- 53 -
Treatment Outcomes of Endoscopic Endonasal Dacryocystorhinostomy
Hyuk Kim, M.D.
2, Jae-Ho Kim, M.D.
1and Bong-Jae Lee, M.D.
1 ABSTRACTEndoscopic dacryocystorhinostomy represents a new and promising approach to removing obstruction of the lacrimal pathways without incising the skin. In this study, the authors aimed to evaluate the efficacy of endoscopic endonasal dacryocystorhinostomy in relation with several other methods of lacrimal bone removal, including the gouge and mallet method, used to treat nasolacrimal duct obstruction. Under review were the medical records of fourteen patients (13 males, one female) undergoing 16 endoscopic dacryocystorhinostomy procedures, of which 14 were primary and two were revision cases. Patients were followed up for 6- 52 months (mean:27 months). Endoscopic dacryocystorhinostomy was successful in 92.9% (13/14) of primary cases and 100% (2/2) of revision cases. Minor postoperative complications, such as synechia and granulation tissue formation, developed in four cases, but were successfully treated. Using the septal gouge and mallet method, we were able to easily remove the bony covering of the lacrimal sac. Our study indicates the efficacy of endoscopic dacryocystorhinostomy to be comparable to that of external approaches.
KEY WORDS:Endoscopic dacryocystorhinostomy・Treatment outcome・Gouge and mallet.
INTRODUCTION
For the treatment of epiphora and chronic dacryocy- stitis caused mainly by nasolacrimal duct obstruction, the probing method, balloon dilatation, stent insertion, ext- ernal dacryocystorhinostomy and endonasal dacryocys- torhinostomy are widely used. Recent developments in endoscopic surgery has allowed unprecedented access to the inside of the nasal cavities, facilitating operations around the lacrimal sac and paving the way for endosc- opic endonasal dacryocystorhinostomy, a new method of treating nasolacrimal duct obstruction. We studied the treatment outcomes of 16 cases, in which the patients, upon visiting the hospital complaining mainly of epip- hora, were diagnosed with nasolacrimal duct obstruction
and subsequently treated with endonasal dacryocystor- hinostomy. We also evaluated the effectiveness of the operating method that, with the use of a gouge and ma- llet, was performed to remove the lacrimal bone.
MATERIALS AND METHODS Materials
Out of 16 patients who visited the otorhinolaryngol- ogy department of Asan Medical Center from September 1993 to September 1997 complaining of epiphora, 14 patients were diagnosed with nasolacrimal duct obstru- ction after a dacryocystogram and subsequently treated with endonasal dacryocystorhinostomy. Of these 14 pa- tients, 13 were male and one was female, with ages ra- nging from from six to 72 years (Table 1). Of the 16 cases, 14 were primary cases and two were revision cases, of which one was a case of recurrence following a primary operation and the other involved a case of revision due to continuing epiphora following external dacryocysto- rhinostomy in the department of ophthalmology. Follow- up periods in the primary cases ranged from six months to 52 months with an average of 27 months, while the period of follow-up in the two revision cases were 12
1Department of Otolaryngology, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, 2Department of Oto- laryngology, Myongji Hospital, College of Medicine, University of Kwandong, Goyang, Korea
Address correspondence and reprint requests to Jae-Ho Kim, M.D., Department of Otolaryngology, College of Medicine, Ul- san University, Asan Medical Center, 388-1 Poongnapdong, Sonpagu, Seoul 138-736, Korea
Tel:82-2-2224-3710, Fax:82-2-489-2773 E-mail:[email protected] Accepted for publication on March 10, 1999
months and 34 months, respectively.
Methods
After administering general (12 cases) or local (four cases) anesthesia to the patients, we anesthetized the nasal mucosa with a gauze containing 4% lidocaine and 0.1% epinephrine. A mixture of 1% lidocaine and epin- ephrine (1:200,000) was then injected for vasoconstr- iction and mucosal anesthesia. The conjunctiva was also anesthetized, with 0.5% pontocaine, and the inferior canaliculus was expanded by using a puncture dilator and inserting a 20-gauge endoilluminator into the lacr- imal sac. By using a 25° endoscope (Wolf, Illinois, USA), we were able to locate the lacrimal sac and, with a sic-
kle knife and Weil-Blakesley forceps, remove a 15×20 mm portion of the mucosa. In eight cases, the inferior bony wall of the lacrimal sac was removed via the septal gouge and mallet method (Fig. 1). In the remaining eight cases, an approximately 8×12 mm portion of the lacri- mal bone was removed by using curettes, Kerison bone punch forceps or diamond drills. The septal gouges we used had a semi-circular edge, and the gouge was placed on the frontal side of the agger nasi cell under the endo- scope. With a mallet, we struck the lacrimal bone forming the external area of the lacrimal sac in an outsideto- inside direction. We then struck the upper part of the lacrimal sac several times with the mallet in an upside- to-downside direction to make a clean removal of bony fragment and expose the interior wall of the lacrimal sac.
The exposed mucosa of the lacrimal sac was incised us- ing Nd-YAG lasers (15 watt, continuous mode) (six ca- ses) or sickle knives and removed with Gruenwaldt’s cutting forceps, making the diameter of the ostium about 5-7 mm. A Crawford-style bicanalicular silastic stent was inserted into the nasal cavities through the superior canaliculus and inferior canaliculus to form knots (15 times) measuring about 10 mm into the nasal cavities and the area was packed with gauze or Merocel (Xomed, Jacksonville, USA).
Postoperative treatment
The nasal packs were removed one or two days after the operation, at which time secretions and crust around the surgical site were also removed. To prevent crust fo- rmation, the area was rinsed with saline solution two times a day for four weeks and oral antibiotics were admini- stered for one to two weeks after the operation. Silicon stents were maintained for four to twelve weeks depen- ding on the condition of the case.
Assessment of surgical outcomes
Success of the operation was based on the post-ope- rative status of the epiphora and dacryocystitis, and the patency of the nasal cavity opening upon examination with an endoscope.
RESULTS
In the 16 cases under study, the single most frequent
Table 1. Age distribution of patients (N=14)
Age Number of patients
0-10 2 11-20 1 21-30 2 31-40 4 41-50 1 51-60 2 61-70 1 71-80 1
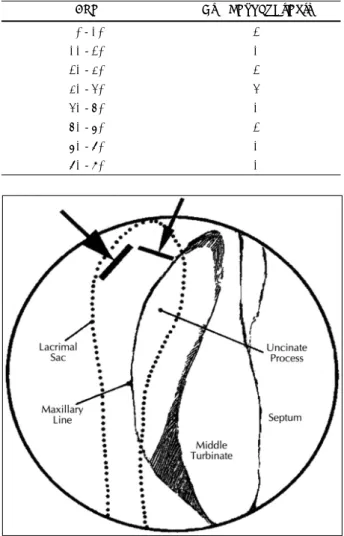
Fig. 1. Septal gouge and mallet method. Solid line shows the po- sition of gouge. Thick arrow shows the force direction (lateral to medial) of mallet in lateral portion of lacrimal sac. Thin arrow shows the direction (superior to inferior) of mallet in superior portion of the lacrimal sac.
cause of the nasolacrimal duct obstruction was trauma (eight cases). The other causes were postoperative com- plication (six cases), a medial maxillectomy (four cases), endoscopic sinus surgery (one case), a Caldwell-Luc operation (one case), chronic dacryocystitis (one case) and congenital factor (one case) (Table 2). In the case involving congenital factor, we conducted the operation on only one side, since the nasolacrimal duct obstruction was caused by the absence of both superior canaliculus.
Out of the 14 primary cases, 13 cases (92.9%) were tr- eated successfully, while one case (7.1%) required rev- ision due to continued epiphora with synechia. Both cases involving revision were treated successfully (Table 3).
Two out of the 16 cases involved simultaneous operati- ons:one case included a septorhinoplasty, conducted to treat deformity of the external nose and septum due to trauma, and the other case included endoscopic sinus surgery, performed to treat chronic sinusitis. Postopera- tive complaints included synechia of the nasal mucosa (two cases), granulation tissue (one case), and synechia and granulation tissue (one case) (Table 4). Of these, three cases were treated with endoscopic granulation tissue removal and short-term treatment with a steroid, while one case underwent reoperation due to nasolacrimal duct obstruction caused by synechia. There was no relation- ship between treatment results and whether or not laser was used, although one out of the six cases treated with laser demonstrated recurrence due to synechia while an- other one exhibited granulation tissue formation.
DISCUSSION
Nasolacrimal duct obstruction may be treated with non-
operative methods, such as the probing method and ba- lloon dilatation, or with operative methods, such as ext- ernal dacryocystorhinostomy and endoscopic endonasal dacryocystorhinostomy. The probing method is effective only for patients younger than one year and whose obs- truction is congenital.1) The main advantage of the bal- loon dilatation procedure is ease of operation, but the method has a low success rate in cases of epiphora inv- olving complete obstruction.2) The external dacryocys- torhinostomy approach has a reported success rate of about 90%,3) but is associated with many disadvantages, including operative difficulties, a complicated procedure and some scarring of the face. Since McDonogh and Me- iring’s report,4) endoscopic endonasal dacryocystorhin- ostomy has become more widely used. The procedure renders skin incision unnecessary and leaves no scarring of the face. In addition, there is no objection to pumping work of the orbicularis oculi.5) The method allows vie- wing of such nasal cavity lesions such as middle turbinate hypertrophy, chronic sinusitis, and fibrosis of the nasal cavities caused by past operations and synechia, that were the two main reasons of external dacryocystorhinostomy failure.6) A final advantage of endoscopic endonasal da- cryocystorhinostomy is that the procedure is easy to re- peat as needed.7)
We conducted endoscopic sinus surgery simultaene- ously in one case to treat accompanying chronic sinu- sitis. During the operation, we experienced difficulty in removing the medial bony wall in the lacrimal sac. After trying several approaches, we found a method using a septal gouge and a mallet, a technique we had designed, to be most effective. When using a drill, it is difficult to remove the side walls completely and dust from the bone hinders vision through the endoscope. Using a drill also takes a long time. A curette is difficult to use when re- moving side walls and often damages surrounding mu- cosa. Using septal gouges and a mallet to remove the medial bony walls saves time and enables complete re- moval of the bony fragment around the lacrimal sac. But
Table 2. Etiologies of the nasolacrimal duct obstruction (N=16) Etiology Number of cases
Trauma 8 Postoperative complication 6
Medial maxillectomy (n=4) Endoscopic sinus surgery (n=1) Caldwell-Luc operation (n=1)
Chronic dacryocystitis 1
Congenital 1
Table 3. Treatment outcomes
Success Failure Total Primary 13 (92.9%) 1 (7.1%) 14
Revision 2 (1 0 0 % ) 0 (0.0%) 2 Total 15 (93.8%) 1 (6.2%) 16
Table 4. Postoperative complications of the endoscopic dacr- yocystorhinostomy
Complication Number of cases
Synechia 2 Granulation tissue 1
Synechia+granulation tissue 1
Total 4
the method requires careful application in cases involving the lateral-side bony fragment of the lacrimal sac because of the possibility of damaging the orbit. The mallet sh- ould move in an outside-to-inside direction in these sit- uations. When removing the upper part of the lacrimal sac, however, the mallet should go in a upside-to-downside direction to prevent damage to the cribriform plate. An Nd:YAG laser, or a contact laser when incising the nasal mucosa or the lacrimal sac, widens the operating view without increasing bleeding and facilitates precise incision and expansion of the site, which in turn helps exact placement of the silicon stent.8) But lasers should be carefully operated because of the possibility of dam- age to the orbit.8)9) In this study, we used an Nd:YAG laser in six cases to incise the lacrimal sac without cau- sing any damage to the orbit. The disadvantages of using laser include its high cost and the possibility of burning the surrounding mucosa and causing granulation tissue formation. Technical challenge is another short-coming of laser use.10) In four cases in our study, the epiphora was apparently caused by a medial maxillectomy to treat inverted papilloma. We obtained successful results in th- ese four cases by probing the medial wall of the lacrimal sac with the use of an Nd:YAG laser and making an opening through which to insert the silicon stent. Because most of the lacrimal bone had already been removed during the medial maxillectomy, there was no need for us to operate at this site and only a local anesthesia was necessary. Regarding the duration of the silicon stent insertion, Pak et al.,11) has reported that six weeks is su- fficient, since granulation tissue begins to form six weeks postoperatively. Metson et al.,12) report waiting for two to six months, while Massaro et al.,13) report leaving the stent for six months after the operation. In our exp- erience, how long the tube is maintained should depend on the condition of the patient, and in situations where this means a duration exceeding six weeks, it should be remembered that the chances of granulation tissue for- mation increase. When granulation is found during the follow-up period, removal of the granulation tissue, sh- ort-term steroid therapy and spraying with a steroid be- fore removal of the tube are considered to be effective ways of preventing restenosis. As a way to reduce the formation of granulation tissue at the openings, a me- thod of coating mitomycin may be used, but this was not attempted in our study. Postoperative complications
may include granulation tissue formation at the openings, restenosis due to adhesion of the middle turbinate and surrounding tissues, orbital complication, repeated dac- ryocystitis, and intracranial complication.10)13) Endoscopic endonasal dacryocystorhinostomy’s success rate has been reported to be 80-82% in primary cases14)15) and 75- 83% in revision cases.7)14) In this study, no recurrence was found during the follow-up period in all cases, su- ggesting a success rate competitive with that of external dacryocystorhinostomy and indicating the procedure to be an effective method of treating nasolacrimal duct obstruction in areas below the lacrimal sac.
CONCLUSION
According to the results of this study, endonasal dac- ryocystorhinostomy carries a success rate that places it on par with external approach. In light of this finding, we consider the endoscopic procedure to be an effective alternative to external dacryocystorhinostomy when tr- eating for nasolacrimal duct obstruction in areas below the lacrimal sac.
REFERENCES
1) Becker BB, Berry FD. Balloon catheter dilatation in pediatric pa- tients. Opthalmic Surg 1991;22:750-2.
2) Song HY. Recent treatment of the nasolacrimal duct obstruction. J Korean Med Assoc 1996;36:742-8.
3) Bumsted RM, Lindberg Ⅳ. External dacryocystorhinostomy. Arch Otolaryngol 1982;108:303-7.
4) McDonogh RM, Meiring H. Endoscopic transnasal dacryocystor- hinostomy. J Laryngol Otol 1989;103:585-7.
5) Rice DH. Endoscopic intranasal dacryocystorhinostomy: Results in four patients. Arch Otolaryngol Head Neck Surg 1990;116:1061.
6) Sprekelson MB, Barberan MT. Endoscopic dacryocystorhinostomy:
Surgical technique and results. Laryngoscope 1996;106:187-9.
7) Metson R. The endoscopic approach for revision dacryocystorhin- ostomy. Laryngoscope 1990;100:1344-7.
8) Mickelson SA, Kim DK, Stein IM. Endoscopic laser-assisted dac- ryocystorhinostomy. Am J Otolaryngol 1997;18:107-11.
9) Kang IB, Kim ST, Kim CW, Park BH, Jang IH, Cha HE. Endosc- opic laser dacryocystorhinostomy. Korean J Otolaryngol 1998;41:
746-9.
10) Park JH, Lee SD, Lee YB, Lee JH, Lee KC. Endoscopic laser dacryocystorhinostomy. Korean J Otolaryngol 1993;36:933-9.
11) Park JH, Lee JH, Kim BH, Lee SD, Lee YB. Endoscopic laser da- cryocystorhinostomy and silicon tube. Korean J Otolaryngol 1994;
37:531-4.
12) Metson R. Endoscopic surgery for lacrimal obstruction. Otolaryngol Head Neck Surg 1991;104:473-9.
13) Massaro BM, Gonnering RS, Jarris GJ. Endoscopic laser dacryoc- ystorhinostomy. Arch Ophthalmol 1990;108:1172-6.
14) Mannor GE, Millman AL. The prognostic value of preoperative dacryocystography in endoscopic intranasal dacryocystorhinostomy.
Am J Ophthalmol 1992;113:134-7.
15) Woog JJ, Metson R, Puliafito CA. Holmium: YAG endonasal laser dacryocystorhinostomy. Am J Ophthalmol 1993;116:1-10.