서 론
전립선 비대증은 전립선이 비대해져 하부 요로의 폐색을 일으켜 소변의 흐름 감소상태를 야기하는데,1) 증상으로는 소변의 흐름을 막 는 하부요로 폐색증상을 전립선비대증으로 정의한다.2) 조직학적으 로는 전립선 간질이나 전립선의 상피세포가 증식한 것으로,2) 크기로
는 전립선 크기가 25 mL 이상을 전립선 비대증으로 정의하고 있다.3) 전립선비대증은 중년 이후의 남성에서 흔한 질환 중의 하나이며, 연령이 증가할수록 그 유병률이 증가하는 만성 진행성 질환이다.4,5) 전립선 크기가 클수록 급성 소변 저류, 신기능 저하, 반복적인 요로 감염, 요실금 등의 증상을 동반하는 전립선비대증으로 진행할 위험 이 높다.6,7)
Received March 9, 2017 Revised August 31, 2017 Accepted September 3, 2017
Corresponding author Da-Hye Choi Tel: +82-42-939-0314, Fax: +82-42-939-0567 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-0522-982X
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.1.39 eISSN 2233-9116
Korean J Fam Pract. 2018;8(1):39-46
Korean Journal of Family Practice
KJFP
전립선 용적 및 전립선 특이항원과 대사적 요소의 연관성
김택영, 최다혜*, 이태영, 문현철, 안영인, 박성지, 정명철
대전보훈병원 가정의학과
Association of Metabolic Factors with Prostate Volume and Prostate-Specific Antigen
Taek-Young Kim, Da-Hye Choi*, Tae-Young Lee, Hyun-Chul Moon, Young-In An, Seong-Jee Park, Myung-Chul Jung Department of Family Medicine, Daejeon Veterans Hospital, Daejeon, Korea
Background: This study was undertaken to evaluate the association of metabolic factors with prostate volume and prostate specific antigen in Korean adult men.
Methods: From January 2011 to December 2015, 268 male patients in a Daejeon Veterans Hospital were enrolled in a retrospective study. Exceptions were patients who were diagnosed with prostate-related diseases such as benign prostatic hyperplasia, prostatitis, or prostate cancer. The association of the results of anthropometric measurements of height, weight, waist circumference, body mass index (BMI), systolic and diastolic blood pressure, and blood chemistry values for fasting blood glucose, total cholesterol, high density lipoprotein, low density lipoprotein, triglyceride, aspartate transaminase, alanine transaminase and gamma-glutamyl transferase with prostate volume and prostate-specific antigen were analyzed by independent-samples t-test, Pearson correlation test, and multiple linear regression analysis. We also analyzed the relationship between metabolic syndrome and the prostate volume and prostate-specific antigen, and in reverse we analyzed the relationship between prostate volume and prostate-specific antigen on metabolic syndrome.
Results: Prostate volume was significantly increased with waist circumference and fasting blood glucose. In addition, as the BMI increased, the prostate- specific antigen level decreased statistically. However, the prevalence of metabolic syndrome, and prostate volume and prostate-specific antigen levels were not found to be statistically significant.
Conclusion: In Korean adult men, waist circumference (P<0.05) and fasting blood glucose (regression coefficient [β]±standard errors [SE]=0.051±0.018, P<0.01) have a positive correlation with prostate volume, and body mass index and prostate-specific antigen have a negative correlation (β±SE=-0.059±0.019, P<0.01).
Keywords: Prostate; Prostate-Specific Antigen; Waist Circumference; Blood Glucose; Body Mass Index; Metabolic Syndrome
Taek-Young Kim, et al. Association of Metabolic Factors with Prostate Volume and Prostate-Specific Antigen
Korean Journal of Family Practice
KJFP
전립선비대증의 병인으로는 연령과 고환성 안드로젠이 알려져 있다.8) 이외에도 인슐린 저항성, 지질대사이상, 복부비만 등의 대사 증후군과의 관련성에 대한 연구가 보고되고 있으나, 전립선비대증 과 이들 대사증후군 및 그 요소와의 관련성에 대한 이전의 연구결 과들은 서로 일치하지 않으며, 상호 간에 이견이 많다. Qu 등9)은 당 뇨병을 가지고 있는 남성의 전립선 용적과 특이항원(prostate-specific antigen, PSA) 수치가 당뇨병이 없는 남성에 비해 증가해 있다는 연구 결과를 보고하였으며, Yim 등1)은 공복혈당과 허리둘레가 증가할수 록 전립선 용적이 증가한다고 보고하였다. 반면 Wallner 등10)은 당뇨 병이 있는 것과 당수치가 잘 조절되지 않는 것은 전립선 용적과 연관 성이 없다는 연구 결과를 보고하였다. 기존의 관련 연구들은 연구 방법과 대상군 선정에 차이가 있으며, 전립선 용적에 영향을 주는 다른 요인의 영향에 대한 분석이 제한적이어서 일관된 결과를 이끌 어 내는 데 한계가 있는 것으로 판단된다.
아직까지 국내의 경우 전립선 용적 및 전립선 특이항원(PSA)과 대 사적 요소의 연관성에 관한 연구가 부족하고, 대사증후군 유무에 따른 차이만을 보거나 대사적 요소만 별개로 분석할 경우에도 연구 별로 대상군의 연령대에 차이가 있었다. 이에 본 연구에서는 전립선 관련 기저 질환으로 치료를 받고 있지 않은 41세부터 70세 남성을 대 상으로 전립선 용적 및 PSA 수치와 대사적 요소들 및 대사증후군과 의 연관성을 조사하였다.
방 법
1. 연구 대상
본 연구는 2011년 1월부터 2015년 12월까지 5년간 대전보훈병원에 내원하여 종합건강검진을 시행 받은 대상자 중 전립선 초음파검사 를 시행한 41세 이상 70세 이하의 남성 대상자 321명을 선정하였다.
이 중 기존에 전립선 비대증, 전립선염이나 전립선암 등의 전립선 관 련 질환을 진단받은 환자 53명을 제외하고 최종 268명을 대상으로 후향적 연구를 진행하였으며, 이중 허리둘레를 계측한 65명에 대해 서도 별도로 분석을 시행하였다.
2. 측정 1) 신체계측
신장, 체중, 허리둘레, 체질량지수(body mass index, BMI), 수축기 및 이완기 혈압의 신체 계측을 숙련된 검사자에 의해 측정하였다. 체 질량지수(BMI)는 체중을 키의 제곱으로 나눈 값(kg/m2)으로 정의하 였다.
2) 검사실 검사
혈액검사는 8시간 이상 금식 후 채혈한 공복혈당, 총콜레스테롤, 고밀도 지질단백(high density lipoprotein, HDL), 저밀도 지질단백(low density lipoprotein, LDL), 중성지방, aspartate transaminase (AST), ala- nine transaminase (ALT), gamma-glutamyl transferase (GGT)의 혈액화 학검사 수치를 본원 종합건강검진 데이터를 이용하여 수집하였고, 동시에 전립선 특이항원(PSA) 수치도 수집하였다. 전립선 특이항원 의 경우 Architect-i2000 (Abbott Laboratories, Abbott Park, IL, USA)을 사용하여 total PSA를 측정하였다.
3) 전립선 크기 측정
전립선 크기 측정은 GE LOGIQ 9 ultrasound scanner (GE Health- care, Waukesha, WI, USA) 기기의 4C probe를 이용하여 전립선의 높 이(H), 넓이(W), 길이(L)를 측정하고, 타원체공식(π/6×W×H×L)에 대 입하여 전립선 용적을 계산하였다.11) 전립선 용적이 25 mL 이상인 경 우 전립선 비대가 있다고 정의하였다.3) 또한 전립선암으로 인한 전립 선 용적 증가를 배제하기 위해서 직장수지검사를 병행하였다.
3. 대사증후군의 진단 기준
본 연구에 사용된 대사증후군 진단 기준은 2009년에 국제당뇨병 연맹(International Diabetes Federation, IDF)과 미국심장협회(Ameri- can Heart Association, AHA)/미국심장폐혈액연구원(National Heart Lung and Blood Institute, NHLBI)의 합동 선언에서 제시한 진단 기준 에 따라 아래 5가지 중 3가지 이상 만족하는 경우로 정의하였다.12) 인 종이나 국가에 따라 정한 허리둘레 기준으로는 대한비만학회에서 우리나라의 복부비만으로 제시한 기준13)을 사용하였다. 구체적인 기준은 다음과 같다.
1) 남성에서 허리둘레 90 cm 이상, 여성에서 허리둘레 85 cm 이상인 경우
2) 중성지방 150 mg/dL 이상이거나 지질강하제 약물을 투여 하는 경우
3) HDL 콜레스테롤 40 mg/dL 미만이거나 지질강하제 약물을 투여하는 경우
4) 수축기 혈압 130 mmHg 이상 혹은 이완기 혈압 8 mmHg 이상이거나 혈압강하제 투여하는 경우
5) 공복혈당 100 mg/dL 이상이거나 혈당강하를 위해 약물 투 여하는 경우
4. 통계 분석
전립선 비대가 있는 경우와 없는 경우의 대사적 요소 수치 및 PSA
김택영 외. 전립선 용적 및 전립선 특이항원과 대사적 요소의 연관성 Korean Journal of Family Practice
KJFP
수치를 비교하기 위하여 independent-samples t-test를 시행하였다. 또 한 수집된 대사적 요소 중에서 대사증후군 진단 기준에 포함되는 요소에 대해서 추가적인 independent-samples t-test를 시행하여 대사 증후군 진단 기준에 따른 전립선 용적 및 PSA 수치를 비교하였다. 대 사적 요소 수치 및 대사증후군 구성요소들과 PSA 수치와 전립선 용 적 간의 상관관계를 분석하기 위해 Pearson’s correlation test를 시행하 였다. 유의한 상관성이 확인되는 경우에는 다른 항목의 교란 영향을 배제하고 분석하기 위해 다중선형회귀분석(multiple linear regression analysis)을 시행하였다.
모든 통계학적 분석은 IBM SPSS Statistics version 23.0 프로그램 (IBM Co., Armonk, NY, USA)을 이용하였으며, P 값(P-value)이 0.05 미 만일 때 통계적으로 유의한 것으로 판정하였다.
결 과
1. 전립선 부피에 따른 연구 표본의 일반적 특성
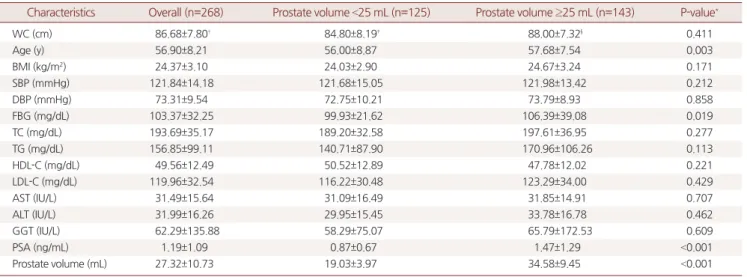
연구 대상자 268명 중 전립선 용적 25 mL 미만인 군은 125명 (46.64%)이었으며, 전립선 용적이 25 mL 이상인 군은 143명(53.36%)이 었다. 평균 나이는 전체 56.9세, 전립선 용적 25 mL 미만인 군 56.0세, 전립선 용적 25 mL 이상인 군은 57.7세였다. 전립선 용적 25 mL 미만 인 군에서 공복혈당 99.93 mg/dL, 전립선 용적 25 mL 이상인 군에서 공복혈당은 106.39 mg/dL로 대사적 요소들 중 공복혈당 수치가 두 군간 통계적으로 유의하게 차이가 있었다(P=0.019). 전립선 평균 혈
청 PSA 수치는 전체 1.19 ng/mL, 전립선 용적 25 mL 미만인 군 0.87 ng/mL, 전립선 용적 25 mL 이상인 군은 1.47 ng/mL였다. 평균 전립선 용적은 전체 27.32 mL, 전립선 용적 25 mL 미만인 군 19.03 mL, 25 mL 이상인 군은 34.58 mL였다. 공복혈당 외에도 연령과 PSA 수치가 전립 선 용적 25 mL 이상인 군에서 통계적으로 유의하게 높았다(Table 1).
2. 대사증후군 진단 기준 개별 요소에 따른 전립선 용적 및 전립선 특이항원 수치
전립선 용적 및 PSA 수치와 대사적 요소들 및 대사증후군과의 연 관성을 분석해 보았다. 전립선 용적은 허리둘레 90 cm 이상인 군에 서 31.03 mL, 90 cm 미만인 군에서 25.41 mL로 양 군에서 통계적으로 유의한 차이가 있었고(P=0.005), 공복혈당 100 mg/dL 이상인 군에서 28.57 mL, 공복혈당 100 mg/dL 미만인 군에서 26.37 mL로 통계적으 로 유의한 차이가 있었다(P=0.025). 40대, 50대, 60대 연령별로 구분하 여 전립선 용적과 PSA 수치에 대하여 대사증후군과의 연관성을 확 인했을 경우에 40대에서는 연관성을 확인할 수 없었고, 50대에서는 PSA 수치가 수축기 혈압, 이완기 혈압, 중성지방에 대하여 통계적으 로 유의한 차이가 있었으나 중성지방의 경우에는 중성지방이 높은 군보다 낮은 군에서 PSA 수치가 높았고, 60대에서는 전립선 용적과 PSA 수치가 허리둘레와 중성지방에 대하여 통계적으로 유의한 차 이가 있었으나, 중성지방의 경우에는 중성지방이 높은 군보다 낮은 군에서 전립선 용적이 크고(P=0.006) PSA 수치가 높았다(P=0.009).
대사증후군 진단 기준 개별 요소들과의 연관성이 확인되는 분분히
Table 1. Baseline characteristics of study participants by prostate volume
Characteristics Overall (n=268) Prostate volume <25 mL (n=125) Prostate volume ≥25 mL (n=143) P-value*
WC (cm) 86.68±7.80† 84.80±8.19‡ 88.00±7.32§ 0.411
Age (y) 56.90±8.21 56.00±8.87 57.68±7.54 0.003
BMI (kg/m2) 24.37±3.10 24.03±2.90 24.67±3.24 0.171
SBP (mmHg) 121.84±14.18 121.68±15.05 121.98±13.42 0.212
DBP (mmHg) 73.31±9.54 72.75±10.21 73.79±8.93 0.858
FBG (mg/dL) 103.37±32.25 99.93±21.62 106.39±39.08 0.019
TC (mg/dL) 193.69±35.17 189.20±32.58 197.61±36.95 0.277
TG (mg/dL) 156.85±99.11 140.71±87.90 170.96±106.26 0.113
HDL-C (mg/dL) 49.56±12.49 50.52±12.89 47.78±12.02 0.221
LDL-C (mg/dL) 119.96±32.54 116.22±30.48 123.29±34.00 0.429
AST (IU/L) 31.49±15.64 31.09±16.49 31.85±14.91 0.707
ALT (IU/L) 31.99±16.26 29.95±15.45 33.78±16.78 0.462
GGT (IU/L) 62.29±135.88 58.29±75.07 65.79±172.53 0.609
PSA (ng/mL) 1.19±1.09 0.87±0.67 1.47±1.29 <0.001
Prostate volume (mL) 27.32±10.73 19.03±3.97 34.58±9.45 <0.001
Values are presented as mean±standard deviation.
WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; TC, total cholesterol; TG, triglyc- eride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma- glutamyl transferase; PSA, prostate-specific antigen.
*P-values were obtained by independent-samples t-test. †Number of subjects who measured waist circumference was 65 persons. ‡Number of subjects with a prostate volume less than 25 mL in the waist circumference is 27 persons. §Number of subjects with a prostate volume of 25 mL or more in the waist circumference is 38 persons.
Taek-Young Kim, et al. Association of Metabolic Factors with Prostate Volume and Prostate-Specific Antigen
Korean Journal of Family Practice
KJFP
Table 2. Prostate volume and PSA level according to metabolic syndrome components
Variable
Age (y)
Overall 41–50 51–60 61–70
N Prostate volume (mL)
PSA level
(ng/mL) N Prostate volume (mL)
PSA level
(ng/mL) N Prostate volume (mL)
PSA level
(ng/mL) N Prostate volume (mL)
PSA level (ng/mL) SBP
≥130 mmHg 87 26.44 1.24 17 24.60 1.01 30 25.22 1.25* 40 28.15 1.33
<130 mmHg 181 27.75 1.24 52 23.73 1.03 52 28.90 0.89* 77 29.68 1.44
DBP
≥85 mmHg 31 25.86 1.17 9 25.50 1.04 14 25.38 1.49* 8 27.10 1.50
<85 mmHg 237 27.52 1.36 60 23.72 0.79 68 28.00 0.93* 109 29.31 1.40
TG
≥150 mg/dL 111 27.43 1.08* 27 24.17 1.15 39 28.21 0.90* 45 28.70* 1.19*
<150 mg/dL 157 27.25 1.27* 42 23.81 0.94 43 26.96 1.14* 72 29.44* 1.54*
HDL-C
≥40 mg/dL 200 27.00 1.19 51 23.50 1.03 63 26.32 1.01 86 29.57 1.42
<40 mg/dL 68 28.29 1.19 18 25.22 1.00 19 31.65 1.08 31 28.02 1.36
FBG
≥100 mg/dL 116 28.57* 1.18 28 24.13 1.09 36 28.70 0.98 52 30.87 1.35
<100 mg/dL 152 26.37* 1.20 41 23.82 0.98 46 26.66 1.06 65 27.78 1.44
WC
≥90 cm 22 31.03* 1.45 2 21.74 1.28 11 26.63 0.78 9 38.47* 2.31*
<90 cm 43 25.41* 1.17 16 25.69 1.20 13 24.95 1.50 14 25.50* 0.84*
MS
Yes 31 29.45 1.28 3 21.40 1.22 13 25.23* 0.82 15 34.70 1.7*
No 34 25.35 1.25 15 26.02 1.20 11 26.30* 1.56 8 22.80 0.88*
Values are presented as number or mean.
PSA, prostate-specific antigen; N, number of subjects; SBP, systolic blood pressure; DBP, diastolic blood pressure; TG, triglyceride; HDL-C, high density lipoprotein cho- lesterol, FBG, fasting blood glucose; WC, waist circumference; MS, metabolic syndrome.
*P<0.05, P-values were obtained by independent-samples t-test.
Table 3. Correlation coefficient between prostate volume, PSA and other variables Variable
Age (y)
Overall (n=268) 41–50 (n=69) 51–60 (n=82) 61–70 (n=117)
Prostate volume PSA level Prostate volume PSA level Prostate volume PSA level Prostate volume PSA level
Age (y) 0.186* 0.184* 0.175 0.058 0.015 0.112 –0.076 0.182*
BMI (kg/m2) 0.099 -0.133* 0.012 -0.049 0.184 -0.146 0.113 -0.122
WC (cm)† 0.250* 0.024 0.158 -0.082 0.180 -0.238 0.350 0.263
SBP (mmHg) -0.020 0.016 0.142 -0.030 -0.122 0.081 –0.071 -0.024
DBP (mmHg) 0.015 0.040 0.007 -0.017 -0.145 0.105 0.126 0.075
FBG (mg/dL) 0.154* -0.005 0.005 -0.019 0.220 -0.036 0.172 0.061
TC (mg/dL) 0.099 0.110 0.100 0.244* 0.119 0.178 0.150 0.083
TG (mg/dL) 0.054 -0.105 0.032 -0.054 0.040 -0.130 0.047 -0.076
HDL-C (mg/dL) -0.043 0.097 –0.104 -0.029 -0.336* 0.032 0.075 0.134
LDL-C (mg/dL) 0.089 0.114 0.132 0.267* 0.131 0.207 0.113 0.068
AST (IU/L) 0.024 -0.006 –0.140 -0.075 0.038 0.018 –0.007 -0.042
ALT (IU/L) 0.098 -0.029 –0.159 -0.128 0.202 0.067 0.178 -0.017
GGT (IU/L) 0.027 -0.038 0.059 -0.078 0.135 -0.099 0.023 -0.049
PSA (ng/mL) 0.445* 0.545* 0.217 0.497*
Values are presented as mean.
PSA, prostate-specific antigen; WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose;
TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma-glutamyl transferase.
*P<0.05, P-values were obtained by Pearson's correlation test. †Number of subjects who measured waist circumference was 65 persons.
김택영 외. 전립선 용적 및 전립선 특이항원과 대사적 요소의 연관성 Korean Journal of Family Practice
KJFP
있었으나, 60대에서 대사증후군 환자가 PSA 수치가 유의하게 상승 한 것을 제외하고는 대사증후군 진단 유무가 전립선 용적과 PSA수 치와 통계적으로 유의한 연관성은 없었다(Table 2).
3. 전립선 용적, 전립선 특이항원 및 대사적 요소들 간의 연관성
대사적 요소별로 전립선 용적과 PSA와의 연관성을 Pearson’s cor- relation test로 확인해 보았다. 나이가 증가할수록 전립선 용적과 혈 청 PSA 수치가 통계적으로 유의하게 상승하는 것이 확인되었다. 허 리둘레, 공복혈당, PSA 수치가 증가할수록 전립선 용적이 유의하게 상승하였고, PSA 수치는 체질량지수(BMI)와 음의 상관관계가 확인 되었다. 40대, 50대, 60대 연령별로 구분하여 동일한 분석을 시행하였 다. 40대에서는 전립선 용적이 PSA 수치와 양의 상관관계가 있었고, PSA 수치가 총콜레스테롤 수치, LDL 수치와 양의 상관관계가 확인 되었다. 50대에서는 전립선 용적이 HDL 수치와 음의 상관관계가 확 인되었다. 60대에서는 전립선 용적이 PSA 수치와 양의 상관관계가 있었고, PSA 수치가 나이와 양의 상관관계가 확인되었다(Table 3).
4. 전립선 용적 및 전립선 특이항원과 대사적 요소들 간의 연관성에 대한 다중회귀분석
대사적 요소들 간에 교란 영향을 줄 수 있는 요인들을 배제하기 위해 Pearson’s correlation test분석 결과에서 통계적으로 유의하게 확 인된 대사적 요소만을 사용하여 다중회귀분석을 시행하여 독립적 인 연관성을 확인해 보았다. 통계적으로 유의하게 확인된 대사적 요 소들 중 전체 연령대에서 상관관계가 확인된 대사적 요소들만 사용 하였다. 전립선 용적에 대하여 공복혈당(P=0.004)과 PSA 수치(P<
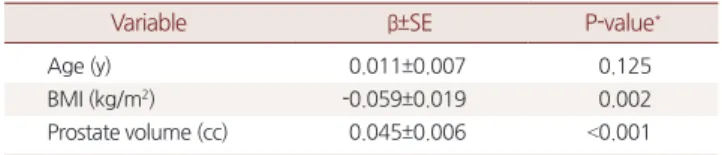
0.001)가 다른 대사적 요소들과 독립적으로 통계적으로 유의하게 연 관성이 있는 것으로 분석되었다(Table 4). PSA 수치에 대하여 BMI
(P=0.002)와 전립선 용적(P<0.001)이 다른 대사적 요소들과 독립적으 로 통계적으로 유의하게 연관성이 있는 것으로 분석되었다(Table 5).
고 찰
본 연구는 한국 성인 남성에서 대사적 요소와 전립선 용적 및 전 립선 특이항원의 연관성을 평가하기 위하여 수행되었다. 허리둘레 와 공복혈당이 증가할수록 전립선 용적이 통계적으로 유의하게 증 가하였으며 체질량지수가 증가할수록 전립선 특이항원 수치가 통 계적으로 유의하게 감소하였다. 그러나 대사증후군의 유병 여부와 전립선 용적과 전립선 특이항원 수치는 통계적으로 유의한 연관성 이 없는 것으로 확인되었다.
대사증후군은 인슐린 저항성을 공통된 특징으로 하는 심혈관질 환 발생 및 사망과 관련된 위험인자의 군집이다.14) 대사증후군의 기 본 병태생리로는 인슐린 저항성으로 인해 인슐린 매개성 포도당 흡 수 장애가 발생하고 이로 인해 이차적으로 발생하는 고인슐린혈증 이 알려져 있다.15) 또한, 대사증후군은 에스트로겐, 테스토스테론의 대사와 밀접한 연관이 있는 것으로 보고되고 있다.16)
전립선비대증의 기전을 설명하는 정확한 병인은 알려지지 않았으 나 다음과 같은 주장들이 제기되고 있다. 첫째로 고인슐린혈증은 시 상하부에 영향을 주어 카테콜아민의 증가를 야기하여 교감신경계 의 항진을 유발한다. 이러한 증가된 교감신경계의 활동이 전립선 평 활근 및 후속 방광 출구 폐색에 기여해 전립선 비대증에 동반되는 하부요로증상을 유발할 수 있다.17) 둘째로 전립선을 포함한 많은 장 기의 생리적 및 병리학적 성장 조절에 관여하는 인슐린유사성장인 자-1 (insulin-like growth factor-1, IGF-1)의 조절 장애가 전립선비대증 과 전립선암의 발병과 관련이 있는데 인슐린은 인슐린유사성장인 자-1 (IGF-1)과 구조적으로 유사하기 때문에 인슐린유사성장인자-1 (IGF-1) 수용체와 결합하여 전립선 세포로 들어가 전립선의 성장 및 증식을 유발할 수 있다.18) 셋째로 테스토스테론과 에스트로겐 등의 스테로이드 호르몬의 이상분비가 전립선비대증에 관여할 수 있는 데, 쥐를 대상으로 시행한 연구에서 쥐를 거세시킨 후 전립선이 위축 Table 4. Multiple regression analysis regarding the association be-
tween prostate volume and other variables
Variable β±SE P-value*
Measurement of WC (n=65)
Age (y) 0.179±0.139 0.203
WC (cm) 0.226±0.139 0.110
FBG (mg/dL) 0.036±0.029 0.220
PSA (ng/mL) 4.161±0.725 <0.001
Overall (n=268)
Age (y) 0.138±0.072 0.055
FBG (mg/dL) 0.051±0.018 0.004
PSA (ng/mL) 4.208±0.541 <0.001
β, regression coefficient; SE, standard errors; WC, waist circumference; FBG, fasting blood glucose; PSA, prostate-specific antigen.
*P-values were obtained by multiple linear regression analysis.
Table 5. Multiple regression analysis regarding the association be- tween PSA and other variables (n=268)
Variable β±SE P-value*
Age (y) 0.011±0.007 0.125
BMI (kg/m2) -0.059±0.019 0.002
Prostate volume (cc) 0.045±0.006 <0.001 PSA, prostate-specific antigen; β, regression coefficient; SE, standard errors; BMI, body mass index.
*P-values were obtained by multiple linear regression analysis.
Taek-Young Kim, et al. Association of Metabolic Factors with Prostate Volume and Prostate-Specific Antigen
Korean Journal of Family Practice
KJFP
되었으며 이 쥐들에게 남성호르몬을 다시 보충하였을 때 전립선이 다시 성장하였다는 결과19)와 사람을 대상으로 시행한 연구에서 남 성호르몬/여성호르몬 비의 감소로 인해 전립선비대증이 유발된다 는 연구 결과가 있었다.20) 마지막으로 고혈당증 및 고인슐린혈증과 관련된 만성적인 염증 상태가 전립선비대증에 기여할 수 있는데, 비 만 유발 당뇨병 쥐 연구에서 전립선 및 요도 조직의 섬유화와 배뇨 장애가 당뇨병 상태와 관련이 있음이 확인되었고,21) 사람의 전립선 절제 표본을 연구한 결과 대사증후군 인자가 염증성 조직학 점수와 단계적으로 연관되어 있음이 확인되었다.22)
위와 같이 대사증후군과 전립선비대증이 병태생리학적인 부분 에 있어서 유사한 부분이 있거나 같은 부분을 공유하고 있을 가능 성이 있다고 생각되고 있어, 많은 연구자들이 대사증후군 혹은 대사 인자들과 전립선비대증에 대한 여러 연구들을 시행하였다. 하지만 대사인자와 전립선비대증의 연관성에 대해서는 일관된 결론이 도 출되지 못하고 연구자들에 따라서 유사하거나 혹은 상반되는 다양 한 결과를 보였기에 본 연구와 비교해 보았다.
본 연구에서 41세에서 70세 남성 전체를 대상으로 한 분석에서 허 리둘레와 전립선 용적 간에 양의 상관관계가 있음이 확인되었다. 허 리둘레와 전립선 용적 간의 연관성은 다음과 같이 설명될 수 있다.
복부비만은 에스트로겐과 인슐린을 증가시키고, 성 호르몬 결합 글 로불린을 감소시킨다. 성 호르몬 결합 글로불린의 감소는 전립선세 포로 안드로겐과 에스트로겐의 진입을 증가시키고, 전립선세포 내 부로 진입한 안드로겐은 안드로겐 수용체와 결합하여 전립선을 증 식시킨다. 또한, 비만으로 인해 증가된 인슐린은 전립선의 증식에 중 요한 역할을 하는 인슐린유사성장인자-1 (IGF-1)의 수용체와 결합 하여 전립선의 증식에 관여한다.23) 이는 Nah 등24)의 허리둘레와 전립 선비대증과의 연관성에 대한 연구 결과와 일치 한다.
또한, 본 연구에서 전체를 대상으로 한 분석에서 공복혈당과 전립 선 용적 간에도 양의 상관관계가 있음이 확인되었다. 공복혈당과 전 립선 용적 간의 연관성은 인슐린 저항성으로 인한 고인슐린혈증으 로 설명할 수 있다.23) 인슐린은 인슐린유사성장인자-1 (IGF-1)과 구조 적으로 유사하기 때문에 인슐린유사성장인자-1 (IGF-1) 수용체와 결 합하여 전립선의 성장 및 증식을 유발할 수 있다.18) 또한, 고혈당증 및 고인슐린혈증과 관련된 만성적인 염증 상태가 전립선 세포의 성 장에 영향을 줄 수 있다.22,23) 이는 Yim 등1)의 공복혈당과 전립선비대 증의 연관성에 대한 연구 결과와도 일치한다.
마지막으로 본 연구에서는 체질량지수와 PSA가 음의 상관 관계 가 있음이 확인되었다. 전립선암 검진과 관련해서 PSA 수치를 해석 할 때 PSA 수치에 나이 외에도 비만이 영향을 줄 수 있다는 연구들 이 보고되고 있다. 체질량지수와 PSA 수치 간의 음의 상관관계가 보
고되고 있는데,25-27) 이는 비만인 전립선암 환자의 전립선암 진단이 지연될 수 있다는 가능성을 제시하고 있다. Banez 등25)의 체질량지 수, PSA 절대양, PSA 농도 수치를 비교한 후향적 코호트 연구에서는 체질량지수와 PSA 절대양의 상관관계는 확인되지 않으나 체질량지 수가 증가할수록 체내 혈장량의 증가가 확인되고 이로 인해 혈액희 석 효과가 생기기 때문에 PSA 농도 수치가 낮게 측정되는 것으로 설 명하였다. 이는 Ahn 등26)의 체질량지수와 PSA 수치의 연관성에 대 한 연구 결과와도 일치한다.
기타 다른 연구들을 좀 더 보면, Kim 등28)은 대사증후군에 부합 하는 실험군이 대조군에 비해 전립선 용적이 유의하게 증가되어 있 다고 보고하였다. 그리고 Hammarsten과 Högstedt29)은 고밀도 콜레 스테롤 수치가 낮거나 중성지방 수치가 높을수록 전립선 용적이 증 가한다고 보고하였다. 그러나 본 연구에서는 고밀도 콜레스테롤 수 치 및 중성지방과 전립선 용적 간의 연관성이 보이지 않았다. 그리고 대사증후군이 진단된 군에서 유의하게 전립선 용적이 증가되어 있 지는 않았다. 이는 Gupta 등30)이 전립선비대증이 대사증후군, 체질 량지수 및 혈중 지질 수치와 관련이 없다고 보고한 연구 결과와 일치 한다.
본 연구를 통해서 허리둘레 및 공복혈당과 전립선 용적의 연관성 을 확인하였으며 체질량지수와 PSA 수치 간의 연관성을 확인할 수 있었다. 그러나 대사적 요소가 전립선 용적 및 PSA 수치에 미치는 영 향성을 후향적 단면연구를 통해 확인하는 것에는 제한이 있으며 연 구 표본의 수가 적고 특히 허리둘레 계측자가 적어 대사증후군과의 연관성을 평가하는 것에도 한계가 있다. 또한, 인슐린 저항성을 좀 더 정확히 대변할 수 있는 혈액검사를 시행하지 못하였으며 생활습 관 관련 변수에 대한 고려를 하지 못한 점이 제한점이다. 그리고 일 개 병원 건강검진 수진자를 대상으로 한 연구 결과를 전체 인구집단 에 일반화하는 것에도 한계가 있다. 추후 대사적 요소와 전립선 용 적 및 PSA 수치의 연관성 및 선후관계를 더욱 정확히 평가하기 위해 서는 대규모의 전향적 연구가 필요할 것으로 사료된다. 또한 대사적 요소의 개선이 전립선 비대증의 예방 및 치료에 효과가 있을지에 대 한 연구도 시행돼야만 한다고 생각한다.
요 약
연구배경:
한국 성인 남성에서 대사적 요소와 전립선 용적 및 전립 선 특이항원의 연관성을 평가하기 위하여 수행되었다.방법:
2011년 1월부터 2015년 12월까지 대전보훈병원에 내원하여 종 합건강검진을 시행 받은 대상자 중 전립선 비대증, 전립선염이나 전 립선암 등의 전립선 관련 질환을 진단받은 환자를 제외하고 268명김택영 외. 전립선 용적 및 전립선 특이항원과 대사적 요소의 연관성 Korean Journal of Family Practice
KJFP
을 선별하여 후향적 연구를 시행하였다. 신장, 체중, 허리둘레, 체질 량지수, 수축기 및 이완기 혈압의 신체 계측 결과와 공복혈당, 총콜 레스테롤, HDL, LDL, 중성지방, AST, ALT, GGT의 혈액화학검사 수 치를 independent-samples t-test와 Pearson’s correlation test, 다중회귀 분석을 이용하여 전립선 용적 및 전립선 특이항원과의 연관성을 분 석하였다. 또한, 2009년 IDF와 AHA/NHLBI의 합동 선언에서 제시한 대사증후군 진단 기준과 전립선 용적 및 전립선 특이항원과의 연관 성을 분석하였고, 대사증후군과 전립선 용적 및 전립선 특이항원과 의 연관성도 분석하였다.
결과:
허리둘레(P<0.05)와 공복혈당(β±SE=0.051±0.018, P<0.01)이 증 가할수록 전립선 용적이 통계적으로 유의하게 증가하였다. 또한, 체 질량지수가 증가할수록 전립선 특이항원 수치가 통계적으로 유의 하게 감소하였다(β±SE=-0.059±0.019, P<0.01). 그러나 대사증후군의 유병 여부와 전립선 용적과 전립선 특이항원 수치는 통계적으로 유 의한 연관성이 없는 것으로 확인되었다.결론:
한국 성인 남성에서 허리둘레와 공복혈당은 전립선 용적과 양의 상관관계가 있고 체질량지수와 전립선 특이항원 수치는 음의 상관관계가 있다.중심단어:
전립선 용적; 전립선 특이항원; 허리둘레; 공복혈당; 체질 량지수; 대사증후군REFERENCES
1. Yim SJ, Cho YS, Joo KJ. Relationship between metabolic syndrome and prostate volume in Korean men under 50 years of age. Korean J Urol 2011;
52: 390-5.
2. Nandeesha H, Koner BC, Dorairajan LN, Sen SK. Hyperinsulinemia and dyslipidemia in non-diabetic benign prostatic hyperplasia. Clin Chim Acta 2006; 370: 89-93.
3. The Korean Urological Association. The textbook of urology. 4th ed. Seoul:
Ilchokak; 2007.
4. Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human be- nign prostatic hyperplasia with age. J Urol 1984; 132: 474-9.
5. Emberton M, Andriole GL, de la Rosette J, Djavan B, Hoefner K, Vela Na- varrete R, et al. Benign prostatic hyperplasia: a progressive disease of aging men. Urology 2003; 61: 267-73.
6. Marberger MJ, Andersen JT, Nickel JC, Malice MP, Gabriel M, Pappas F, et al.
Prostate volume and serum prostate-specific antigen as predictors of acute urinary retention. Combined experience from three large multinational placebo-controlled trials. Eur Urol 2000; 38: 563-8.
7. Lieber MM, Jacobsen SJ, Roberts RO, Rhodes T, Girman CJ. Prostate volume and prostate-specific antigen in the absence of prostate cancer: a review of the relationship and prediction of long-term outcomes. Prostate 2001; 49:
208-12.
8. Lee C, Kozlowski JM, Grayhack JT. Etiology of benign prostatic hyperplasia.
Urol Clin North Am 1995; 22: 237-46.
9. Qu X, Huang Z, Meng X, Zhang X, Dong L, Zhao X. Prostate volume corre- lates with diabetes in elderly benign prostatic hyperplasia patients. Int Urol Nephrol 2014; 46: 499-504.
10. Wallner LP, Hollingsworth JM, Dunn RL, Kim C, Herman WH, Sarma AV.
Hyperglycemia, hyperinsulinemia, insulin resistance, and the risk of BPH/
LUTS severity and progression over time in community dwelling black men: the Flint men’s health study. Urology 2013; 82: 881-6.
11. Aarnink RG, de la Rosette JJ, Debruyne FM, Wijkstra H. Formula-derived prostate volume determination. Eur Urol 1996; 29: 399-402.
12. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and preven- tion; national heart, lung, and blood institute; American heart association;
world heart federation; international atherosclerosis society; and interna- tional association for the study of obesity. Circulation 2009; 120: 1640-5.
13. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract 2007; 75: 72-80.
14. Hedblad B, Nilsson P, Engström G, Berglund G, Janzon L. Insulin resistance in non-diabetic subjects is associated with increased incidence of myocar- dial infarction and death. Diabet Med 2002; 19: 470-5.
15. Reaven GM. Banting lecture 1988. Role of insulin resistance in human dis- ease. Diabetes 1988; 37: 1595-607.
16. Kim C, Halter JB. Endogenous sex hormones, metabolic syndrome, and dia- betes in men and women. Curr Cardiol Rep 2014; 16: 467.
17. Oelke M, Kirschner-Hermanns R, Thiruchelvam N, Heesakkers J. Can we identify men who will have complications from benign prostatic obstruc- tion (BPO)? ICI-RS 2011. Neurourol Urodyn 2012; 31: 322-6.
18. Sarma AV, Kellogg Parsons J. Diabetes and benign prostatic hyperplasia:
emerging clinical connections. Curr Urol Rep 2009; 10: 267-75.
19. Timme TL, Truong LD, Merz VW, Krebs T, Kadmon D, Flanders KC, et al.
Mesenchymal-epithelial interactions and transforming growth factor-beta expression during mouse prostate morphogenesis. Endocrinology 1994;
134: 1039-45.
20. Brochu M, Bélanger A. Comparative study of plasma steroid and steroid glucuronide levels in normal men and in men with benign prostatic hyper- plasia. Prostate 1987; 11: 33-40.
21. Gharaee-Kermani M, Rodriguez-Nieves JA, Mehra R, Vezina CA, Sarma AV, Macoska JA. Obesity-induced diabetes and lower urinary tract fibrosis promote urinary voiding dysfunction in a mouse model. Prostate 2013; 73:
1123-33.
22. Vignozzi L, Gacci M, Cellai I, Santi R, Corona G, Morelli A, et al. Fat boosts, while androgen receptor activation counteracts, BPH-associated prostate inflammation. Prostate 2013; 73: 789-800.
23. Dahle SE, Chokkalingam AP, Gao YT, Deng J, Stanczyk FZ, Hsing AW. Body size and serum levels of insulin and leptin in relation to the risk of benign prostatic hyperplasia. J Urol 2002; 168: 599-604.
24. Nah EH, Cho HI, Choi JC. Association of metabolic factors and prostate- specific antigen levels with prostate volume in medical check-ups. Lab Med Online 2014; 4: 212-7.
25. Bañez LL, Hamilton RJ, Partin AW, Vollmer RT, Sun L, Rodriguez C, et al.
Obesity-related plasma hemodilution and PSA concentration among men
Taek-Young Kim, et al. Association of Metabolic Factors with Prostate Volume and Prostate-Specific Antigen
Korean Journal of Family Practice
KJFP
with prostate cancer. JAMA 2007; 298: 2275-80.
26. Ahn SC, Shim SJ, Choi KE, Song IC, Kang DW, Kwon SR. Association of metabolic syndrome with prostate-specific antigen. Korean J Fam Pract 2015; 5(Suppl 3): S315-20.
27. Kubota Y, Seike K, Maeda S, Shinohara Y, Iwata M, Sugimoto N. Relation- ship between prostate-specific antigen and obesity in prostate cancer screening: analysis of a large cohort in Japan. Int J Urol 2011; 18: 72-5.
28. Kim JH, Shim BS, Kim JS, Hong YS. Voiding dysfunction of men is associat- ed with metabolic syndrome. Korean J Urol 2006; 47: 257-62.
29. Hammarsten J, Högstedt B. Hyperinsulinaemia as a risk factor for develop- ing benign prostatic hyperplasia. Eur Urol 2001; 39: 151-8.
30. Gupta A, Gupta S, Pavuk M, Roehrborn CG. Anthropometric and metabol- ic factors and risk of benign prostatic hyperplasia: a prospective cohort study of Air Force veterans. Urology 2006; 68: 1198-205.