- 121 -
Incidence and Types of Sphenoethmoid Cell in Patients with Chronic Paranasal Sinusitis
Seung-Kyu Chung, M.D., Hyo Yeol Kim, M.D. and Seong-Won Yoon, M.D.
ABSTRACT
The sphenoethmoid cell is the most posterior ethmoid cell, pneumatizing far laterally and to some degree superiorly to the sphenoid sinus. A accurate understanding of the sphenoethmoid cell is important for avoiding fatal injury to the orbit and safely approaching the sphenoid sinus. To investigate the incidence of sphenoethmoid cells, the authors analyzed the coronal CT scans of 50 patients who underwent endoscopic sinus surgery for sinusitis. Sphenoethmoid cells were identified in 39 out of 100 nasal cavities and divided into two types according to their relationship with the optic canal and the sphenoid sinus:type 1 cells, where the optic nerve bordered the sphenoethmoid cell and the sphenoid sinus, were observed in 14 cavities, and type 2 cells, where the optic nerve bordered only the sphenoethmoid cell, were observed in 25 cavities. We anticipate the existence of an optic canal in the posterior ethmoid sinus in one third of the cases, and the direction of the approach to the anterior wall of the sphenoid sinus should be modified according to the type of sphenoethmoid cell if one is present.
KEY WORDS:Sphenoethmoid cell·Onodi cell·PACS.
INTRODUCTION
Damage to the optic nerve, which is located in the superol- ateral portion of the sphenoid and posterior ethmoid sinuses, is a serious complication of intranasal sinus surgery. The sph- enoethmoid or Onodi cell is the most posterior of the posterior ethmoid cells, pneumatizing far laterally and to some degree superiorly to the sphenoid sinus. Depending on the degree of the pneumatization, the optic nerve canal and the carotid artery may in some cases bulge into the sphenoethmoid cell;that is, the optic canal may be found not only in the sphenoid sinus but also in the sphenoethmoid cell. In the presence of a sphenoet- hmoid cell, therefore, great care should be taken during surgery not to injure the optic nerve or carotid artery in the posterola- teral part of the posterior ethmoid cell. Careful interpretation of CT scans before the operation may help to prevent fatal da- mage to the optic nerve during sinus surgery.
In cadaver dissection studies, the incidence of sphenoeth-
moid cells has been found to vary between 12-51%.1-4) In pa- tients with chronic inflammation of the paranasal sinuses, the sphenoethmoid cell is reported to be present in about 13% of cases.5) In the study of 150 cases of paranasal sinusitis, De- Lano et al.6) found the optic nerve to be contiguous with the posterior ethmoid sinus in only 3% of cases. As can be obs- erved, the reported range of sphenoethmoid cell’s prevalence is very wide. Furthermore, there have been no reports on the prevalence of sphenoethmoid cells in Asian patients with ch- ronic paranasal sinusitis. Driben et al. report that a CT was not able to identify the presence of the sphenoethmoid cell reliably in comparison to anatomic dissection.3) Driben’s study, however, used two window settings for a CT reading, which might have resulted in imprecise observation of the anterior sphenoid wall. The authors believe the low detection rate may be improved with a picture archiving and communication sy- stem (PACS).
In this study, the authors investigated the incidence of sp- henoethmoid cells invading the sphenoid sinus and classified these cells according to their relationship with the course of the optic nerve. To examine the relationship of the optic canal with the sphenoid and posterior ethmoid sinuses, the study used high-resolution CT with a PACS.
MATERIALS AND METHODS
Direct coronal sinus CT scans of 50 consecutive patients with chronic inflammatory sinus disease, taken from October Department of Otorhinolaryngology, Head and Neck Surgery,
College of Medicine, Sungkyunkwan University, Samsung Me- dical Center, Seoul, Korea
Address correspondences and reprint requests to Seung-Kyu Chung, M.D., Department of Otorhinolaryngology, Head and Neck Surgery, College of Medicine, Sungkyunkwan University, Samsung Medical Center, 50 Ilwondong, Kangnamku, Seoul 135- 710, Korea
Tel:82-2-3410-3572, Fax:82-2-3410-3879 E-mail:[email protected] Accepted for publication on October 8, 1998
1996 to January 1997, were reviewed. The patient population included 14 females and 36 males, whose ages ranged from 11 to 72 years (mean 39.54 years). Patients whose anatomic structures around the posterior ethmoid sinus area were dest- royed due to previous surgery were excluded from this study.
Patients younger than 10 years old or with bony diseases were also excluded.
The scans were performed by a General Electric 9800 sy- stem (General Electric Corporation 240 high-speed advantage system, 120 kv, 100 mA, Milwaukee, USA) on continuous thin section slices in the coronal plane. Scan section widths were 3 mm. Preoperative coronal CT scans of the patients with ch- ronic paranasal sinusitis were reviewed with a PACS at Sam- sung Medical Center. The PACS enables easy adjustment of the window width and level of the CT image and easy mag- nification of the image.
The right and left sides were considered separately, and a total of 100 sinus-to-optic canal relationships were analyzed.
The direct relationships between the optic canal, the posterior ethmoid and the sphenoid sinuses were recorded.
Posterior ethmoid cell pneumatization was classified as no- rmal if the posterior cells were confined within the usual pos- terior limits of the ethmoid labyrinth;they were categorized as sphenoethmoid cells if they extended posteriorly over the sphenoid sinus.
Sphenoethmoid cells were classified into one of two types according to the relationship of the posterior ethmoid cell, the
sphenoid cell and the course of the optic nerve:type 1, if the optic nerve was contiguous with both the sphenoethmoid cell and the sphenoid sinus, or type 2, if the optic nerve was cont- iguous only with the sphenoethmoid cell.
We also recorded the incidence of optic nerves that bulged into a sinus more than half the circumference of the optic nerve.
RESULTS
The posterior ethmoid cells remained within the usual limits of the ethmoid labyrinth in 61% of the 100 nasal cavities, and the optic nerve was adjacent to the sphenoid sinus in these patients. In 39% of the cavities studied, the posterior ethmoid
Fig. 2. A:No sphenoethmoid cell on the right side and type 2 sphenoethmoid cell on the left side. On this series of coronal CT scans (1-4, from anterior to posterior), the left posterior ethmoid cell extends posteriorly and touches the optic canal, and the left sphenoid sinus does not meet the optic nerve. B:Postoperative state of the left posterior ethmoid and the sphenoid sinus. The optic nerve is observed only in the posterior ethmoid sinus, and the sphenoid sinus is below the optic nerve canal. S:sphenoid sinus, P:posterior ethmoid cell, Arrow:optic nerve canal.
Fig. 1. Incidence of the sphenoethmoid cell.
A AA
A BBBB
1 1 1
1 2222
33
33 4444
cells pneumatized over the ipsilateral sphenoid sinuses, and either the posterior ethmoid cell or the sphenoid sinus was co- ntacted by the ipsilateral optic canal. Fourteen cavities (14%) indicated a type 1 sphenoethmoid cell, and 25 cavities (25%) indicated a type 2 sphenoethmoid cell (Figs. 1, 2 and 3).
Optic nerves that bulged into a sinus more than half the circumference of the optic nerve were noted in 11 cavities (11%) (Fig. 4). Of these 11, sphenoethmoid cells were pre- sent in 9 cavities.
DISCUSSION
It is important that rhinologists performing sinus surgery, transseptal transsphenoidal pituitary operations or transnasal endoscopic optic nerve decompression have a clear understa- nding of the anatomic relationships that exist between poste- rior ethmoid cells, the sphenoid sinus, and their neighboring structures.
Improvements in CT imaging and past successes with end- oscopy have encouraged surgeons to enter the sphenoid sinus whenever necessary. The sphenoid sinus is intimately related to the optic nerve, but the relationship is variable due in part to the varying degrees of sphenoid sinus pneumatization and the varying extent to which the posterior ethmoid cell extends back into the sphenoid sinus. Cheung et al have found some skull specimens to contain posterior ethmoid cells reaching all the way to the sella.7)
Although the relationship between the optic nerve, the sp- henoid sinus and the posterior ethmoid sinus has been invest- igated, the prevalence of sphenoethmoid cell varies considerably among studies. In most of the studies, a sphenoethmoid or Onodi cell is defined as an optic nerve bulging into an ext-
Fig. 3. A:Type 2 sphenoethmoid cell on the right side and type 1 sphenoethmoid cell on the left side. Coronal CT scans show the left optic nerve to be in contact with the posterior ethmoid sinus at its junction with the sphenoid sinus. B, C:Postoperative featu- res of the posterior ethmoid cells and the sphenoid cells of the right (B) and left (C) sides. On the left side, the optic nerve canal crosses over the septum between the sphenoid sinus and poste- rior ethmoid sinus. S:sphenoid sinus, P:posterior ethmoid sinus, Arrow:optic nerve canal.
A AA
A BBBB
ccc c
1 1 1
1 2222
3 3 3
3 4444
ensively pneumatized posterior ethmoid. The incidence of sp- henoethmoid cells in cadaver dissection ranges between 9%
and 51%.1-4)8) Sphenoethmoid cells were found in 10% of cases in gross anatomic studies.8) In studies where the prevalence exceeded 35%, the anatomic dissection had been done with a microscope, a loupe or an endoscope.2-4) That the incidence of sphenoethmoid cell varies so widely across the literature can be attributed to the fact that definitions and interpretations of the local anatomy are inconsistent from study to study.
The incidence of sphenoethmoid cell has also been investi- gated with CT scanning. Bansberg et al studied the CT scans of 80 patients indicating no inflammation of the sinuses. In 8% of these cases the posterior ethmoid cells extended into the ipsilateral sphenoid sinus and contacted the ipsilateral op- tic nerve.9) In studies of CT scans of patients with chronic inflammatory sinus disease, the incidence of sphenoethmoid cell ranges between 3% and 12%.5)6) The detection rate of the sphenoethmoid cell with CT appears to be lower than with cadaver dissection. In the present study, the incidence of sph- enoethmoid cell was 39%, higher than other studies with CT scanning and similar to studies with cadaver dissection.
According to Driben et al.,3) the fact that CT studies and cadaver dissections yield different incidences of sphenoethmoid cell can be attributed to limitations of the current CT scanning protocol. However, there are also difficulties related to how a sphenoethmoid cell is defined. One condition that defines the sphenoethmoid cell is a posterior ethmoid cell that pneumatizes into the sphenoid sinus. With CT scanning at the normal sett- ings, the wall that separates the ethmoid sinus from the sph- enoid sinus is not well visualized due to the fact that this wall is located in the coronal plane. To properly observe the anterior wall of the sphenoid sinus, the window settings of the CT scan must be adjusted. With PACS, which allows easy adjustment of the window settings, the chance of observing the anterior wall of the sphenoid sinus increases. In this study, the wall us- ually became visible when the level of the window setting was lowered. Another condition is bulging of the optic nerve. There are no definite criteria for this definition. Whether or not the optic nerve appears to bulge is open to the discretion of the observer. Because the optic nerve runs in the medial posterior direction from the globe, bulging of the nerve becomes less apparent with a coronal or axial section of a CT scan. The bu- lging becomes much less apparent with thick section thickness.
Many surgeons consider it important to understand the rel- ationship between the optic nerve and surrounding sinuses for avoiding injury of the nerve.10)11) Kainz and Stammberger fo- und dehiscence in the bony wall of the optic canal in 12% of the cases they studied.2) After conducting CT studies, Bansberg et al. reported that the posterior ethmoid air cells were observed to be in contact with the ipsilateral optic canals in all cases involving sphenoethmoid cells, in 43% of cases with normal posterior ethmoid cells and in 48 % of the total cases they st- udied.9) A study by DeLano et al. reports on the relationship found between the optic nerve and the posterior ethmoid sin- uses in the CT scans of 150 patients with chronic inflammatory sinus disease:6) they found the optic nerves to be in contact with the posterior ethmoid sinus in only 3% of cases.
With regard to the protrusion of the optic nerve into the posterior ethmoid cells or the sphenoid sinus, the reported in- cidence ranges from 2% to 24%.1)5)6)12) With protrusion defined
Fig. 4. Bulging of the optic nerve canal into the cavity of the left posterior ethmoid sinus to a degree more than half the cir- cumference of the nerve was seen in left side. Bony dehiscence of the canal is observed (white arrow). S:sphenoid sinus, P:
posterior ethmoid sinus, Arrow:optic nerve canal.
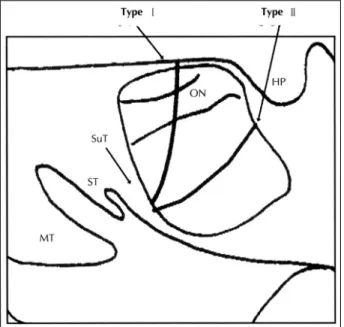
Fig. 5. Direction of the approach to the septum between the posterior ethmoid cell and the sphenoid sinus. The choice of instrument should depend on the type of sphenoethmoid cell.
MT:middle turbinate, ST:superior turbinate, SuT:supreme tu- rbinate, ON:optic nerve, HP:hypophysis.
as bulging of the optic canal into the cavity of the sinus to a degree that exposes more than half the circumference of the nerve, Dessi et al. reported no bulging into the posterior et- hmoid cells and bulging of the optic nerve into the sphenoid sinus in 8% of axial and coronal scans.12) Based on the same definition, the authors of this study found bulging of the optic nerve into the posterior ethmoid sinus or sphenoid sinus in 11%
of the cases under observation;bulging of the optic nerve was observed in 23% of cases involving a sphenoethmoid cell.
DeLano et al. classified the relationship into four categories, and found that the optic nerve coursed adjacent to the sphenoid sinus without indentation in 76% of cases.6) That is, the prev- alence of optic nerve indentation was higher than what has been found in other reports. These findings indicate that not all optic nerves make indentations into the posterior ethmoid cell or the sphenoid sinus.
The authors of this study also encountered many cases of endoscopic sinus surgery in which the optic nerve did not bu- lge into the ethmoid sinus or the sphenoid sinus. Bulging of the optic nerve is usually required for defining a Onodi cell, and the above studies do not mention cases in which the po- sterior ethmoid sinus pneumatized over the sphenoid sinus without indentation of the optic nerve into the ethmoid cell.
This may be another reason for the varying prevalence of sp- henoethmoid cell. In the present study, the authors classified sphenoethmoid cells into one of two types according to the degree of pneumatization over the sphenoid sinus, regardless of whether or not there was bulging of the optic nerve. In the case of a type 1 sphenoethmoid cell, the anterior sphenoid wall met the optic canal. In the case of a type 2 sphenoethmoid cell, the course of the optic nerve remained entirely within the posterior ethmoid cell.
The approaches of choice to the sphenoid sinus are through the ethmoidectomized cavity or through the space between the septum and turbinates.13) Widening the natural opening of the sphenoid sinus by removing the septum that separates the sphenoid sinus from the posterior ethmoid sinus is a safe me- thod. The direction of the endoscope in relation to the position of the septum depends on the extent of the pneumatization of the sphenoethmoid cell.3) The anterior wall of the sphenoid sinus thus may not present in the coronal plane, but run from anteromedially to posterolaterally. It could prove to be a seri- ous mistake to follow the lamina papyracea posterolaterally when looking for the sphenoid sinus behind a sphenoethmoid cell.2) When the overriding of the posterior ethmoid cell over
the sphenoid cell is little or none, the plane of the septum is perpendicular to the direction of the endoscope and the septum can be removed easily with upward cutting forceps. When a type 2 sphenoethmoid cell is encountered, the plane of the septum is parallel to the direction of the endoscope and strai- ght cutting forceps are required (Fig. 5).
CONCLUSION
Sphenoethmoid cells were noted in 39% of the cases exa- mined in the present study. Once found present, the type of the sphenoethmoid cell should determine the direction of the approach to the septum between the posterior ethmoid cell and the sphenoid sinus and the choice of instrument.
REFERENCES
1) Sethi DS, Stanley RE, Pillay PK. Endoscopic anatomy of the sp- henoid sinus and sella turcica. J Laryngol Otol 1995;109:951-5.
2) Kainz J, Stammberg H. Danger areas of the posterior rhino-basis:
An endoscopic and anatomical-surgical study. Acta Otolaryngol 1992;112:852-61.
3) Driben JS, Bolger WE, Robles HA, Cable B, Zinreich SJ. The rel- iability of computerized tomographic detection of the Onodi (sp- henoethmoid) cell. Am J Rhinol 1998;12:105-11.
4) Yoeh KH, Tan KK. The optic nerve in the posterior ethmoid in As- ians. Acta Otolaryngol (Stoch) 1994;114:329-36.
5) Meloni F, Mini R, Rovasio S, Stomeo F, Teatini GP. Anatomic va- riations of surgical importance in ethmoid labyrinth and sphenoid sinus. A study of radiological anatomy. Surg Radiol Anat 1992;
14:65-70.
6) DeLano MC, Fun FY, Zinreich SJ. Relationship of the optic nerve to the posterior paranasal sinuses: A CT anatomic study. Am J Ne- uroradiol 1996;17:669-75.
7) Cheung DK, Martin GF, Rees J. Surgical approach to the sphenoid sinus. J Otolaryngol 1992;21:1-8.
8) Lang J. Clinical anatomy of the nose, nasal cavity and paranasal sinuses. New York: Thieme Medical Publishers Inc;1989. p.85-98.
9) Bansberg SF, Harner SG, Forbes G. Relationship of the optic ne- rve to the paranasal sinuses as shown by computed tomography.
Otolaryngol Head Neck Surg 1987;96:331-5.
10) Maniglia AJ. Fatal and other major complications of endoscopic sinus surgery. Laryngoscope 1991;101:349-54.
11) Rauchfuss A. Komplikationen der endonasalen Chirurgie der Na- sennebenhohlen. Spezielle Anatomie, Pathomechanismen, operat- ive Versorgung. HNO 1990;38:309-17.
12) Dessi P, Moulin G, Castro F. Protrusion of the optic nerve into the ethmoid and sphenoid sinus: Prospective study of 150 CT studies.
Neuroradiol 1994;36:515-6.
13) Metson R, Gliklich RE. Endoscopic treatment of sphenoid sinusitis.
Otolaryngol Head Neck Surg 1996;114:736-44.