서 론
뇌 자기공명영상(magnetic resonance imaging, MRI)에서 white matter hyperintensity (WMH)는 뇌졸중 및 인지기능장애의 위험요 소로,1) 신경학적인 이상이 없는 일반 노년층에서도 흔히 관찰되는
병변이다.2) WMH는 대뇌 소혈관의 만성적인 허혈로 인한 신경의 탈 수초화 및 축삭(Axon)의 소실로 인해 발생하는 것으로 알려져 있으 며,3) 심뇌혈관질환의 위험 요소인 고혈압,4) 당뇨,5) 흡연6) 등의 요인과 연관성 있다는 연구들이 있다.
한편, 대사증후군은 혈관 내 동맥경화와 지방유리질증(lipohyali-
Received July 6, 2017 Revised September 5, 2017 Accepted September 15, 2017
Corresponding author Jin-Ho Park Tel: +82-2-2072-3335, Fax: +82-2-766-3296 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-3942-6813
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Brief
Communication
https://doi.org/10.21215/kjfp.2018.8.3.477 eISSN 2233-9116
Korean J Fam Pract. 2018;8(3):477-481
Korean Journal of Family Practice
KJFP
신경학적 이상이 없는 성인에서 대사증후군과 White Matter Hyperintensity의 연관성에 대한 분석
강미소
1, 박진호
1,2*, 남기웅
3, 권형민
3,4, 김상혁
1, 정수민
1, 김신혜
1, 유태곤
1, 이지은
11서울대학교병원 가정의학과, 2서울대학교병원 건강검진센터, 3서울대학교병원운영 서울특별시보라매병원 신경과, 4서울대학교 의과대학 신경과
Association of Metabolic Syndrome with White Matter Hyperintensity Volume in Neurologically Healthy Adults
Miso Kang1, Jin-Ho Park1,2,*, Ki-Woong Nam3, Hyung-Min Kwon3,4, Sang Hyuck Kim1, Su-Min Jeong1, Shinhye Kim1, Tae Gon Yoo1, Ji Eun Lee1
1Department of Family Medicine and 2Health Promotion Center, Seoul National University Hospital; 3Department of Neurology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center; 4Department of Neurology, Seoul National University College of Medicine, Seoul, Korea
Background: White matter hyperintensity (WMH), known to be caused by chronic ischemic damage in blood vessels, is a predictor of stroke and cognitive decline. Metabolic syndrome (MS) is a risk factor for blood vascular disorders, such as atherosclerosis. This study aimed to analyze the association of MS with WMH volume in adults without a history of stoke or transient ischemic attack.
Methods: A total of 3,168 subjects who underwent brain magnetic resonance imaging as part of a screening health check-up were enrolled in this study. WMH volume was quantitatively measured, and its square root value was calculated for the normal distribution data prior to analysis. MS was defined as according to the 2009 American Heart Association guidelines. Multivariate linear regression analysis was performed for the association between MS and WMH volume after adjustments for age, sex, body mass index, current smoking status, and anticoagulant or antithrombotic drug intake.
Results: The mean age of the subjects was 56.4±9.5 years, and the mean WMH volume was 2.6±6.3 cm3. A total of 849 subjects (26.8%) met the diagnostic criteria for MS. In multivariate linear regression analysis, MS showed a significant association with WMH volume (β=0.155; P<0.001), and WMH volume tended to increase with an increase in the number of MS components (P<0.001).
Conclusion: MS incidence and its severity, measured by the number of components, were independently associated with WMH volume. Longitudinal studies should be performed in future to evaluate their causal relationship and degree of association.
Keywords: Leukoaraiosis; Metabolic Syndrome; Magnetic Resonance Imaging; Cerebrovascular Diseases
Miso Kang, et al. Association of Metabolic Syndrome with White Matter Hyperintensity
Korean Journal of Family Practice
KJFP
nosis)을 진행시켜 뇌졸중 및 심근경색 등 심뇌혈관질환을 유발하는 강력한 위험요소로,7,8) 최근에는 인지기능 저하와의 관련성도 제기
되고 있다.9,10)
심뇌혈관의 허혈성 변화를 유발하는 대사증후군이 WMH 발생 과 연관 있을 것이라는 가능성이 제기되었고, 몇 개의 연구들이 시 행되었다. 기존에 대사증후군과 WMH와의 연관성에 대한 연구는, 대부분 WMH 유무 혹은 정도의 그룹화에 따른 정성적 분석으로, 연관성은 입증되었으나 양의 상관관계 여부 등은 밝혀지지 않았
다.11-15) WMH 부피를 정량적으로 분석한 연구도 있었으나, 정성적 연
구들의 결과와는 달리 대사증후군과 WMH 부피가 연관성이 없다 는 결과가 있었다.16) 이는 다른 연구가 대부분 신경학적 이상이 없는 사람을 대상으로 한 것과 달리, 해당 연구는 동맥질환이 있는 환자 를 대상으로 했다는 점에서 차이가 있을 것으로 생각된다. 이에, 본 연구에서는 뇌졸중 및 일과성 허혈발작의 병력이 없는 사람을 대상 으로 하여 WMH의 정량적 부피와 대사증후군의 연관성을 확인하 고, 양적 상관관계의 여부를 알아보고자 하였다.
방 법
1. 연구 대상
2006년 1월부터 2013년 12월까지 건강검진을 위해 서울대학교병 원에 내원한 수검자 중 뇌 MRI를 촬영한 성인을 대상으로 하였다.
연구 대상자의 생활습관 및 병력을 설문지를 통해 조사하였고, 검사 전 가정의학과 의사가 다시 한번 연구 대상자의 과거 및 현재 병력과 현재 약물 복용력을 면담을 통해 확인하였다. 항고혈압제, 당뇨병 약 제, 지질강하제, 항혈소판제제 복용 여부를 조사하였고, 생활습관 중 흡연은 1) 비흡연군+과거 흡연군, 2) 현재 흡연군으로 분류하였다.
키와 체중은 가벼운 가운만 입고 측정하였고, 복부 둘레는 장골능 과 늑골의 하한선의 중간부위를 줄자로 측정하였다. 혈압은 충분한 휴식 후 자동혈압계로 측정하였다. 검사 전날 저녁부터 12시간 이상 의 금식 후 혈액을 채취해 혈청 자동분석기(Architect c8000; Toshiba Inc., Tokyo, Japan)을 이용하여 측정하였으며, 1.5-Tesla MR (Signa, GE Healthcare, Milwaukee, WI, USA or Magnetom SONATA, Siemens, Munich, Germany)를 이용하여 뇌 MRI를 촬영하였다.
뇌 MRI을 촬영한 22–86세 수검자 3,258명 중 혈액검사 결과가 누 락된 27명, WMH 부피 측정이 누락된 1명, 과거 뇌졸중 및 일과성 허 혈발작(transient ischemic attack)의 병력이 있는 62명을 ‘신경학적 이 상이 있는 대상’으로 제외하고, 최종 3,168명을 대상으로 분석하였 다.
본 연구는 서울대학교병원 임상연구윤리위원회(Institutional Re-
view Board)의 승인을 받아 시행되었다(IRB no. H-1604-072-754).
2. WMH 부피 측정
1.5-Tesla MR을 이용해, T2--weighted images [repetition time (TR)/
echo time (TE)=5000/127 ms], T1-weighted images (TR/TE=500/11 ms), T2 f luid-attenuated inversion recovery (FLAIR) images (TR/
TE=8800/127 ms), T2-gradient echo images (TR/TE=57/20 ms), three- dimensional time-of-flight MRA images (TR/TE=24/3.5 ms, slice thick- ness=1.2 mm)를 촬영하였다.
WMH는 axial FLAIR 영상에서 피질하 회백질(subcortical grey matter) 및 뇌간(brainstem)을 제외한 뇌 백질(white matter)에 공동을 형성하지 않는 고강도 신호로 정의하였다.17) WMH 부피(cm3) 측정은 임상 데이터를 모르는 상태의 신경과 전문의 1인이 독립적으로 수행 하였으며, 수작업을 거친 신호 강도 임계값을 정하여 WMH의 관심 영역(region-of-interest)을 설정하였고, digital imaging and communi- cations in medicine 형태의 MRI 영상을 MRIcro software (University of Nottingham School of Psychology, Nottingham, UK; http://www.mri- cro.com)에 적합한 형식으로 변환하여 반자동화된 기술로 계산하였 다.
3. 대사증후군의 정의
대사증후군의 정의는 2009년 American Heart Association 기준에 따라 아래와 같은 5가지 구성요소 중 3가지 이상을 만족하는 경우 로 정의하였고,18) 그 중 복부비만의 진단기준은 대한비만학회 기준 을 사용하였다.19)
1) 공복혈당 ≥100 mg/dL 또는 당뇨병 약제 복용 중인 자
2) 수축기 혈압 ≥130 mmHg 및 또는 이완기 혈압 ≥85 mmHg 또는 항고혈압제 복용 중인 자
3) 중성지방(triglyceride) ≥150 mg/dL
4) 고밀도지질단백질(high density lipoprotein, HDL) 콜레스테롤 저 하: 남자 <40 mg/dL, 여자 <50 mg/dL
5) 복부 비만: 허리둘레 남자 ≥90 cm, 여자 ≥85 cm
4. 통계 분석
WMH 부피 값이 ‘0’인 수검자가 상당수 포함되어 있어(608명, 19.2%), 데이터가 좌측 편위되는 경향을 보였다. 따라서 이로 인한 오 류를 최소화하기 위해 모든 분석에는 WMH 부피를 제곱근변환 (square root transformation)하여 사용하였다.
먼저 수검자의 일반적인 특성과 WMH 부피와의 관계를 단변량 선형회귀 분석(univariate linear regression)을 통해 비교하였다. 단변
강미소 외. 대사증후군과 WMH의 연관성 분석 Korean Journal of Family Practice
KJFP
량 선형회귀 분석 결과 연관성을 보인 요소들 중, 공선성이 있는 변 수를 최소화하고, 대사증후군의 진단기준과 중복되는 요소를 제외 하여 보정변수를 정하였다. 대사증후군 여부 및 대사증후군 요소의 개수가 WMH 부피에 끼치는 독립적인 영향을 보기 위해 다변량 선 형회귀 분석(multiple linear regression)을 시행했다. 마지막으로 제곱 근변환 한 WMH 부피 값을 다시 제곱하여 각 그룹의 평균 WMH 부 피를 구해 비교하였다.
모든 분석은 STATA software version 14.1 (StataCorp., College Sta- tion, TX, USA)을 이용하였으며, 선형회귀 계수 β 및 95% 신뢰구간 (confidence interval, CI)을 제시하였고, P값이 0.05 미만인 경우를 통 계적으로 유의한 것으로 판단하였다.
결 과
1. 대상자의 일반적 특성과 단변량 분석
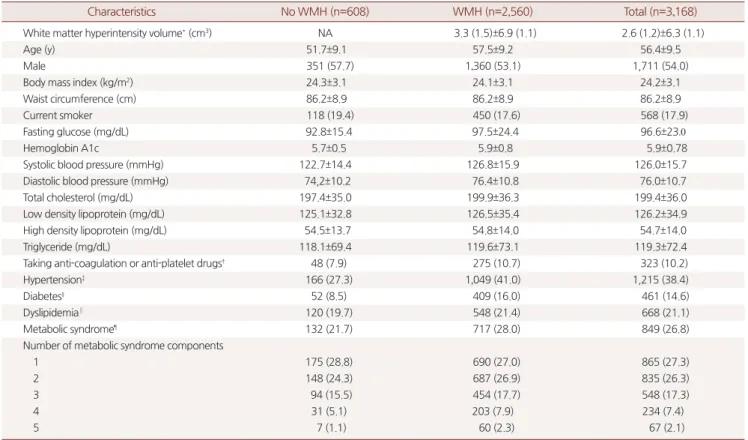
대상자 중 WMH는 2,560명(80.8%)에서 관찰되었고, 전체 대상자 의 WMH 부피의 평균은 2.6±6.3 cm3이고, 평균 연령은 56.4±9.5세였 다. 전체 대상자 중 남성은 1711명(54%)이었고, 대사증후군의 진단기 준을 만족하는 대상자는 849명(26.8%)이었다(Supplementary Table 1).
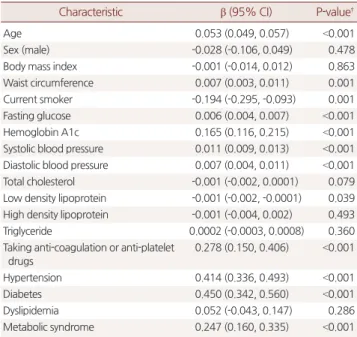
단변량 선형회귀 분석결과, 연령, 복부 둘레, 현재 흡연 여부, 공복 혈당, 당화혈색소, 수축기 및 이완기 혈압, low density lipoprotein 콜레 스테롤, 항응고제 및 항혈소판제 복용 여부, 고혈압 유무, 당뇨 유무, 대사증후군 유무가 WMH 부피와 연관성이 있었다(all P<0.05). 성별, 체질량지수(body mass index), 총 콜레스테롤, HDL 콜레스테롤, 중성 지방, 이상지질혈증 유무는 연관성이 없었다(Supplementary Table 2).
2. 대사증후군 및 대사증후군 요소의 개수와 WMH 부피와의 연관성
단변량 분석을 바탕으로 P값이 0.1 미만인 변수 중, 변수 간 공선성 을 최소화하여 연령, 복부 둘레, 현재 흡연 여부, 당화혈색소, 수축기 혈압, 총 콜레스테롤, 항응고제 및 항혈소판제 복용 여부를 보정변수 후보로 하였다. 대사증후군의 진단요소와 중복되는 요소를 제외하 고 최종적으로 연령, 현재 흡연 여부, 항응고제 및 항혈소판제 복용 여부를 보정변수로 정하였다. 더불어 본 논문의 단변량 분석에서는 연관성이 증명되지 않았으나, 여성에서 WMH 부피가 더 크다는 기
존 연구들13,20)과, 체질량지수가 증가할수록 두개 내 뇌 용적이 감소
한다는 연구결과21,22)를 고려하여 성별 및 체질량지수를 추가로 보정 하였다.
대사증후군 유무 및 대사증후군 요소의 개수와 WMH 부피와의 연관성에 대해 다변량 선형회귀분석을 시행하였다(Table 1). 대사증 후군은 WMH 부피와 유의한 상관 관계(β=0.155; P<0.001)를 보였고, 대사증후군 요소의 개수가 증가할수록 WMH 부피가 증가하는 경 향을 보였다(P for trend <0.001).
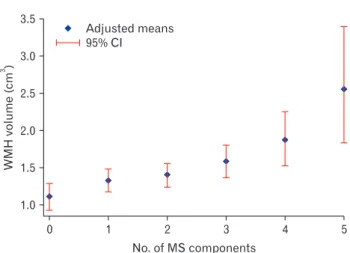
대사증후군 요소의 개수 별 WMH 부피 평균을 비교하였을 때, 5 개를 만족한 그룹이 만족하는 요소가 없는 그룹보다 약 2.3배 WMH 부피가 컸다(normal group: volume=1.106 cm3, CI, 0.933 to 1.295; Num- ber of metabolic syndrome component=5 group: volume=2.554 cm3, CI, 1.836 to 3.389) (Figure 1, Supplementary Table 3).
Table 1. Association of metabolic syndrome and white matter hyperin- tensity*
Multivariate β (95% CI) P-value†
Metabolic syndrome 0.155 (0.068, 0.242) <0.001 No. of MS components
0 Reference
1 0.097 (-0.008, 0.202) 0.069
2 0.129 (0.016, 0.241) 0.025
3 0.203 (0.074, 0.332) 0.002
4 0.315 (0.149, 0.481) <0.001
5 0.546 (0.282, 0.810) <0.001
P for trend <0.001
MS, metabolic syndrome; CI, confidence interval.
*The square root of white matter hyperintensity volume. †By multivariate linear regression analysis adjusted for age, sex, body mass index, current smoking and the use of anti-coagulation or anti-platelet drugs.
WMHvolume(cm)3
0 3.5
3.0
2.5
2.0
1.5
1.0
5 No. of MS components
Adjusted means 95% CI
4 3
2 1
Figure 1. Adjusted means of white matter hypertintensity volume by the number of metabolic syndrome components. Adjusted means of WMH volume are shown with CI (adjusted for age, sex, body mass in- dex, current smoking and the use of anti-coagulation or anti-platelet drugs).
WMH, white matter hyperintensity; MS, metabolic syndrome; CI, con- fidence intervals.
Miso Kang, et al. Association of Metabolic Syndrome with White Matter Hyperintensity
Korean Journal of Family Practice
KJFP
고 찰
본 연구는 뇌졸중 및 일과성 허혈발작의 병력이 없는 사람을 대상 으로 하여, 대사증후군과 WMH의 정량적 부피와의 연관성을 확인 하였고, 대사증후군 요소의 개수가 증가할 수록 WMH 부피가 증가 하는 경향성을 증명했다. 이러한 결과는 대사증후군이 WMH의 진 행과 관련 있음을 의미하고, WMH의 뇌졸중 및 인지기능저하의 예 측인자로써의 역할을 고려할 때, 대사증후군의 적극적 관리의 중요 성을 뒷받침한다.
그 동안 대사증후군과 WMH의 연관성을 분석했던 다른 연구와 비교해보면, 2007년 Park 등11)은 대사증후군과 WMH 유무와의 연 관성은 입증했으나, 대사증후군이 WMH 발생과는 관련이 있지만, WMH 진행에는 관련이 없을 것으로 추정했다. 2008년 Bokura 등의 연구12)에서도 로지스틱 회귀분석을 통해 대사증후군 요소의 증가 에 따라 WMH 발생이 증가하는지 분석했으나, 경향성을 증명하지 못했었다. 그러나 본 연구에서는 대사증후군 요소의 개수가 증가할 수록 WMH 부피가 증가하는 경향성을 확인하여, WMH 진행에도 대사증후군이 연관 있음을 제시하였고, 이와 같은 결과의 차이는 WMH 유무가 아닌, WMH의 부피를 정량적으로 측정함으로써 분 석의 정확도가 상승했기 때문으로 생각된다.
또한, 본 연구는 서론에 언급한 기존 유사 연구들과11-16) 비교할 때, 가장 많은 수의 WMH 유소견자를 포함한 대규모 연구로, 제곱근 변 환을 사용하여 WMH 부피의 분포를 정규화 함으로써, ‘WMH=0’값 과 관련된 가능한 바이어스를 최소화하였다. 이를 통해 WMH 부피 를 정량적으로 측정했으나, 정규분포를 따르지 않아 연속변수로 활 용하지 못했던 2012년 Portet 등14)의 연구의 단점을 보완했다.
본 연구와 유사하게 WMH 부피를 측정하고, 두개 내 전체 부피에 대한 비율로 환산하여 분석했던 연구가 있었으나, 연구 결과 대사증 후군과 WMH 부피와의 유의한 연관성은 찾지 못했었다.16) 이는 관 상동맥질환, 뇌혈관질환, 말초동맥질환, 복부 대동맥 동맥류 중 한가 지 이상을 진단받은 환자군을 대상으로 하였기 때문에 발생한 차이 로 추측된다. 신경학적으로 뇌졸중 및 일과성 허혈발작의 이상소견 이 없는 사람을 대상으로 한 우리 연구 결과에서, 이전 WMH의 정성 적 분석을 통한 연구들에서 밝혀진 대사증후군과 WMH의 연관성 이 재현된 점을 고려하면, 이미 일과성 허혈발작 및 뇌졸중의 증상 이 나타난 단계의 WMH보다 증상이 없는 WMH 단계에서 대사증 후군의 조절이 WMH 진행을 예방하는데 중요할 수 있다는 점을 시 사한다.
본 연구는 몇 가지 제한점이 있다. 먼저 단면적 연구이므로 대사 증후군과 WMH 부피의 명확한 인과관계를 파악할 수 없다. 또한, 단
일 의료기관에서 시행한 검사이므로, 일반 집단을 대표한다고 보기 어려우므로, 여러 의료기관의 자료를 바탕으로, WMH 위치에 따른 분류를 고려한 추가적인 분석이 필요할 것으로 생각된다.
결론적으로 대사 증후군과 WMH 부피는 연관성이 있으며 대사 증후군 요소의 개수가 증가할 수록 WMH 부피도 증가하는 경향을 보였다. 이는, 대사증후군 요소에 대한 생활습관 교정 등의 적극적인 조절을 통해 무증상 WMH 진행의 예방에 기여할 가능성을 제시하 였다. 향후 정확한 인과관계 및 상관 정도를 평가하기 위한 전향적 연구가 필요하다.
요 약
연구배경:
White matter hyperintensity (WMH)는 혈관의 만성적인 허혈성 손상으로 인해 발생하는 병변으로, 뇌졸중 및 인지기능저하 의 예측 인자이다. 대사증후군은 동맥경화 등 혈관 변화에 기여하는 위험요소로, 본 연구는 뇌졸중 및 일과성 허혈발작의 병력이 없는 성인에서 두 질환의 연관성을 분석하고자 하였다.방법:
2006년 1월부터 2013년 12월까지 건강검진을 받은 수검자 중, 뇌졸중 및일과성 허혈발작의 병력이 없으며, 뇌 자기공명영상을 촬 영한 3,168명을 대상으로 하였다. WMH 부피를 정량적으로 측정한 후, 데이터 정규분포를 위해 측정값을 제곱근변환(square root)하여 분석에 이용하였다. 대사증후군은 2009년 AHA 진단기준에 따라 5 가지 구성요소 중 3가지 이상을 만족하는 경우로 정의하였다. 두 질 환의 연관성 분석을 위해 연령, 성별, 체질량지수, 현재 흡연 여부, 항 응고제 및 항혈소판제 복용 여부를 보정변수로 하여 다변량 선형회 귀분석을 시행하였다.결과:
대상자의 평균연령은 56.4세로, WMH 부피의 평균은 2.6 cm3 였으며, 대사증후군의 유병률은 26.8% (849명)였다. 다변량 선형회귀 분석결과 대사증후군은 WMH 부피와 유의한 상관 관계(β=0.155;P<0.001)를 보였고, 대사증후군 요소의 개수가 증가할수록 WMH 부 피가 증가하는 경향을 보였다(P for trend <0.001).
결론:
대사 증후군과 WMH 부피는 연관성이 있으며, 특히 진단 기 준을 많이 만족할 수록 WMH 부피가 증가했다. 향후 정확한 인과관 계 및 상관 정도를 평가하기 위해 전향적 연구가 필요할 것으로 생각 된다.중심단어:
Leukoaraiosis; 대사증후군; 뇌 자기공명영상; 뇌혈관질환강미소 외. 대사증후군과 WMH의 연관성 분석 Korean Journal of Family Practice
KJFP
REFERENCES
1. Debette S, Markus HS. The clinical importance of white matter hyperinten- sities on brain magnetic resonance imaging: systematic review and meta- analysis. BMJ 2010; 341: c3666.
2. Longstreth WT Jr, Manolio TA, Arnold A, Burke GL, Bryan N, Jungreis CA, et al. Clinical correlates of white matter findings on cranial magnetic reso- nance imaging of 3301 elderly people. The Cardiovascular Health Study.
Stroke 1996; 27: 1274-82.
3. Pantoni L, Garcia JH. Pathogenesis of leukoaraiosis: a review. Stroke 1997;
28: 652-9.
4. van Dijk EJ, Breteler MM, Schmidt R, Berger K, Nilsson LG, Oudkerk M, et al. The association between blood pressure, hypertension, and cerebral white matter lesions: cardiovascular determinants of dementia study. Hy- pertension 2004; 44: 625-30.
5. Ferguson SC, Blane A, Perros P, McCrimmon RJ, Best JJ, Wardlaw J, et al.
Cognitive ability and brain structure in type 1 diabetes: relation to microan- giopathy and preceding severe hypoglycemia. Diabetes 2003; 52: 149-56.
6. Gons RA, van Norden AG, de Laat KF, van Oudheusden LJ, van Uden IW, Zwiers MP, et al. Cigarette smoking is associated with reduced microstruc- tural integrity of cerebral white matter. Brain 2011; 134: 2116-24.
7. Soler EP, Ruiz VC. Epidemiology and risk factors of cerebral ischemia and ischemic heart diseases: similarities and differences. Curr Cardiol Rev 2010;
6: 138-49.
8. Cortez-Dias N, Martins S, Belo A, Fiuza M; Investigadores do estudo VAL- SIM. Comparison of definitions of metabolic syndrome in relation to risk for coronary artery disease and stroke. Rev Port Cardiol 2011; 30: 139-69.
9. Yaffe K, Kanaya A, Lindquist K, Simonsick EM, Harris T, Shorr RI, et al. The metabolic syndrome, inflammation, and risk of cognitive decline. JAMA 2004; 292: 2237-42.
10. Schmidt R, Ropele S, Enzinger C, Petrovic K, Smith S, Schmidt H, et al.
White matter lesion progression, brain atrophy, and cognitive decline: the Austrian stroke prevention study. Ann Neurol 2005; 58: 610-6.
11. Park K, Yasuda N, Toyonaga S, Yamada SM, Nakabayashi H, Nakasato M, et al. Significant association between leukoaraiosis and metabolic syndrome in healthy subjects. Neurology 2007; 69: 974-8.
12. Bokura H, Yamaguchi S, Iijima K, Nagai A, Oguro H. Metabolic syndrome is
associated with silent ischemic brain lesions. Stroke 2008; 39: 1607-9.
13. Choi HS, Cho YM, Kang JH, Shin CS, Park KS, Lee HK. Cerebral white mat- ter hyperintensity is mainly associated with hypertension among the com- ponents of metabolic syndrome in Koreans. Clin Endocrinol (Oxf) 2009;
71: 184-8.
14. Portet F, Brickman AM, Stern Y, Scarmeas N, Muraskin J, Provenzano FA, et al. Metabolic syndrome and localization of white matter hyperintensities in the elderly population. Alzheimers Dement 2012; 8(5 Suppl): S88-95.e1.
15. Seo J, Kye S, Lee GI, Kim J, Lee J, Lee J, et al. Association between Metabolic syndrome with Leukoaraiosis in 50s healthy Korean men. Korean J Fam Pract 2015; 5(Suppl 3): S610-4.
16. Tiehuis AM, van der Graaf Y, Mali WP, Vincken K, Muller M, Geerlings MI;
SMART Study Group. Metabolic syndrome, prediabetes, and brain abnor- malities on mri in patients with manifest arterial disease: the SMART-MR study. Diabetes Care 2014; 37: 2515-21.
17. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al.
Neuroimaging standards for research into small vessel disease and its con- tribution to ageing and neurodegeneration. Lancet Neurol 2013; 12: 822-38.
18. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Preven- tion; National Heart, Lung, and Blood Institute; American Heart Associa- tion; World Heart Federation; International Atherosclerosis Society; and In- ternational Association for the Study of Obesity. Circulation 2009; 120:
1640-5.
19. Lee S, Park HS, Kim SM, Kwon HS, Kim DY, Kim DJ, et al. Cut-off points of waist circumference for defining abdominal obesity in the Korean popula- tion. Korean J Obes 2006; 15: 1-9.
20. Sachdev PS, Parslow R, Wen W, Anstey KJ, Easteal S. Sex differences in the causes and consequences of white matter hyperintensities. Neurobiol Aging 2009; 30: 946-56.
21. Ward MA, Carlsson CM, Trivedi MA, Sager MA, Johnson SC. The effect of body mass index on global brain volume in middle-aged adults: a cross sec- tional study. BMC Neurol 2005; 5: 23.
22. Gunstad J, Paul RH, Cohen RA, Tate DF, Spitznagel MB, Grieve S, et al. Rela- tionship between body mass index and brain volume in healthy adults. Int J Neurosci 2008; 118: 1582-93.
Table 1 . Baseline characteristics of study subjects
Characteristics No WMH (n=608) WMH (n=2,560) Total (n=3,168)
White matter hyperintensity volume* (cm3) NA 3.3 (1.5)±6.9 (1.1) 2.6 (1.2)±6.3 (1.1)
Age (y) 51.7±9.1 57.5±9.2 56.4±9.5
Male 351 (57.7) 1,360 (53.1) 1,711 (54.0)
Body mass index (kg/m2) 24.3±3.1 24.1±3.1 24.2±3.1
Waist circumference (cm) 86.2±8.9 86.2±8.9 86.2±8.9
Current smoker 118 (19.4) 450 (17.6) 568 (17.9)
Fasting glucose (mg/dL) 92.8±15.4 97.5±24.4 96.6±23.0
Hemoglobin A1c 5.7±0.5 5.9±0.8 5.9±0.78
Systolic blood pressure (mmHg) 122.7±14.4 126.8±15.9 126.0±15.7
Diastolic blood pressure (mmHg) 74,2±10.2 76.4±10.8 76.0±10.7
Total cholesterol (mg/dL) 197.4±35.0 199.9±36.3 199.4±36.0
Low density lipoprotein (mg/dL) 125.1±32.8 126.5±35.4 126.2±34.9
High density lipoprotein (mg/dL) 54.5±13.7 54.8±14.0 54.7±14.0
Triglyceride (mg/dL) 118.1±69.4 119.6±73.1 119.3±72.4
Taking anti-coagulation or anti-platelet drugs† 48 (7.9) 275 (10.7) 323 (10.2)
Hypertension‡ 166 (27.3) 1,049 (41.0) 1,215 (38.4)
Diabetes§ 52 (8.5) 409 (16.0) 461 (14.6)
Dyslipidemia∥ 120 (19.7) 548 (21.4) 668 (21.1)
Metabolic syndrome¶ 132 (21.7) 717 (28.0) 849 (26.8)
Number of metabolic syndrome components
1 175 (28.8) 690 (27.0) 865 (27.3)
2 148 (24.3) 687 (26.9) 835 (26.3)
3 94 (15.5) 454 (17.7) 548 (17.3)
4 31 (5.1) 203 (7.9) 234 (7.4)
5 7 (1.1) 60 (2.3) 67 (2.1)
Values are presented as mean±standard deviation or numbers of participants (%).
WMH, white matter hyperintensity; NA, not applicable; SBP, systolic blood pressure; DBP, Diastolic blood pressure; HbA1c, hemoglobin A1c.
*The square root of white matter hyperintensity volume. †Subjects taking aspirin, plavix, warfarin, or other antiplatelet drugs. ‡Subjects taking antihypertensive drugs or with a SBP ≥140 mmHg, or a DBP ≥90 mmHg. §Subjects taking antidiabetic drugs or with a fasting blood glucose ≥126 mg/dL or a HbA1c ≥6.5%. ∥Subjects taking lipid lowering drugs or with a total cholesterol level ≥240 mg/dL. ¶Subjects having three or more of the diagnostic criteria.
Table 2. Association of the base characteristics and white matter hy- perintensity*
Characteristic β (95% CI) P-value†
Age 0.053 (0.049, 0.057) <0.001
Sex (male) -0.028 (-0.106, 0.049) 0.478
Body mass index -0.001 (-0.014, 0.012) 0.863
Waist circumference 0.007 (0.003, 0.011) 0.001
Current smoker -0.194 (-0.295, -0.093) 0.001
Fasting glucose 0.006 (0.004, 0.007) <0.001
Hemoglobin A1c 0.165 (0.116, 0.215) <0.001
Systolic blood pressure 0.011 (0.009, 0.013) <0.001 Diastolic blood pressure 0.007 (0.004, 0.011) <0.001
Total cholesterol -0.001 (-0.002, 0.0001) 0.079
Low density lipoprotein -0.001 (-0.002, -0.0001) 0.039 High density lipoprotein -0.001 (-0.004, 0.002) 0.493
Triglyceride 0.0002 (-0.0003, 0.0008) 0.360
Taking anti-coagulation or anti-platelet drugs
0.278 (0.150, 0.406) <0.001
Hypertension 0.414 (0.336, 0.493) <0.001
Diabetes 0.450 (0.342, 0.560) <0.001
Dyslipidemia 0.052 (-0.043, 0.147) 0.286
Metabolic syndrome 0.247 (0.160, 0.335) <0.001
CI, confidence interval.
*The square root of white matter hyperintensity volume. †By univariate linear re- gression analysis.