여러
연구에서 보고되었으며 MORE 연구에서 랄록시펜 60 mg/day을 36개월간 투여하였을 때 골밀도 증가는 대조군에 비해 척추 골밀도 2.6%, 대퇴골 골밀도 2.1%로 보고하였다8. 다른 여러 연구에서도 2~3년 간 랄록시펜을 투여하였을 때 척추 골밀도는 기저치 에 비해 약 1~3%, 대조군에 비해 약 2~3%의 증가 를 보였으며 대퇴골 골밀도는 대조군에 비해 1~2%
의 증가를 보였다고 보고하였다9,25,31. MORE 연구의 대상군을 상대로 연구 기간을 4년 더 연장한 CORE
(Continuing Outcomes Relevant to Evista) 연구 결과 가 최근 보고 되었는데 7년 동안 랄록시펜을 투여한 군에서 척추 골밀도는 기저치에 비해 2.2%, 대조군 에 비해 4.3% 증가하였으며, 대퇴골 골밀도는 기저 치에 비해 1.9%, 대조군에 비해 3.0% 증가하였다고 한다32. 본 연구에서는 랄록시펜 투여군에서 기저치 에 비해 대퇴골 골밀도는 1.9% 척추 골밀도는 1.0%
증가하였으나 통계적으로 유의한 차이는 없었다.
Prestwood 등18은 6개월간 랄록시펜과 에스트로겐 을 투여 후 골밀도 변화를 비교한 연구에서 두군 모 두에서 대퇴골 골밀도와 척추 골밀도가 기저치에 비 해 유의하게 증가하였으며, 척추 골밀도는 에스트로 겐 요법군에서 랄록시펜 투여군보다 유의하게 증가 하였고 대퇴골 골밀도는 랄록시펜 투여군에서 에스 트로겐 요법군보다 유의하게 증가하였다고 보고하 였다.
Reid 등26은 3년간 위약군과 랄록시펜 투여군, 에 스트로겐 요법군을 비교한 결과 위약군에서는 척추 골밀도가 2% 감소한 반면 랄록시펜 투여군에서는 변화가 없었으며 에스트로겐 요법군에서는 4.6%의 증가를 보여 척추 골밀도가 에스트로겐 요법군에서 위약군이나 랄록시펜 투여군에 비해 유의하게 증가 하였다고 보고하였다. 본 연구에서는 랄록시펜 투여 군과 에스트로겐 요법군에서 대퇴골 골밀도 및 척추 골밀도 변화가 기존 연구와는 달리 유의한 차이를 보이지 않았다.
결 론
본 연구에서 랄록시펜 투여군과 에스트로겐 요법 군에서 각각 기저치에 비해 지질 대사와 골밀도에
있어 유의한 변화를 보이지 않았으며 또한 두 군 간 의 유의한 차이를 보이지 않았다. 이는 대조군이 없 다는 점과 한국 폐경 여성을 대상으로 하였다는 점, 그리고 대상수가 적고 환자의 투약 순응도에 대한 평가가 없었다는 점 등을 그 원인으로 유추할 수 있 으며 향후 한국 폐경 여성을 대상으로 두 약제의 지 질 대사와 골밀도 변화에 미치는 영향을 확인할 수 있는 다기관 전향적 연구가 시행되어야 할 것으로 생각된다.
참 고 문 헌
1. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52705 women with bhreast cancer and 108411 women without breast cancer. Lancet 1997;350:1047-59.
2. Beresford SA, Weiss NS, Voigt LF, Mcknight BS.
Risk of endometrial in relation to use of oestrogen combined with cyclic progestagen therapy in post- menopausal women. Lancet 1997;349:458-61.
3. Grady D, Wenger NK, Herrington D, Khan S, Furberg C, Hunnmghake D, et al. Postmenopausal hormone therapy increases risk for venous throm- boembolic disease: the Heart and Estrogen/
progestin Replacement Study. Ann Intern Med 2000;132:689-96.
4. Manson JE, Hsia J, Johnson KC, Rossouw JE, Assaf AR, Lasser NL, et al. Estrogen plus proges- tin and the risk of coronary heart disease. N Engl J Med 2.3;349:523-34.
5. Rossouw JE, Anderson GL, Prentice RL, LaCroixAZ, Kooperverg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321-33.
6. Wassertheil-Smoller S, Hemdrix SL, Limacher M, Heiss G, Kooperberg C, Mysiw WJ. Effect of
estrogen plus progestin on stoke in postmenopausal women: the Women's Health Initiative: a randomi- zed trial. JAMA 2003;289:2673-84.
7. Writing group for the women's health initiative investigators. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA 2004;291:1707-12.
8. Effects of estrogen or estrogen/progestin regimens on heart disese risk factors in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions(PEPI) Trial. The Writing Group for the PEPI Trial. JAMA 1995;273:199-208.
9. Delmas PD, Bjarnason NH, Milak BH, Ravoux AC, Shah AS, Huster WJ, et al. Effects of raloxifene on bone mineral density, serum cholesterol concent- rations, and uterine endometrium in postmenopausal women. N Engl J Med 1997;337:1641-7.
10. Cummings S Eckert S, Krueger KA, Grady D, Powles TJ, Cauley JA, et al. The effect of raloxifene on risk if breast cancer in postmeno- pausal women. JAMA 1999;281:2189-97.
11. Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen T, Genant HK, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. JAMA 1999;282:637-45.
12. Walsh BW. Kuller LH, Wild RA, Paul S, Farmer M, Lawrence JB, et al. Effects of raloxifene on serum lipids and coagulation factors in healthy postmenopausal women. JAMA 1998;279:1445-51.
13. Barret-Connor E, Grady D, Sashegyi A, Anderson PW, Cox DA, Hoszowski K, et al. Ralozifene and cardiovascular events in osteoporotic postmeno- pausal women: 4-year results from the MORE (Multiple Outcomes of Raloxifene Evaluation) randomized trial. JAMA 2002;287:847-57.
14. Cauley JA. Norton L, Lippaman ME, Eckert S, Krueger KA, Purdie DW, et al. Continued breast
cancer risk reduction in postmenopausal women treated with raloxifene: 4-year results from the MORE trial. Breast Cancer Res Treat 2001;65:
125-34.
15. Boss SM, Huster WJ, Neild JA, Glant MA, Eisenhut CC, Draper MW. Effects of raloxifene hydrochloride on the endometrium of postmeno- pausal women. Am J Obstet Gynecol 1997;177:
1458-64.
16. Davies GC. Huster WJ, Shen W, Mitlak B, Plouffe L, Shan A, et al. Endometrial response to raloxifene compared with placebo, cyclical hormone replace- ment therapy, and unopposed estrogen in postmeno- pausal women. Menopause 1996;6:188-95.
17. Delmas PD, Bjarnason NH, Mitlak BH, Ravoux AC, Shah AS, Huster WJ, et al. The effects of raloxifene on bone mineral density serum cho- lesterol, and uterine endometrium. N Engl J Med 1997;337:1641-7.
18. Prestwood KD, Gunness M, Muchmore DB, Lu Y, Wong M, Raisz LG. A comparison of the effects of raloxifene and estrogen on bone in postmenopausal women. J Clin Endocrinol Metab 2000;85:2197- 202.
19. Wish BW, Schiff I, Rosner B, Greenverg L, Ravnikar V, Sacks FM. Effects of postmenopausal estrogen replacement on the concentrations and metabolism of lipoprotein. N Engl J Med 1991;
325:1196-204.
20. Wild RA. Estrogens: effects on the cardiovascular tree. Obstet Gynecol 1996; 87 Suppl 2:27S-35S.
21. Sherwin BB. Gelfand MM. A prospective one-year study of estrogen and progestin in postmenopausal women: effects on clinical symptoms and lipoprtein lipids. Obstet Gynecol 1989;73(5 Pt 1):759-66.
22. Farish E, Barnes JE, Fletcher CD, Ekevall K, Caler A, Hark DM. Effects of tibolone on serum lipotrotein and apolipoprotein levels compared with a cyclical estrogen/pregestogen regimen. Meno- pause 1999;6:98-104.
23. Walsh BW, Kuller LM, Wild RA, Paul S, Farmer M, Lawrence JB, et al. Effects of raloxifene on serum lipids and coagulation factors in healthy postmenopausal women. JAMA 1998;279:1445-51.
24. Lufkin EG, Whitaker MD, Nickelsen T, Argueta R, Caplan RH, Knickerbocker RK, et al. Treatment of established postmenopausal osteoporosis with raloxifene: a randomized trial. J Bone Miner Res 1998;13:1747-54.
25. Meunier PJ, Vignot E, Garnero P, Confavreux E, Paris E, Liu-Leage S, et al. Treatment of postmeno- pausal women with osteoporosis or low bone density with raloxifene. Osteoporos Int 1999;10:
330-6.
26. Reid IR, Eastell R, Fogelman I, Adachi JD, Rosen A, Netelenbos C, et al. A comparison of the effects of raloxifene and conjugated equine estrogen on bone and lipids in healthy postmenopausal women.
Arch Intern Med 2004;164:871-9.
27. Christodoulakos GE, Lambrinoudaki V, Panoulis P, Papadias A, Kouskouni E, Creatsas GC. Effect of hormone replacement therapy, tibolone and raloxi- fene on serum lipids, apolipoprotein A1, apolipo- protein B and lipoprotein (a) in Greek postmeno- pausal women. Gyneco Endocrino 2004;18:244-57.
28. The Writing Group for the PEPI trial, Effects of hormone therapy on bone mineral density: results from the postmenopausal Estrogen/Progestin Inter- ventions (PEPI) Trial. JAMA 1996;276:1389-96.
29. Lindsay R, Gallagher JC, Kleerekoper M, Pickar JH. Effect of lower doses of conjugated equine estrogens with and without medorxyprogesterone accate on bone in early postmenopausal women.
JAMA 2002;287:2668-76.
30. Bone HG, Greenspan SL, Mckeever C, Bell N, Davidoson M, Downs RW, et al. Alendronate and estrogen effects in postmenopausal women with low bone mineral density. J Clin Endocliol Metab 2000;85:720-6.
31. Lufkin EG, Whitaker MD, Nickelsen T, Argueta R, Caplan RH, Knickerbocker RK, et al. Treatment of established postmenopausal osteoporosis with ralo- xifene: a randomized trial. J Bone Miner Res 1998;13:1747-54.
32. Ethel ss, Steve TH, Richard E, Jose RZ, Stefan G, Adolfo DP, et al. Skeletal effects of raloxifene after 8 year: Results from the Continuing Outcomes Relevant to Evista (CORE) study. J Bone Miner Res 2005;20:1514-24.
■ 국문초록 ■
목적: 한국 폐경 여성을 대상으로 한 에스트로겐과 랄록시펜에 대한 비교 연구가 희소하여 이에 저 자는 한국 폐경 여성을 대상으로 랄록시펜과 에스트로겐을 24개월 동안 투여하였을 때 지질 대사와 골 밀도 변화에 미치는 영향을 비교하여 알아보기 위하여 본 연구를 시행하게 되었다.
방법: 약물의 투여는 랄록시펜 투여군 (N=42)에서는 매일 EvistaⓇ 60 mg을 투여하였고, 에스트로겐 요법군 (N=84)에서는 매일 ProgynivaⓇ 2 mg을 투여하였다. 약물 투여 전 골밀도 및 공복 시 혈중 총 콜 레스테롤, 중성 지방, 고밀도 지단백 콜레스테롤, 저밀도 지단백 콜레스테롤을 측정하였으며 이후 매 1 년마다 총 2년간 위 검사를 시행하였다.
결과: 총 콜레스테롤은 랄록시펜 투여군에서는 4.8% 감소하였으며 에스트로겐 요법군에서는 1.1%
감소하였고 고밀도 지단백 콜레스테롤은 랄록시펜 투여군에서는 7.1% 증가하였으며 에스트로겐 요법 군에서는 5.3% 증가하였고 저밀도 단백질 콜레스테롤은 랄록시펜 투여군에서는 1.7% 증가하였으며 에 스트로겐 요법군에서는 6.1% 증가하였고 중성 지방은 랄록시펜 투여군에서는 5.4% 감소하였고 에스트 로켄 요법군에서는 2.5% 증가하였고 대퇴골 골밀도는 랄록시펜 투여군에서는 109% 증가하였으며 에스 트로겐 요법군에서는 0.7% 증가하였고 척추 골밀도는 랄록시펜 투여군에서는 1.0% 증가하였으며 에스 트로겐 요법군에서는 2.7% 감소하였다.
결론: 본 연구에서 랄록시펜 투여군과 에스트로겐 요법군에서 각각 기저치에 비해 지질 대사와 골밀 도에 있어 유의한 변화를 보이지 않았으며 또한 두 군 간의 유의한 차이를 보이지 않았다. 이는 대조군 이 없다는 점과 한국 폐경 여성을 대상으로 하였다는 점, 그리고 대상수가 적고 환자의 투약 순응도에 대한 평가가 없었다는 점 등을 그 원인으로 유추할 수 있으며 향후 한국 폐경 여성을 대상으로 두 약제 의 지질 대사와 골밀도 변화에 미치는 영향을 확인할 수 있는 다기관 전향적 연구가 시행되어야 할 것 으로 생각된다.
중심단어: 폐경기, 골밀도, 에스트로젠, 랄록시펜, 지질대사